www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
Hearing
handicap
in
patients
with
chronic
kidney
disease:
a
study
of
the
different
classifications
of
the
degree
of
hearing
loss
夽
Klinger
Vagner
Teixeira
da
Costa
a,∗,
Sonia
Maria
Soares
Ferreira
a,
Pedro
de
Lemos
Menezes
a,baHospitalVida,CentroUniversitárioCESMAC,ProgramadePós-graduac¸ão,Maceió,AL,Brazil bUniversidadeEstadualdeCiênciasdaSaúdedeAlagoas,Maceió,AL,Brazil
Received17June2016;accepted7August2016 Availableonline10September2016
KEYWORDS
Chronickidney disease; Hearingloss; Audiometry
Abstract
Introduction:Theassociationbetweenhearinglossandchronickidneydiseaseand hemodial-ysishasbeenwelldocumented.However, theclassificationusedfor thedegreeoflossmay underestimatetheactualdiagnosisduetospecificcharacteristicsrelatedtothemostaffected auditory frequencies. Furthermore, correlationsofhearing loss andhemodialysistime with hearinghandicapremainunknowninthispopulation.
Objective:To compare the results of Lloyd’s and Kaplan’s and The Bureau Internacional d’Audiophonologieclassificationsinchronickidneydiseasepatients,andtocorrelatethe aver-agescalculatedbytheirformulaswithhemodialysistimeandthehearinghandicap.
Methods:This isan analytical, observationaland cross-sectional study with 80 patients on hemodialysis. Tympanometry, speech audiometry, pure tone audiometry and interview of patients with hearingloss throughHearing HandicapInventoryfor Adults. Cases were clas-sifiedaccordingtothedegreeofloss.Thecorrelationsoftoneaverageswithhemodialysistime andthetotalscoresofHearingHandicapInventoryforAdultsanditsdomainswereverified.
Results:86 ears (53.75%) had hearing loss in at least one of the tonal averages in 48 patientswho respondedtoHearingHandicapInventoryforAdults.TheBureauInternacional d’Audiophonologieclassificationidentifiedagreaternumberofcases(n=52)withsomedegree ofdisabilitycomparedtoLloydandKaplan(n=16).Inthegroupwithhemodialysistimeofat least2years,therewasweak butstatisticallysignificantcorrelationofTheBureau Interna-cionald’Audiophonologieclassificationaveragewithhemodialysistime(r=0.363).Therewere moderatecorrelations ofaverageThe BureauInternacionald’Audiophonologie classification (r=0.510)and tritone 2(r=0.470)with the total scoresof HearingHandicapInventory for Adultsandwithitssocialdomain.
夽 Pleasecitethisarticleas:CostaKV,FerreiraSM,MenezesPL.Hearinghandicapinpatientswithchronickidneydisease:astudyofthe
differentclassificationsofthedegreeofhearingloss.BrazJOtorhinolaryngol.2017;83:580---4.
∗Correspondingauthor.
E-mail:[email protected](K.V.Costa).
PeerReviewundertheresponsibilityofAssociac¸ãoBrasileiradeOtorrinolaringologiaeCirurgiaCérvico-Facial.
http://dx.doi.org/10.1016/j.bjorl.2016.08.008
Conclusion: TheBureauInternacionald’Audiophonologieclassificationseemstobemore appro-priatethanLloyd’sandKaplan’sforuseinthispopulation;itsaverageshowedcorrelationswith hearinglossinpatients withhemodialysistime≥2yearsanditexhibitedmoderatelevelsof correlationwiththetotalscoreofHearingHandicapInventoryforAdultsanditssocialdomain (r=0.557andr=0.512).
© 2016 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Published by Elsevier Editora Ltda. This is an open access article under the CC BY license (http://
creativecommons.org/licenses/by/4.0/).
