w w w . r b o . o r g . b r
Original
Article
How
to
classify
plantar
plate
injuries:
parameters
from
history
and
physical
examination
夽
Caio
Nery
a,
Michael
Coughlin
b,
Daniel
Baumfeld
c,
Fernando
Raduan
a,
Tania
Szejnfeld
Mann
a,
Fernanda
Catena
a,∗aEscolaPaulistadeMedicina,UniversidadeFederaldeSãoPaulo,SãoPaulo,SP,Brazil bSaintAlphonsusFootandAnkleClinic,Boise,ID,UnitedStates
cHospitalFelícioRocho,BeloHorizonte,MG,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received21April2014 Accepted27May2014
Availableonline26October2015
Keywords:
Hammertoesyndrome Acquiredfootdeformities Metatarsophalangealjoint
a
b
s
t
r
a
c
t
Objective:Tofindthebestclinicalparametersfordefiningandclassifying thedegreeof plantarplateinjuries.
Method:Sixty-eightpatients(100metatarsophalangealjoints)wereclassifiedinaccordance withtheArthroscopicAnatomicalClassificationforplantarplateinjuriesandweredivided intofivegroups(0toIV).Theirmedicalfileswerereviewedandtheincidenceofeach
param-eterfortherespectivegroupwascorrelated.Theseparameterswere:useofhighheels, sports,acutepain,localedema,Mulder’ssign,wideningoftheinterdigitalspace,painin theheadofthecorrespondingmetatarsal,touchingtheground,“drawertest”,toegripand toedeformities(inthesagittal,coronalandtransversalplanes).
Results:Therewerenostatisticallysignificantassociationsbetweenthedegreeofinjuryand useofhigh-heelshoes,sportstrauma,painattheheadofthemetatarsal,Mulder’ssign, deformityinpronationordisplacementinthetransversalandsagittalplanes(although theircombination,i.e.“crosstoe”,showedastatisticallysignificantcorrelation).Positive correlationswiththeseverityoftheinjurieswerefoundinrelationtoinitialacutepain, progressivewideningoftheinterdigitalspace,lossof“touchingtheground”,positiveresults fromthe“drawertest”onthemetatarsophalangealjoint,diminishedgripstrengthandtoe deformityinsupination.
Conclusions:The“drawertest”wasseentobethemorereliableandprecisetoolfor classi-fyingthedegreeofplantarplateinjury,followedby“touchingtheground”androtational deformities.Itispossibletoimprovetheprecisionofthediagnosisandthepredictionsofthe anatomicalclassificationforplantarplateinjuriesthroughcombiningtheclinicalhistory anddatafromthephysicalexamination.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
夽
WorkdevelopedintheFootandAnkleMedicineandSurgerySector,DepartmentofOrthopedicsandTraumatology,EscolaPaulistade Medicina,UniversidadeFederaldeSãoPaulo(UNIFESP),SãoPaulo,SP,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](F.Catena). http://dx.doi.org/10.1016/j.rboe.2015.10.009
Como
classificar
as
lesões
da
placa
plantar:
parâmetros
de
história
e
exame
físico
Palavras-chave:
Síndromedodedodopéem martelo
Deformidadesadquiridasdopé Articulac¸ãometatarsofalângica
r
e
s
u
m
o
Objetivo: Encontrarosmelhoresparâmetrosclínicosparadefinireclassificarograudas lesõesdaplacaplantar.
Método: Foramclassificados68pacientes(100articulac¸õesmetatarsofalângicas[MTF])de acordocomaclassificac¸ãoanatômicaartroscópicaparalesãodeplaca plantare dividi-dosemcincogrupos(0aIV).Seusregistrosmédicosforamrevisadosesecorrelacionou
aincidênciadecadaparâmetronorespectivogrupo.Osparâmetrosforam:usodesaltos altos,esportes,doraguda,edemalocal,sinaldeMulder,alargamentodoespac¸o interdigi-tal,dornacabec¸adometatarsocorrespondente,toqueaosolo,“testedagaveta”,preensão dosdedosedeformidadesdosdedos(planosagital,coronaletransversal).
Resultados: Nãohouveassociac¸ãoestatisticamentesignificativaentreograudelesãoeo usodesapatosdesaltoalto,traumaesportivo,dordecabec¸adometatarso,sinaldeMulder, deformidadeempronac¸ão,desvionoplanotransversalesagital(emboraasuacombinac¸ão, ocrossovertoe,tenhamostradocorrelac¸ãoestatisticamentesignificativa).Acorrelac¸ão pos-itivacomaseveridadedaslesõesfoiencontradaem:dor agudanoinício,alargamento progressivodoespac¸ointerdigital,perdade“toqueaosolo”;positividadedo“testedegaveta” daMTF;diminuic¸ãodaforc¸adepreensãoedeformidadeemsupinac¸ãododedo.
Conclusões: O“testedegaveta”seapresentacomoaferramentamaisconfiáveleprecisa paraclassificarograudalesãodaplacaplantar,seguidopelo“toqueaosolo”eas deformi-dadesrotacionais.Épossívelmelhoraraprecisãododiagnóstico,bemcomoaprevisãoda classificac¸ãoanatômicadelesãodaplacaplantar,pormeiodacombinac¸ãodehistóriaclínica ededadosdeexamefísico.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Instability of the metatarsophalangeal (MTP) joints of the smallertoesisacommonclinicalentity,butitisoftennot diag-nosedintheconsultationoffice.Severalauthorshavestated thattheplantarplateperformsthemainroleinmaintaining joint stabilityin thesagittal plane.1–4 Insufficiencyor
tear-ingoftheplantarplatetendstoevolvewithsomedegreeof deformity,inassociationwithahighpossibilityofsignsand symptoms.Themaincomplaintsamongthesepatientsare painintheforefootandsomedegreeofdeformity.1–5
DuVries apud Smith and Coughlin6 observed that the
second MTP was the joint that mostcommonly presented subluxationintheforefoot.Thedeformitymaypresent multi-planarvariance,butmorefrequentlyconsistsofattenuationof thelateralcollateralligamentinassociationwithinjurytothe lateralportionoftheplantarplate,thuscausingdorsomedial subluxationoracrossovertoe.1,3,7,8
Manyauthorsoverthelasttwodecadeshavereportedthat insufficiencyoftheplantarplateistheprimarypathological findingsthatleadtoinstability,9–12 but itwasonlyrecently
suggestedthat this structureshould be the mainfocus in surgicaltreatment.1,13,14 Coughlinetal.10 describedastudy
oncadaversaffectedbyacrossed-oversecondtoe.Dissection demonstrated anatomical alterations inthe MTP joint and thepresenceofplantarplateinjuriesthatformedapattern. They reported that in this case series, all the 16 cadavers had a transversal lesion adjacent to the insertion of the
plantar plate, atthe baseof the proximal phalanx, which variedinlengthfrom33%to100%alongtheinsertionarea. Intrasubstantial lesions,lesions of the collateral ligaments andcompletetearsoftheplantarplatewerefoundincases ofdeformitiesofgreaterseverity.Itwasconcludedthatthe plantar plate was the main element in deformities of the smaller toes. Since these authors were studying samples presentingcrossovertoe,whichisknowntobetheadvanced stageofthedeformity,theydidnotmentiontheanatomyor otherfindingsrelatingtothemildandmoderatestages.
The clinical symptoms and physical findings among patientswithplantarplateinjuriestotheMTPjoints,along withtheactivitiesandhabitsassociatedwiththiscondition, havebeendescribedbydifferentauthors,butcontroversystill surroundstheimportanceandsignificanceofeachofthese factors.Thus,thishasstimulatedmanyresearcherstostudy thephysiopathologyofthisdeformity,inanattempttoclassify thelesions.ThompsonandHamilton15proposeda
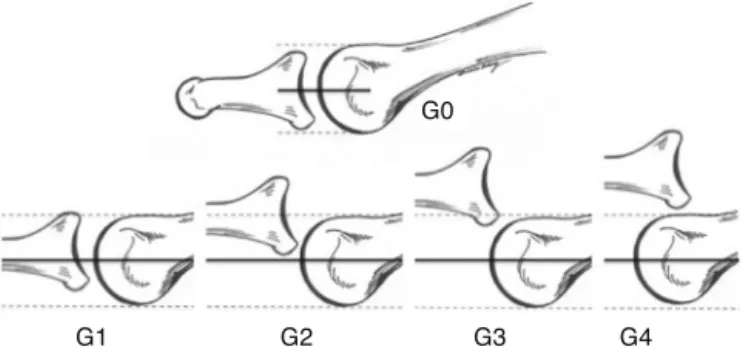
classifica-tionsystembasedonthelevelofsubluxationoftheproximal phalanxduringthe“drawertest”(Fig.1).Thistestwasalso usedasoneoftheparametersintheclinicalstagingsystemfor jointinstabilitythatwasproposedbyCoughlinetal.1(Table1).
Thisclassificationsystemalsotakesinto consideration the parametersofpainintheMTP,alignment,toegripandfeelings ofswellingintheforefoot.
The anatomical classification system for plantar plate injuriesthatwasproposedpreviouslygradeslesionsaccording totheirlocationandseverity.1Ithasbeensuggestedbysome
G1 G2 G3 G4 G0
Fig.1–Hamilton–Thompsonmetatarsophalangeal“drawer test”:G0,stablejoint;G1,mildinstability
(subluxation<50%);G2,moderateinstability
(subluxation>50%);G3,severeinstability(capacityforjoint dislocation);G4,dislocatedjoint.
parameters.However,sofar,noanalyticalstatisticalstudies definingtherelationshipbetweeneachtypeoflesionanda specificclinicalfindinghavebeenconducted.
Theobjectiveofthisstudywastodetermineclinical param-eters ofgreater reliability fordefining and grading plantar plateinjuries.Wehopethatthroughamoreaccurate diagno-sis,analgorithmencompassingtreatmentoptionsforallthe differentdegreesofplantarplateinjuriestotheMTPjointsof thesmallertoescanbeestablished.
Material
and
method
Between January 2009 and January 2012, 82 patients pre-sentingpainand sometypeofdeformityand/or instability oftheMTPjointswereobservedprospectively.Inaccordance withthe inclusion and exclusion criteria, 14patients were rejectedforthisstudyand68patients(100MTPjointsofthe smallertoes)were includedand treated.Ofthese,49 (72%) werewomenand19weremen(28%).Theirmeanageatthe startofsymptomswas61 years(range:40–78).Thesecond MTPwastheonemostcommonlyaffected,in63cases(63%), followedbythethirdin34cases(34%)andthefourthinthree cases(3%).