PALAVRAS-CHAVE
Doenc¸arenalcrônica; Perdaauditiva; Audiometria
OHandicapauditivoempacientescomdoenc¸arenalcrônica:umestudo dasdiferentesclassificac¸õesdograudaperdaauditiva
Resumo
Introduc¸ão: Aassociac¸ãoentreperdaauditivaedoenc¸arenalcrônicaehemodiálisetemsido bemdocumentada.Porém, aclassificac¸ãoutilizadapara ograudaperdapodesubestimaro realdiagnósticodevidoacaracterísticasespecíficasemrelac¸ãoàsfrequênciasauditivasmais acometidas. Além disso, correlac¸ões da perda auditiva e do tempo de hemodiálise com o handicapauditivopermanecemdesconhecidasnessapopulac¸ão.
Objetivo: Compararosresultadosdasclassificac¸õesdeLloydeKaplanedoBureauInternacional d’Audiophonologieempacientescomdoenc¸arenalcrônicaecorrelacionarasmédiascalculadas porsuasfórmulascomotempodehemodiáliseecomohandicapauditivo.
Método: Estudoanalítico,observacionaletransversalcom80pacientesemhemodiálise.Todos ospacientesforamsubmetidosatimpanometria,logoaudiometria,audiometriatonallimiar,e ospacientescomperdaauditivaforamentrevistadosatravésdoHearingHandicapInventory forAdults.Aclassificac¸ãodoscasosfoifeitadeacordocomograudaperda.Foramverificadas ascorrelac¸õesdasmédiastonaiscomotempodehemodiáliseecomaspontuac¸õestotaisdo
HearingHandicapInventoryforAdultseseusdomínios.
Resultados: Em 48 pacientes que responderam ao Hearing Handicap Inventory for Adults, 86 orelhas (53,75%)apresentaram perdaauditiva em pelomenos uma dasmédias tonais.A Classificac¸ão doBureau Internacionald’Audiophonologieidentificoumaiornúmero decasos (n=52) que apresentavam algum grau de deficiência do que a classificac¸ão de Lloyd e Kaplan(n=16).Nogrupocomtempodehemodiáliseapartirdedoisanos,houvecorrelac¸ão fraca, masestatisticamentesignificante,damédia daclassificac¸ão doBureau Internacional d’Audiophonologiecomotempodehemodiálise(r=0,363).Houvecorrelac¸õesmoderadasdas médias da classificac¸ão do Bureau Internacional d’Audiophonologie (r=0,510) e tritonal 2 (r=0,470)compontuac¸õestotaisdoHearingHandicapInventoryforAdultsecomseudomínio social.
Conclusão:A classificac¸ão do Bureau Internacional d’Audiophonologie mostra-se mais ade-quada doqueadeLloyd eKaplannessapopulac¸ão,suamédiaapresentou correlac¸ões com perdas auditivasem pacientescomtempo dehemodiálise≥2anose manteveníveis mod-eradosdecorrelac¸ãocomapontuac¸ãototaldoHearingHandicapInventoryforAdultseseu domíniosocial(r=0,557er=0,512).
© 2016 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Publicado por Elsevier Editora Ltda. Este ´e um artigo Open Access sob uma licenc¸a CC BY (http://
creativecommons.org/licenses/by/4.0/).
Introduction
Currently, there are several classification scales of the degreeofhearinglossandtheirformulasconsiderdifferent hearingfrequenciestocalculatethetoneaverage.Thereis notyetconsensusonwhichscalebetterfitsthepatternof hearinglossoccurringinpatientswithchronickidneydisease (CKD)andhemodialysis(HD).