Theinclusion criteriaused comprisedpain inthe adult forefoot,withorwithoutdeformitiesofthehalluxorsmaller toes,andwithorwithout callosities.Theexclusioncriteria comprised presence of systemic comorbidities (especially
Table2–Clinicalparametersusedinthisstudy.
Type Parameter
History Acutepainatoutsetofcondition Sports-relatedtrauma
Useofhighheels Feelingoflocaledema Physicalexamination Increaseinspacebetweentoes
Touchingtheground
Painonplantarpalpationofthe correspondingmetatarsalhead Positive“drawertest”a Negativeplantargripb Mulder’ssign Displacementoftoec
a GradingofHamilton–Thompsontest:G0=stablejoint;G1=mild
instability(subluxation<50%);G2=moderateinstability (sublux-ation>50%);G3=severeinstability(capacityforjointdislocation); G4=dislocatedjoint.
b Bouche’splantargriptest:0=absent;1=diminished;2=normal.
c Displacementoftoeaccordingtotheplanes:axial(varus/valgus);
frontal (supination/pronation); sagittal (dorsal/plantar); combined–crossovertoe.
diabetes mellitus and rheumatoid arthritis); previous sur-gical treatmenton thefoot orankle;infectiousor vascular diseases;andanyotherpathologicalconditionofthefootor ankle thatmightcause misalignmentorpainfulconditions intheforefoot.
Theprojectforthisstudy wassenttothe localresearch ethicscommitteeandwasapproved.Allthepatientsinvolved gavetheiragreementtothefreeandinformedconsent state-mentofthisstudy.
Beforethesurgicaltreatment,allthepatientsunderwent assessment oftheir clinical history and complete physical examinations.Basedonpreviousreportsofcommon symp-toms andthe maindifferential diagnoses forplantar plate injuries,someparameterswereselectedforanalysis(Table2). Theseweretheparametersthatweremostpopularandhad beenmostfrequentlymentionedbyauthorsintheliterature onthistopic.1,4–6,8,10,16
Dataonthefollowingparametersweregathered:
Plantar grip: The patient’s toe grip was evaluated in a testusingastripofpaper,describedasa“paperwithdrawal test”.9,11Withthepatientstanding,anarrowstripofpaperof
1cminwidthby8cminlengthwasplacedunderthetoethat wastobetested,andthepatientwasthenaskedtogripthe
Table1–ClinicalstagingsystemforinstabilityoftheMTPjoints.
Grade0–MTPaligned;prodromicstagewithpain,butno deformity
JointpaininMTP;thickeningoredemaoftheMTPjoint; diminishedplantargrip;negativedrawertest
GradeI–mildMTPjointdisplacement;wideningofspacebetween
toes,medialdisplacement
PainintheMTPjoints;jointswelling;diminishedplantargrip; mildlypositive“drawertest”(subluxation<50%)
GradeII–moderatedisplacement;medial,lateral,dorsalor
dorsomedialdeformity;hyperextensionoftoe
Jointpain;notmuchedema;negativeplantargrip;moderately positive“drawertest”(subluxation>50%)
GradeIII–severedisplacement;dorsalordorsomedialdeformity; secondtoemayoverlaponhallux;flexibletoeclawingmaybe present
Paininjointsandfeet;notmuchswelling;negativeplantargrip; verypositivedrawer(MTPjointsdislocated);flexibletoeclawing
GradeIV–dorsomedialordorsaldisplacement;severedeformity
withdislocation;fixedtoeclawing
paperstriponthegroundandtrytostoptheexaminerfrom pullingitaway.Whenthepatientwasabletokeepthepaper stripunderhistoe,thetestwasconsideredpositive.Whenthe patientonlypartiallyresistedthisforce,thegripwas consid-eredtobediminished.Whennogripforcewasappliedandthe paperwaseasilywithdrawn,thetestwasconsideredtobe neg-ative.Inthepresentstudy,allthe“diminished”and“negative” resultsweregroupedas“negativeplantargrip”.
Jointstability:ThestabilityoftheMTPjointswas deter-minedbymeans ofthe“drawertest”.WiththeMTPunder evaluationextendedat25◦, averticalforce movementwas
applied.Theresultswere classifiedinaccordance withthe clinicalstagingsystem,usingascale from0to4:0=stable joint;1=mildinstability(subluxation<50%ofthejoint sur-face);2=moderateinstability(subluxation>50%ofthejoint surface);3=severeinstability(jointwithcapacityfor disloca-tion);4=dislocatedjoint.9
“Touchingtheground”test:Withthepatientinanupright standingposition,thesituationinwhichthetoetouchedthe groundinanormalmanner(i.e.causingaroundedtoeprint throughcontactbetweenthetipofthetoeandtheground) wasconsideredtobepositive.
After all the positive physical findings had been docu-mented,imagingstudieswereperformedonallthepatients, including radiographyand magneticresonance imaging.In thismanner,itwaspossibletodeterminethedegreeof defor-mityandinferthetypeofinjurytotheplantarplateinthe MTPjoints.
ThearthroscopicprocedureontheMTPwasdoneasthe firststageoftheoperationselectedforeachpatient,andnever asaseparateprocedure.TheMTPjointwasaccessedusinga 2.7mmarthroscopeinclinedat30◦,throughtwodorsalportals
(medialandlateral)abovethejointspace.Withslighttraction onthetoe,thecentralanddistalportionsoftheplantarplate couldbeviewed,inspectedandthenpalpatedusingaprobe. Synovectomywasperformedonthejointaffectedand, follow-ingthis,theplantarplateinjurywasgraded.Thefindingsfrom thephysicalexaminationandtheradiologicalandmagnetic resonanceimageswerethencorrelatedwiththearthroscopic findings(whichwereusedasthegoldstandard),inorderto definitivelydeterminethetypeofplantarplateinjuryinour patients. Systemicanalysis onthese arthroscopic discover-iesprovideduswithimportantinformationthatallowedus toputforwardasuggestionforananatomicalclassification system(Table3).Theresultsfromtreatingthesepatientswill bethesubjectofanotherarticle,inwhichthesurgical treat-mentperformedonthedifferentplantarplateinjurieswillbe explained.
For the firsttime inthe literature,positive clinicaldata frompatients’historiesandphysicalexaminationswere cor-relatedinthisstudywitharthroscopicfindingsfromtheMTP joints.Datagatheredprospectivelyweresubjectedto statis-ticalanalysisinordertodeterminewhethertherewasany significanceincorrelationsbetweenthepreoperativefindings andtheanatomicalgradesoftheplantarplateinjuries.
Wedivided the variables according tothe groups stud-ied(gradesoftheplantarplateinjuries),inordertoproduce descriptivestatistics:mean,standarddeviation(SD),median, minimumandmaximumnumericalvariablesandrelativeand absolutefrequencies(%),forthecategoricalvariables.
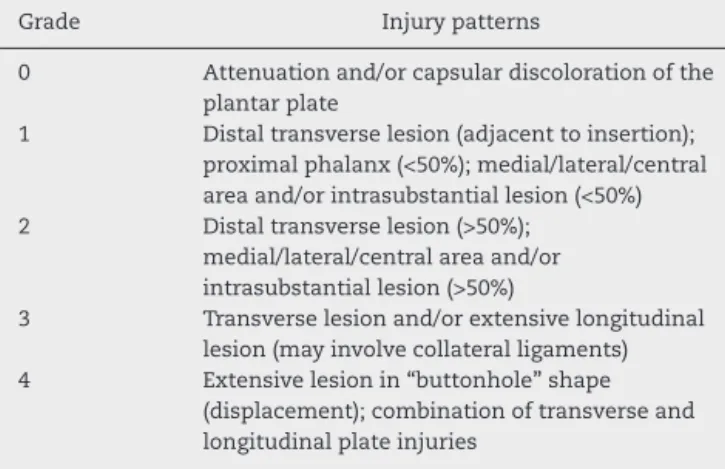
Table3–Anatomicalgradingofplantarplateinjuries.
Grade Injurypatterns
0 Attenuationand/orcapsulardiscolorationofthe plantarplate
1 Distaltransverselesion(adjacenttoinsertion); proximalphalanx(<50%);medial/lateral/central areaand/orintrasubstantiallesion(<50%) 2 Distaltransverselesion(>50%);
medial/lateral/centralareaand/or intrasubstantiallesion(>50%)
3 Transverselesionand/orextensivelongitudinal lesion(mayinvolvecollateralligaments) 4 Extensivelesionin“buttonhole”shape
(displacement);combinationoftransverseand longitudinalplateinjuries
Tocomparepairsofgroupsindependently,thettestandthe
nonparametricMann–WhitneyUtestwereapplied.To
com-parethreeormoreindependentgroups,analysisofvariance
(ANOVA)wasusedwithafixedgroupfactor,complemented
withBonferronimultiple-comparisontest;andalsothe non-parametricKruskal–Wallistest,complementedwiththeDunn multiple-comparisontest,ifstatisticallysignificantpvalues werefound.Associationsbetweenthegroupsstudiedandthe categoricalvariableswereanalyzedusingPearson’schi-square testorthelikelihoodratiochi-squaretest.
Theanalyses on all the statisticaldata were performed
usingSPSSforWindows,version18.0.Weusedthesignificance levelof5%,andpvaluesbelowthislevelwereconsideredto bestatisticallysignificantandwereidentifiedwithanasterisk (*).
Results
Morethantwothirdsofthepatientspresentedahistoryof acutepainintheMTPjointsofthesmallertoes(Table4).There wasastatisticallysignificantassociationbetweenthegrade oftheplantarplateinjuryandthissymptom(p=0.0005).We foundapositivecorrelationbetweenthegradeoftheplantar plateinjuryandthepresenceofacutepain,withtheexception ofgradeIV,inwhichthepercentageofpatientswithpainin thisjointbecamedrasticallyreduced.
Trauma associatedwith sports activity did notseem to playany importantroleinthe genesisoftheplantarplate injuriesinoursample,andtherewasnostatistically signifi-cantdifferencebetweenthegroupsstudied,inrelationtothis parameter(p=0.4546).Likewise,asubjectivefeelingofedema wasreportedbysomepatients,withoutpredominanceofany group(p=0.0927).
A highpercentageofthe patients (68%)correlated their plantarplateinjurieswithuseofhigh-heeledshoes.Although 83%oftheindividualswithgradeIinjuriesmadesuchreports, therewasnostatisticalsignificanceinrelationtothetypesof plantarplateinjury(p=0.2910).
Table4–Clinicalhistoryparametersaccordingtoinjurygrades.