The best-known association between CKD and hearing lossisAlportSyndromewhichhasageneticcause.1However,
mosthearinglossesthatoccurinCKDarenotgenetic,and areduetoanatomical,physiological,pathologicaland phar-macologicalsimilaritiesbetweenthenephronandvascular
striaofthecochlea.2Theprevalenceofhearingimpairment
isgreaterin CKDthanin thegeneralpopulation,3evenin
children,4---7andisthemostsevereandsensorineuralintype
athighfrequencies.8---10
TheworldwideprevalenceofCKDhasincreasedinrecent decades.In 2013, 2.5 million patients wereon dialysisin theworld,andthisnumberisexpectedtoreach6.5million in2030.11 In2014, theestimated totalnumber ofdialysis
patientsinBrazilwas112,004,with91.4%beingonHD,and 8.6%onperitonealdialysis.12
(restrictionof participation)refers to the involvement in lifesituationsandshowstheindividual’sadaptationtothe environmentasaresultofhearinglossanddisability.13
Emotional andsocial damage fromhearingimpairment arevariableanddependonlifeexperiences,expectations related to health, and even on the adaptive capacity of theindividual. Thus, peoplewithsimilar hearingloss can experiencedifferentcommunicative, socialandemotional difficulties in daily life andhave differentperceptions of theirqualityoflife.14
HHIA Questionnaire (Hearing Handicap Inventory for Adults)isatooltoassesstheimpactofhearinglossbasedon theperceptionofhearinghandicap,andamongitsusesin clinicalpracticeistheabilitytoassesstheimpactofa ther-apeuticmeasure(e.g.hearingaids)andtoidentifyspecific treatmentneeds.15
As the hearing loss associated with CKD is more pro-nouncedathighfrequencies,theformulausedtocalculate the tone average can lead to different categorizations. Becauseof the importanceof high frequencies in speech intelligibility,it isnecessarytobetterunderstand the for-mulathatpossiblyhasassociationswithtimeofhemodialysis andwithhearinghandicap.Therewerenostudiesinthe lit-eratureevaluatinghearinghandicapin HDpatients.Thus, theobjectivesofthisstudyare:(1)tocomparetheresults ofLloyd andKaplanand BIAPclassifications,(2) to corre-latethetonalaveragescalculatedbytheformulasusedby thesetwoclassifications and tritonal formula of high fre-quencieswithhemodialysistime(HT)ingroupsofpatients witheither lessthan 2 yearsandwithat least 2 yearsof treatment,andfinally(3)tocorrelatetheseaverageswith hearinghandicap.
Methods
Thisisananalytical,observationalandcross-sectionalstudy. Thesampleconsistedof80patientsonHDforatleastthree months,withagesbetween14and54years.
TheprotocolofthisresearchisbasedonResolutionNo. 466/12 of the National Health Council of the Ministry of Healthforresearchwithhumansubjects,andwasapproved bytheResearchEthicsCommitteewithNo.1290310/2015. Thepatientsselectedwerethoseonregular hemodialy-sistreatmentinthecenterofnephrologyofahospitalwith public and private care. Inclusion criteria were: patients with CKD under the age of 55 and on HD for at least 3 months,while theexclusioncriteriawere:hearing lossof any etiology beginning before the CKD, transplantation, chronicearinfection,exposuretonoise,mentaldisability, anduse ofototoxicdrugs for more than1 week. Patients with normal otoscopy underwent tympanometry with an Interacoustics® brand immittanciometer, model at235 XP, serialnumber206331,contralateralTDH39handset, ipsilat-eralclinicalheadset;patientswithtympanogramofJerger type‘‘A’’ (1970) underwent speechaudiometry and Pure Tone Audiometry(PTA) in an audiometric 2m×2m cabin toassessthefrequenciesof0.25;0.5;1;2;4;6and8kHz withInteracoustics® audiometer, ac33 model, serial num-ber185994withbone vibratorb-71,TDH-39right andleft headphonesproperlycalibratedaccordingtostandardsISO 389-1 and ISO 389-3; PTA tests, speech audiometry and
imitanciometrytestswereperformedbythesamephysician in all cases. The following average values were calcu-lated with the formulas: tritone 1 average --- Lloyd and Kaplan(0.5,1and2kHz),quadritonalaverage---BIAP(0.5, 1, 2 and 4kHz) and tritonal 2 average (4, 6 and 8kHz). Hearing losseswereconsidered whenthethresholdof tri-tonalaverageswereabove25dBHL,andBIAPaveragewas above 20dB HLaccording to the Lloyd andKaplan (1978) andBIAP (1997)classifications, respectively.Patientswith losses of theseaverages wereinterviewed for completing the HHIAthat consistedof 25questionsquantifying social (12 questions) and emotional (13 questions) effects aris-ingfromhearinglossinindividualsyoungerthan65years. Therespondentisaskedtoanswer‘‘yes’’,‘‘sometimes’’or ‘‘no.’’A‘‘yes’’answerisworth4points,‘‘sometimes’’is worth2points,and‘‘no’’doesnotgetanypoints.Thescore ranges from 0 to100. The classificationfollows the total scoreofHHIA:noperceptionofhearinghandicap(0---16%), mild/moderateperception(18---42%)andsevere(above42%) perception.
Two groups of patients were created according to HT: GroupI(lessthan2years)andGroupII(2yearsorlonger). The correlations of the three tonal averages with hemodialysistimeinGroupsIandIIwerechecked. Corre-lationsofthethreetonalaverageswiththetotalscoresof HHIAandtheirdomainswerealsotested.
Statistical analysis was conducted usingthe Statistical Package for the Social Sciences --- SPSS version 21.0 for Windows®. The profile of hearingloss and the perception of hearinghandicapwereestablishedby applying descrip-tivestatisticstechniques,andtheresultswereexpressedin theformoftablesandillustrativechart.Thenormalitytest used was the Shapiro---Wilk. Correlations were performed usingbivariatecorrelationtest withdegreeoflinear rela-tionshipanalyzedbySpearmancoefficient.Differenceswere consideredsignificantfortheerrorvalueof˛=0.05.
Results
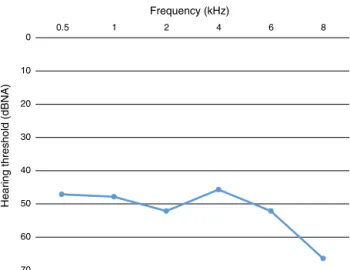
Thesampleconsistedof80patients(160ears)onHD,39men (48.75%) and41 women(51.25%). Eighty-sixears (53.75%) had hearing loss in at least one of the pure tone aver-agesin48patients(uni-andbilateralloss).The48patients responded to HHIA, 28 (58.3%) being male. HD average timewas50.50(±41.25)monthsofthesampleandofthe patients with hearing loss was 54.25 (± 52) months. The typeoflosswassensorineuralinallcases,andwithgreater impairmentofhighfrequencies(Fig.1).
Thetotalnumberofearswithlossesandthedistribution ofgradesaccordingtoLloydandKaplan,BIAPandtritone2 sensorineuralcanbeseeninTable1.
ThecorrelationtestbetweentritonalandBIAPaverages withHT inGroups Iand II wasperformed. In Group I,no correlationofaverageswithHTwasobserved.InGroupII, therewasaweak,butstatisticallysignificantcorrelationof BIAPaveragewithHT(Table2).
Forty-eightHHIA questionnaireswerefilledand 43.75% hadsomedegreeofhandicapperceptionwithatotal aver-ageof30.50---63.00(Table3).
Table1 TotalofearswithhearinglossandthedegreeaccordingtoLloyd’sandKaplan’sandBIAP’sclassifications.
Tonalaverages Earswith
hearingloss
Mild degree
Moderate degree
Severe degree
Profound degree
Cofosis
Tritonal1(0.5;1and2kHz) 16 13 2 0 1 0
BIAPaverage(0.5;1;2and4kHz) 52 47 4 0 1 0
Tritonal2(4.6and8kHz) 57 25 26 5 1 0
Table2 CorrelationsbetweenthetonalaveragesandthetimeofhemodialysisofGroupsIandII.
Averages GroupI GroupII
TH TH
Tritonal1average(0.5;1and2kHz) p=0.511;r=0.156 p=0.335;r=0.163 BIAPaverage(0.5;1;2and4kHz) p=0.801;r=0.060 p=0.027;r=0.363 Tritonal2average(4;6and8kHz) p=0.644;r=0.110 p=0.134;r=0.251
Table 3 Numberof cases, percentages, total averages and ofemotional andsocial domains according to thedegree of perceptionofhearinghandicapmeasuredbyHHIA.
Perception n % HHIAaverage HHIA(e)average HHIA(s)average
Noperception 27 56.25 6.00(±7.65) 3.5(±4.12) 9.00(±8.24)
Mild/moderateperception 17 35.41 30.50(±11.12) 15.50(±9.00) 15.00(±2.58) Severeperception 04 8.34 63.00(±7.57) 30.50(±2.51) 32.50(±5.98)
Total 48 100
HHIA,HearingHandicapInventoryforAdults;HHIA(e),emotionaldomain;HHIA(s),socialdomain.