History Grade(plantarplateinjury) Total(n=100)
0(n=23) I(n=12) II(n=15) III(n=33) IV(n=17)
Acutepain–n(%)
No 10(43.5%) 4(33.3%) 3(20.0%) 3(9.1%) 11(64.7%) 31(31.0%)
Yes 13(56.5%) 8(66.7%) 12(80.0%) 30(90.9%) 6(35.3%) 69(69.0%)
p 0.0005
Traumafromsports–n(%)
No 18(78.3%) 10(83.3%) 11(73.3%) 29(87.9%) 16(94.1%) 84(84.0%)
Yes 5(21.7%) 2(16.7%) 4(26.7%) 4(12.1%) 1(5.9%) 16(16.0%)
p 0.4546
Useofhighheels–n(%)
No 9(39.1%) 2(16.7%) 7(46.7%) 11(33.3%) 9(52.9%) 38(38.0%)
Yes 14(60.9%) 10(83.3%) 8(53.3%) 22(66.7%) 8(47.1%) 62(62.0%)
p 0.2910
Localedema–n(%)
No 18(78.3%) 5(41.7%) 9(60.0%) 17(51.5%) 13(76.5%) 62(62.0%)
Yes 5(21.7%) 7(58.3%) 6(40.0%) 16(48.5%) 4(23.5%) 38(38.0%)
p 0.0927
boththepatients’impressionsandthephysician’sobjective confirmationthattherereallywasagreaterdistancebetween thetoes,whenthepatientwasstanding.Amongthepatients ofthiscohort, 77%presentedthis characteristic.Therewas asignificantdifferenceintheincidenceofthis characteris-ticbetween the injury grades, such that open toes clearly
predominated at the more advanced stages of the injury
(p=0.0127).
Incapacity ofthe toes to touch the groundin anormal
manner when the patient is standing up (touching the
ground) is an important physical finding among patients
withplantarplateinjuries.Attheearlystages,almosthalfof
Table5–Physicalexaminationparametersaccordingtoanatomicalgradeofplantarplateinjuries.
Physicalexaminationparameters Grade(Plantarplateinjury) Total(n=100)
0(n=23) I(n=12) II(n=15) III(n=33) IV(n=17)
Separationoftoes
Absent 8(34.8%) 5(41.7%) 3(20.0%) 7(22.2%) 0(0%) 23(23.0%)
Present 15(65.2%) 7(58.3%) 12(80.0%) 26(78.8%) 17(100%) 77(77.0%)
p 0.0127
Touchingtheground–n(%)
Negative 9(39.1%) 6(50.0%) 14(93.3%) 32(97.0%) 16(94.1%) 77(77.0%) Positive 14(60.9%) 6(50.0%) 1(6.7%) 1(3.0%) 1(5.9%) 23(23.0%)
p <0.0001
Painundermetatarsalhead–n(%)
Absent 1(4.3%) 2(16.7%) 0(0%) 3(9.1%) 0(0%) 6(6.0%)
Present 22(95.7%) 10(83.3%) 15(100%) 30(90.9%) 17(100%) 94(94.0%)
p 0.1814
“Drawertest”–n(%)
I 23(100%) 11(71.6%) 49(60.0%) 15(35.4%) 0(0%) 58(58.0%)
II 0(0%) 1(8.3%) 6(40.0%) 14(42.4%) 6(35.3%) 27(27.0%)
III 0(0%) 0(0%) 0(0%) 4(12.1%) 5(29.4%) 9(9.0%)
IV 0(0%) 0(0%) 0(0%) 0(0%) 6(35.3%) 6(6.0%)
p <0.0001
Plantargrip–n(%)
Absent 10(43.5%) 10(83.3%) 14(93.3%) 32(97.0%) 15(88.2%) 81(81.0%)
Diminished 11(47.8%) 0(0%) 0(0%) 0(0%) 0(0%) 11(11.0%)
Normal 2(8.7%) 2(16.7%) 1(6.7%) 1(3.0%) 2(11.8%) 8(8.0%)
p <0.0001
Mulder’ssign–n(%)
Present 5(21.7%) 3(25.0%) 4(26.7%) 9(27.3%) 5(29.4%) 26(26.0%) Absent 18(78.3%) 9(75.0%) 11(73.3%) 24(72.7%) 12(70.6%) 74(74.0%)
Fig.2–Podoscopicviewsoftwopatientswhowere includedinourstudy.A,touchingthegroundwithallthe smallertoes;B,secondandthirdtoesnegativefortouching theground.
thetoesexamined presentedthisfinding,but this percent-ageincreasedwithincreasing gradeofplantarplate injury (p<0.0001).Morethantwo-thirdsofthejointsincludedinthis study presentedthis characteristic,which was determined throughdirectviewingofpodoscopicimages(Fig.2).
Oneofthephysicalfindingsmostcorrelatedwithplantar plateinjurieswaspainonplantarpalpationoftheheadof themetatarsalaffected.Nodifferencewasshownbetweenthe injurygroups(p=0.1814),but94%ofthejointsincludedinthis studypresentedthissymptom.The“drawertest”ontheMTP jointshowedaclearandsignificantdifferencebetweenthe typesofplantarplateinjury(p<0.0001).
Thescalefrom0to4thatwasusedtoclassifythe“drawer test”ontheMTPpresentedapositivecorrelationwith increas-inggradesofplantarplateinjury,whichwastranslatedasa progressiveincreaseinthedegreeofdislocationastheplantar plateinjuryworsened.Allthejointsincludedinourstudy pre-sentedsomedegreeofinstability,asmeasuredusingthistest, and15%wereclassifiedasinstabilityofgradeIIIorIV (capa-bleofdislocationordislocated,respectively),onthescaleof ThompsonandHamilton).
Anotherimportantobservationinthephysical examina-tionwastheplantargriptestonthetoes,alsoknownasthe “paper-pullingtest”,asdescribedbyBoucheandHeit15(Fig.3).
Wefoundthattherewerestatisticallysignificantdifferences betweenthegradesofplantarplateinjury,withaclear reduc-tionintoestrengthasthelesionworsened(p<0.0001).Among allofourpatients,92%Ifthejointsstudiedpresentedthis find-ing.Mulder’ssign,whichisusedinthedifferentialdiagnosis forMorton’sneuroma,wasobservedinasmallpercentageof thecasesofourcohort.Nostatisticaldifferencewasfound betweenthedifferentgradesofplantarplateinjuriesandthis finding(p=0.9854).
Table6presentstheresultsfromthestatisticalanalysison thetoedisplacementsinthreedifferentanatomicalplanes. To evaluate these physical examination parameters, the
Fig.3–Plantargripofthetoes.
imaginary long axis of the toes was used in comparison with the imaginary long axis ofthe metatarsal (by means ofanarticulatedgoniometer),usingtheclassicalmannerof measuring angles within clinical orthopedics, both axially (varus/valgus)andsagittally(dorsal/plantar).Toevaluatethe displacementsinthefrontalplane(supination/pronation)the leveland inclinationofthenail wasused,withthepatient standing(Fig.4).
Displacementofthetoesintheaxialplanewasfoundto beverycommon (84%),buttherelationshipwiththegrade oftheplantarplateinjuryshowedlowstatisticalsignificance (p=0.0459),withoutcleardifferentiationbetweenthegroups (Table6).
Inthesagittalplane,93%oftheMTPjointsstudied pre-sented dorsal elevation,but withlowstatistical correlation (p=0.0352)forthedifferentgroups.Itwasimpossibletodefine anycleardifferencebetweenthem.
Table6–Deformitiesofthesmallertoes.
Deformitiesofthesmallertoes Grade(Plantarplateinjury) Total(n=100)
0(n=23) I(n=12) II(n=15) III(n=33) IV(n=17)
Varus/Valgus–n(%)
Absent 8(34.8%) 2(16.7%) 3(20.0%) 2(6.1%) 1(5.9%) 16(16.0%)
Present 15(65.2%) 10(83.3%) 12(80.0%) 31(93.9%) 16(94.1%) 84(84.0%)
p 0.0459
Dorsalelevation–n(%)
Absent 5(21.7%) 0(0%) 1(6.7%) 1(3.0%) 0(0%) 7(7.0%)
Present 18(78.3%) 12(100%) 14(93.3%) 32(97.0%) 17(100%) 93(93.0%)
p 0.0352
Crossovertoe–n(%)
Absent 13(56.5%) 2(16.7%) 4(26.7%) 3(9.1%) 1(5.9%) 23(23.0%)
Present 10(43.5%) 10(83.3%) 11(73.3%) 30(90.9%) 16(94.1%) 77(77.0%)
p 0.0004
Pronation–n(%)
Absent 23(100%) 12(100%) 15(100%) 29(87.9%) 17(100%) 96(96.0%)
Present 0(0%) 0(0%) 0(0%) 4(12.1%) 0(0%) 4(4.0%)
p 0.0560
Supination–n(%)
Absent 23(100%) 12(100%) 11(73.3%) 21(63.6%) 4(23.5%) 71(71.0%)
Present 0(0%) 0(0%) 4(26.7%) 12(36.4%) 13(76.5%) 29(29.0%)
p <0.0001
Pronationofthetoewasshowntobeararedeformity(4%), withoutanydifferencebetweentheclassesofplateinjury.On theotherhand,supinationseemedtobeanimportantfinding ingroupsII,III andIV withplantarplateinjuries,inaccordance
withthetendencyforworseningofthedeformities(p<0.0001).
Discussion
Chronic instability of the smaller MTP joints presents an
insidiousonsetofpain.6Thisinstabilityencompassesawide
spectrumofsignsandsymptoms,composedofsynovitis,toe displacement,subluxationand,subsequentlydislocation.In theinitialphases,makingadiagnosisofinsufficiencyofthe plantarplatemaybedifficult,becausethesymptomsmimic
Fig.4–Differentdegreesofdeformityofcrossovertoe.
other common pathologicalconditions, suchasinterdigital neuromaormetatarsalgia.1,11,17
However, early diagnosis of this injury provides better results.Kleinetal.4recentlyreportedontheparameters
pre-sentedinpatients’historiesandphysicalexaminationsthat had greatestspecificityand sensitivityandcomparedthese parameterswiththeintraoperativefindings.18
Inthepresentstudy,allthepatientsevaluatedpresented sometypeofinjurytotheplantarplate.However,therehave been noreportsofpatientswithlesionsofgrade0orwith attenuatedplantarplates.Norhavetherebeenany descrip-tions of the characteristics of plantar plate injuries from observationsduringintraoperativeevaluations.