Table4 Correlationsbetweentonalaverages(dBNA)withtotalscoresofHHIAanditsdomains.
Averages HHIA HHIA(e) HHIA(s)
Tritonal1averages(0.5;1and2kHz) p=0.108;r=0.344 p=0.468;r=0.159 p=0.025;r=0.466 BIAPaverages(0.5;1;2and4kHz) p=0.013;r=0.510 p=0.066;r=0.389 p=0.006;r=0.557 Tritonal2averages(4;6and8kHz) p=0.024;r=0.470 p=0.072;r=0.382 p=0.013;r=0.512
HHIA,HearingHandicapInventoryforAdults;HHIA(e),emotionaldomain;HHIA(s),socialdomain.
0
10
20
30
40
50
60
70
0.5 1 2 4 6 8
Hearing threshold (dBNA)
Frequency (kHz)
Figure1 Profileofhearinglossaccordingtoaveragehearing thresholdinfrequencies.
moderatecorrelationofquadritonalandtritonal2averages withtotalscoresofHHIAanditssocialdomain(Table4).
Discussion
There was a slight predominance of females in the sam-ple(51.25%),butmen(58.3%)predominatedamongpatients withhearingloss.TheaveragetimeofHDofpatientswith loss(54.25months)washigherthantheaveragesampletime (50.50months).
ofhighfrequenciesoccurs;BIAPclassificationprovedtobe theonethatbestrepresentsthedegree ofhearinglossin thispopulationwithlosseswiththisfeature.16
Sincethemostpronouncedhearinglossinhigh frequen-cies stands as a characteristic of loss in this population, theformulausedbyBIAPclassificationwasmore appropri-atethan theLloyd Kaplanbecause itconsidered the high frequenciesinitscalculation.
In Group I nocorrelation of any of the tonalaverages withHTwasobserved;however,in GroupII(HT≥2years) thelossesinBIAPaverageshowedcorrelationswiththeHT.It followsthatafter2yearsoftreatment,therewasagreater impactof factorsrelated toCKD/hemodialysisonhearing function,andthisisconsistentwithotherstudiesthathave shownthathearinglossmayoccurmorefrequentlyafter2 yearsofHD.17,18
Hearing handicap proved tobemild/moderatein most caseswithgreatsimilarityofscoresintheirfields.
Nolevelofcorrelationoftritonal1averagewithhearing handicap was observed. Lima et al.19 tested the
correla-tionsoftritonal1averagewithtotalHHIAandfoundweak butsignificantcorrelations(r=0.30);thesedatasuggestthat theclassificationofLloydandKaplanislimitedbecauseit doesnotreflect theimpairmentincommunicative perfor-mancegenerated by such losses in this population. Total HHIAshowedmoderatecorrelationswiththeaveragesthat considerthehighfrequencies(BIAPandtritonal2)andthe socialdomainportionoftheHHIA.Thisillustratesthe impor-tance of high frequencies in the intelligibility of words, especiallyforthesociallife.KielinenandNerbonne20
iden-tified poor correlations of the audiometric averages with hearinghandicap (r=0.41),but the correlationsimproved whentheaveragesincluded4kHzintheformula(r=0.55). Stewartetal.21 found ahighercorrelation of audiometric
average of frequencies of 1---4kHz with hearing handicap (r=0.678)thantheaverageofthefrequenciesof0.5,1and 2kHz(r=0.550);thesameauthorsstatethatprofessionals whousetonalaveragescalculatedfromhigherfrequencies tendtointerveneearlierinpopulationswithhearinglossat highfrequenciesthroughtheuseofsoundamplificationor otherauditoryrehabilitationproceduressuchasthoseusing formulasemploying0.5kHz.