Coughlin et al.1 proposed a clinical staging system for
instabilityofthesecondMTPjointandsuggestedthatthere mightbeadirectcorrectionwiththeanatomical classifica-tion system. Althoughtheir suggestion was based onlyon observations, without statistical analysis, we camea simi-larconclusioninthepresentstudy:patientswithinjuriesof gradesIIandIIIweretheoneswhomostcommonlypresented pain,whichindicatesthattherewasaclearworseningofthe clinicalconditionwithprogressionoftheplantarplateinjury. ThenumberofpatientswithgradeIVinjurieswhopresented conditionsofacutepainwassubstantiallysmallerthanthe numbersintheothergroups.Weinterpretthisfindingasthe resultofcompletetearingoftheadjacentsofttissues, includ-ing thelocalsensorynervefibers,inthefinal stagesofthe plantarplateinjury.
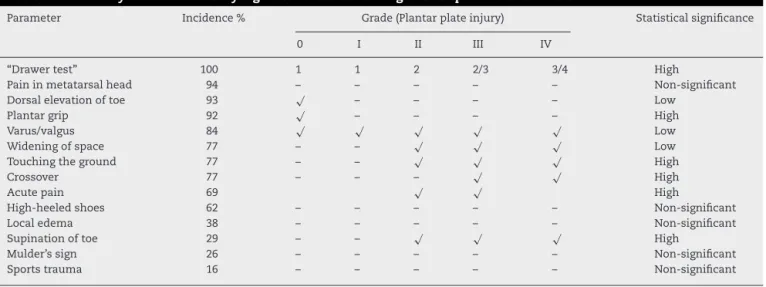
Table7–Summaryofthestatisticallysignificantresultsrelatingtoeachparameterstudied.
Parameter Incidence% Grade(Plantarplateinjury) Statisticalsignificance
0 I II III IV
“Drawertest” 100 1 1 2 2/3 3/4 High
Paininmetatarsalhead 94 – – – – – Non-significant
Dorsalelevationoftoe 93 √ – – – – Low
Plantargrip 92 √ – – – – High
Varus/valgus 84 √ √ √ √ √ Low
Wideningofspace 77 – – √ √ √ Low
Touchingtheground 77 – – √ √ √ High
Crossover 77 – – – √ √ High
Acutepain 69 √ √ High
High-heeledshoes 62 – – – – – Non-significant
Localedema 38 – – – – – Non-significant
Supinationoftoe 29 – – √ √ √ High
Mulder’ssign 26 – – – – – Non-significant
Sportstrauma 16 – – – – – Non-significant
anatomicalinjury,thefindingsfromthephysicalexamination alsoseemtoworsen.3,14,18,19
Basedonthestatisticalanalysispresentedhere,wewere abletoevaluateeachparameterstudiedinaccordancewith itsimportance,incidenceandstatisticalsignificance(Table7). Thephysicalcharacteristicofgreatestimportanceinourstudy wasthe“drawertest”ontheMTPjoints.Thistestwasdoneon allthejointswithplantarplateinjuries,withadirect correla-tionbetweenthemagnitudeoftheinstabilityandthegradeof theplantarplateinjury,whichwasdeterminedthroughhigh statisticalsignificance.This testwasthe mostreliable and precisetoolforclassifyingandgradingplantarplateinjuries beforethesurgery.
Afterthe“drawertest”,thenextcommonestfindingwas “painbelowthe metatarsal head”.Thissymptom wasvery commoninoursample(94%),butitdidnothavethecapacity todifferentiatebetweenthegroups.
Deformityconsistingofdorsalelevationofthetoeaffected wasanimportantclinicalfinding(93%)anditcorrelatedwith allgradesofplantarplateinjury,althoughitwassomewhat lessfrequentingrade0(attenuation).Thedegreeofdorsal elevationofthetoeincreasedwithworseningoftheplantar plateinjury,suchthatthismightevenbeawayofgradingthe severityoftheinjury.
Absenceordiminutionoftheplantargripcapacityofthe toewasobservedin92%ofourcases.Exceptforthelow per-centagedecreasein gripstrength amongthepatients with grade 0 injuries (48%), this parameter was not useful for differentiatingbetween other typesofplantar plate injury. Nevertheless,itwasavaluabletoolforverifyingthetreatment. Varus/valgusdisplacementwasfoundin84%ofthetoesin ourcohort.Itwaslessfrequentinthecasesofgrade0 defor-mityanditsincidencewasseentoincreasewithincreasing severityoftheplantarplateinjury.Thisdisplacementmaybe usefulfordifferentiatingbetweenthegradesofplantarplate injury.
Expansionofthespacebetweenthetoes,toesthatwould nottouchthegroundwhenthepatientwasstandingupand crossover toes (deformity in the sagittal and axial planes) appearedin77% oftheMTP jointsinthis study,and their
incidenceincreasedwithprogressionoftheinjury.Widening ofthespacebetweenthetoeswasseenmorefrequentlyin thegroupswithinjuriesofgradesII,IIandIV.Incapacityof toes to touch the ground showed a clear correlation with progressionoftheplantarplateinjuries,andcrossover defor-mitieswerecommonestingradesIIIandIV.Allofthesethree parameterscanbeusedastoolsfordifferentiatingbetween thegradesofplantarplateinjuries.Acutepainattheoutset ofthesymptomsappearedin69%ofourpopulation,butwas concentratedmainlyingradesIIandIII.Useofhigh-heeled shoeswasreportedby62%ofoursampleandtherewasno correlationwiththedifferentgroups.
Rotationaldeformityofthetoeinsupinationoccurredin only29%ofthetoesevaluatedinthisstudy,buttherewasa clearcorrelationbetweenthisobservationandworseningof theplantarplateinjuries.