Conclusion
In patients with hearing loss associated with CKD/ hemodialysis the BIAP classification seems to be more suitable since it allows a better categorization regarding thedegree of impairment.Itscalculated average through the quadritonal formula correlated with the duration of hemodialysisinpatientswith2ormoreyearsoftreatment, andhadmoderatecorrelationwiththetotalscoreofHHIA anditssocialdomain.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.AlportAC.Hereditaryfamilialcongenitalhaemorrhagic nephri-tis.BrMedJ.1927;1:504---6.
2.PandeyS,GoreG,ValameD,MehtaK.Audiometricprofilein patientswithchronicrenal failure.JOtolaryngolHead Neck Surg.2011;40:131---6.
3.ThodiC,ThodisE,DanielidesV,PasadakisP,VargemezisV. Hear-inginrenalfailure.NephrolDialTransplant.2006;21:3023---30.
4.ManciniML,DelloSL,BianchiPM,TieriL,RizzoniG. Sensorineu-ral hearing lossin patientsreachingchronic renal failure in childhood.PediatrNephrol.1996;10:38---40.
5.Nikolopoulos TP, KandilorosDC, Segas JV, Nomicos PN, Fer-ekidis EA, Michelis KE, et al. Auditory function in young patientswithchronicrenalfailure.ClinOtolaryngolAlliedSci. 1997;22:222---5.
6.SamirM,RiadH,MahgoubM,AwadZ,KamalN.Transient otoa-cousticemissionsin childrenwithchronic renal failure.Clin Otolaryngol.1998;23:87---90.
7.Stavroulaki P, Nikolopoulos TP, Psarommatis I, Apostolopou-losN.Hearingevaluationwithdistortion-productotoacoustic emissions in young patients undergoing haemodialysis. Clin OtolaryngolAlliedSci.2001;26:235---42.
8.AntonelliAR,BonfioliF,GarrubbaV,GhiselliniM,LamorettiMP, NicolaiP,et al.Audiologicalfindingsinelderlypatientswith chronicrenalfailure.ActaOtolaryngolSuppl.1991;476:54---68.
9.BazziC,VenturiniCT,PaganiC,ArrigoG,D’AmicoGD.Hearing lossinshort-andlong-termhaemodialysedpatients.Nephrol DialTransplant.1995;10:1865---8.
10.BendoE,Resuli M,MetaxasS.Hearingevaluationinpatients withchronicrenalfailure.JOAD.2015;4:51---3.
11.CAREFM.FreseniusMedicalCareAnnualReport2013.Fresenius MedCare.2014;294.
12.SessoRC,LopesAA,ThoméFS,LugonJR,MartinsCT.Brazilian chronicdialysiscensus2014.JBrasNefrol.2016;38:54---61.
13.HelvikA-S,JacobsenG,WennbergS,ArnesenH,RingdahlA, HallbergLR-M.Activitylimitationandparticipationrestriction inadultsseekinghearingaidfittingandrehabilitation.Disabil Rehabil.2006;28:281---8.
14.Aiello CP, Lima II, Ferrari DV. Validity and reliability of the hearinghandicapinventoryforadults.BrazJOtorhinolaryngol. 2011;77:432---8.
15.SacconePA,SteigerJR.Hearinghandicapamongadultresidents ofanurbanhomelessshelter.JHealthCarePoorUnderserved. 2007;18:161---72.
16.Kano CE, Mezzena LH, Guida HL. Estudo comparativo da classificac¸ãodograudeperdaauditivaemidosos institucional-izados.RevCEFAC.2009;11:473---7.
17.PeyvandiA,RoozbahanyNA.Hearinglossinchronicrenal fail-urepatientundergoinghemodialysis.IndianJOtolaryngolHead NeckSurg.2013;65:537---40.
18.Meena RS, Aseri Y, Singh BK, Verma PC. Hearing loss in patientsofchronicrenalfailure:astudyof100cases.Indian JOtolaryngolHeadNeckSurg.2012;64:356---9.
19.LimaIIde,AielloCP,FerrariDV.Correlac¸õesaudiométricasdo questionário de handicap auditivo para adultos. Rev CEFAC. 2011;13:496---503.
20.KielinenL,NerbonneM.Furtherinvestigationoftherelationship betweenhearinghandicapandaudiometricmeasuresofhearing impairment.JAcadRehabilAudiol.1990;23:89---94.