Basedonthelackofstatisticalsignificanceandlow inci-denceoflocaledema(38%),Mulder’ssign(26%)andhistories ofsportstrauma (16%)inour sample,weconsideredthese parameterstobeoflesserimportancefordiagnosingand dif-ferentiatingplantarplateinjuries.
Conclusions
Itispossibletoimprovetheprecisionofthediagnosisandthe predictionoftheanatomicalgradeofplantarplateinjuries, throughcombiningtheclinicalhistoryandthedatafromthe physicalexamination.
Basedonourresults,thepreciseclinicaldescriptionofa plantarplateinjurytoaMTPjointshouldincludeacomplaint ofpainbelowtheheadofthemetatarsal affected,in asso-ciation with varying degreesof dorsal elevationand varus displacement ofthecorrespondingtoe,alsocombinedwith expansionofthespacebetweenthetoes.Morethanhalfof ourpatientsrecalledanepisodeofacutepainattheoutsetof theirsymptoms,possibleassociatedwithusinghigh-heeled shoes.
anatomicaltypeofplantar plate injury.This seemedto be thebesttoolforevaluatingthestabilityoftheMTPjoint.The abilityofthetoe totouchthe groundisgraduallylost asa resultofprogressionoftheinsufficiencyoftheplantarplate.
Fromourresults,wecansuggestthefollowing:
When a patient presents normally functioning toe strength,and there isno suspicion ofplantar plate injury despitethelocalpain,theinjuryisprobablyofgrade0.
Ifthetoetouchesthegroundinapatientwithapossible plantarplateinjury,thisisprobablyaninjuryofgrade0orI.
Supination of the affected toe appears injuries encom-passing>50%ofthe plantarplate(grade IIorhigher), with increasingprevalenceastheseverityoftheinjurybecomes greater.
Inthepresenceofseverecrossovertoedeformity,the plan-tarplateinjuryisprobablygradeIIIorIV.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. CoughlinMJ,BaumfeldDS,NeryC.SecondMTPjoint instability:gradingofthedeformityanddescriptionof surgicalrepairofcapsularinsufficiency.PhysSportsmed. 2011;39(3):132–41.
2. FrimenkoRE,LieversW,CoughlinMJ,AndersonRB,Crandall JR,KentRW.Etiologyandbiomechanicsoffirst
metatarsophalangealjointsprains(turftoe)inathletes.Crit RevBiomedEng.2012;40(1):43–61.
3. MyersonMS,JungHG.Theroleoftoeflexor-to-extensor transferincorrectingmetatarsophalangealjointinstabilityof thesecondtoe.FootAnkleInt.2005;26(9):675–9.
4. KleinEE,WeilL,WeilLS,CoughlinMJ,KnightJ.Clinical examinationofplantarplateabnormality:adiagnostic perspective.FootAnkleInt.2013;34(6):800–4.
5.BlitzNM,ChristensenJC,FordLA.Plantarplaterupturesof thesecondmetatarsophalangealjoint.JFootAnkleSurg. 2002;41(2):138–9.
6.SmithBW,CoughlinMJ.Disordersofthelessertoes.Sports MedArthrosc.2009;17(3):167–74.
7.DelandJT,SungIH.Themedialcrossovertoe:acadaveric dissection.FootAnkleInt.2000;21(5):375–8.
8.CoughlinMJ.Crossoversecondtoedeformity.FootAnkle. 1987;8(1):29–39.
9.CooperMT,CoughlinMJ.Sequentialdissectionforexposure ofthesecondmetatarsophalangealjoint.FootAnkleInt. 2011;32(3):294–9.
10.CoughlinMJ,SchuttSA,HiroseCB,KennedyMJ,GrebingBR, SmithBW,etal.Metatarsophalangealjointpathologyin crossoversecondtoedeformity:acadavericstudy.FootAnkle Int.2012;33(2):133–40.
11.DotyJF,CoughlinMJ.Metatarsophalangealjointinstabilityof thelessertoes.JFootAnkleSurg.2013.S1067-2516(13)00106-3. 12.JohnstonRB,SmithJ,DanielsT.Theplantarplateofthelesser toes:ananatomicalstudyinhumancadavers.FootAnkleInt. 1994;15(5):276–82.
13.BlitzNM,FordLA,ChristensenJC.Plantarplaterepairofthe secondmetatarsophalangealjoint:techniqueandtips.JFoot AnkleSurg.2004;43(4):266–70.
14.WeilL,SungW,WeilLS,MalinoskiK.Anatomicplantarplate repairusingtheWeilmetatarsalosteotomyapproach.Foot AnkleSpec.2011;4(3):145–50.
15.ThompsonFM,HamiltonWG.Problemsofthesecond metatarsophalangealjoint.Orthopedics.1987;10(1):83–9. 16.BouchéRT,HeitEJ.Combinedplantarplateandhammertoe
repairwithflexordigitorumlongustendontransferfor chronic,severesagittalplaneinstabilityofthelesser metatarsophalangealjoints:preliminaryobservations.JFoot AnkleSurg.2008;47(2):125–37.
17.FortinPT,MyersonMS.Secondmetatarsophalangealjoint instability.FootAnkleInt.1995;16(5):306–13.
18.NeryC,CoughlinMJ,BaumfeldD,MannTS.Lesser
metatarsophalangealjointinstability:prospectiveevaluation andrepairofplantarplateandcapsularinsufficiency.Foot AnkleInt.2012;33(4):301–11.