REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
Official Publication of the Brazilian Society of Anesthesiologywww.sba.com.br
SCIENTIFIC
ARTICLE
The
influence
of
airway
supporting
maneuvers
on
glottis
view
in
pediatric
fiberoptic
bronchoscopy
Tarik
Umutoglu
a,∗,
Ahmet
Hakan
Gedik
b,
Mefkur
Bakan
a,
Ufuk
Topuz
a,
Hayrettin
Daskaya
a,
Erdogan
Ozturk
a,
Erkan
Cakir
b,
Ziya
Salihoglu
aaDepartmentofAnesthesiologyandReanimation,FacultyofMedicine,BezmialemVakifUniversity,Istanbul,Turkey
bDepartmentofPediatricPulmonaryMedicine,FacultyofMedicine,BezmialemVakifUniversity,Istanbul,Turkey
Received5August2014;accepted17September2014 Availableonline30March2015
KEYWORDS
Fiberoptic bronchoscopy; Pediatrics;
Airwaymaneuvers; Jawtrust;
Glottisview
Abstract
Introduction:Flexiblefiber opticbronchoscopy isavaluableinterventionforevaluationand managementofrespiratorydiseasesinbothinfants,pediatricandadultpatients.Theaimof thisstudyistoinvestigate theinfluenceoftheairwaysupportingmaneuversonglottisview duringpediatricflexiblefiberopticbronchoscopy.
Materialsandmethods: Inthisrandomized,controlled,crossoverstudy;patientsagedbetween 0and 15years whounderwent flexible fiberopticbronchoscopy procedure havingAmerican SocietyofAnesthesiologistsI---IIriskscorewereincluded.Patientshavingriskofdifficult intu-bation,intubatedorpatientswithtracheostomy,andpatientswithreducedneckmobilityor havingcautionsforneckmobilitywereexcludedfromthisstudy.Afterobtainingbestglottic viewattheneutralposition,patientswerepositionedjawtrustwithopenmouth,jawtrust withteethprottution,headtiltchinliftandtripleairwaymaneuversandbestglottisscores wererecorded.
Results:Totalof121pediatricpatients,57girlsand64boys,wereincludedinthisstudy.Both jawtrustwithopenmouthandjawtrustwithteethprottutionmaneuversimprovedtheglottis viewcomparedwithneutralposition(p<0.05),butwedidnotobserveanydifferencebetween jaw trustwith openmouth andjawtrust withteeth prottution maneuvers(p>0.05).Head tilt chinlift and triple airwaymaneuvers improved glottisview when compared withboth jawtrustwithopenmouth andjawtrustwithteethprottutionmaneuversandneutral posi-tion(p<0.05);howeverwefoundnodifferencesbetweenheadtiltchinliftandtripleairway maneuvers(p>0.05).
∗Correspondingauthor.
E-mail:[email protected](T.Umutoglu).
http://dx.doi.org/10.1016/j.bjane.2014.09.016
Conclusion:Allairwaysupportingmaneuvers improvedglottic viewduringpediatric flexible fiberopticbronchoscopy;howeverheadtiltchinliftandtripleairwaymaneuverswerefoundto bethemosteffectivemaneuvers.
©2015SociedadeBrasileiradeAnestesiologia.PublishedbyElsevier EditoraLtda.Allrights reserved.
PALAVRAS-CHAVE
Fibrobroncoscopia; Pediatria;
Manobrasdasvias aéreas;
Elevac¸ãoda mandíbula;
Visibilidadedaglote
Ainfluênciadasmanobrasdesuportedasviasaéreassobreavisibilidadedagloteem fibrobroncoscopiapediátrica
Resumo
Introduc¸ão:A broncofibroscopia flexível (BF) é uma valiosa intervenc¸ão para o manejo e avaliac¸ão de doenc¸as respiratórias em pacientestanto pediátricos quanto adultos. O obje-tivodeste estudofoiinvestigar ainfluênciadasmanobrasde apoiodasviasaéreas sobrea visibilidadedagloteduranteaBFpediátrica.
Materialemétodo:Estudocruzado,randômicoecontrolado,incluindopacientescomidades entre0-15anos,ASAI-II,queforamsubmetidosàBF.Pacientescomriscodeintubac¸ão difí-cil,entubadosoucomtraqueostomiaeaquelescommobilidadereduzidadopescoc¸oouque exigissemcuidadosparaamobilidadedopescoc¸oforamexcluídosdoestudo.Depoisdeobtera melhorvisibilidadedaglotenaposic¸ãoneutra,ospacientesforamposicionadoscomelevac¸ão damandíbulaeaberturadaaberta(EMBA),comelevac¸ãodamandíbulaeprotrusãodosdentes (EMPD),cominclinac¸ãodacabec¸aelevac¸ãodoqueixo(ICEQ)ecomatriplamanobradasvias aéreas(TMVA).Osmelhoresescoresdagloteforamregistrados.
Resultados: Nototal,121pacientespediátricosforamincluídosnoestudo:57pacientesdosexo femininoe64dosexomasculino.AmbosasmanobrasEMBAeEMPDmelhoraramavisibilidade dagloteemcomparac¸ãocomaposic¸ãoneutra(p<0,05),masnãoobservamosdiferenc¸aentre asmanobrasEMBAeEMPD(p>0,05).AsmanobrasICEQeTMVAmelhoraramavisibilidadeda gloteemcomparac¸ãocomasmanobrasEMBAeEMPDeaposic¸ãoneutra(p<0,05);porém,não encontramosdiferenc¸asentreaICEQeaTMVA(p>0,05).
Conclusão:Todasas manobrasde acesso àsvias aéreas melhoraramavisibilidade daglote duranteaBFpediátrica;porém,ainclinac¸ãodacabec¸aeelevac¸ãodoqueixoeatriplamanobra dasviasaéreasforamconsideradasasmanobrasmaiseficazes.
©2015SociedadeBrasileiradeAnestesiologia.PublicadoporElsevierEditoraLtda.Todosos direitosreservados.
Introduction
Flexiblefiberopticbronchoscopy(FOB)isavaluable inter-vention for evaluation and management of respiratory diseases in both infants, pediatric and adult patients. Since its first introduction by Ikeda in 1968, fiber optic bronchoscope in clinical practice; it has been 46 years and there have also been a number of other changes in pediatric pulmonology that have consequences on bron-choscopy practice.1 Most common indications of FOB in
pediatric population arepersistent radiological
abnormal-ities, unexplained respiratory distress, and stridor. Also
direct inspectionin patients with suspected foreignbody
aspirations and broncho-alveolar lavage requirement for
patientshavinglunginfectionaretheotherindications.
Children often require deep sedation or general
anes-thesia during FOB procedure.2 Usually there is a clear
airwaypresentinawakepatientshoweverinanaesthetized
patients,duetochangesinupperairwaystructures;partial
orcompleteobstructionmakesthefiberopticadvancement
difficult. Reduction in muscle tone during deep sedation
or anesthesiahas effects on upper airway structures like
soft palate, tongue base and epiglottismay be relocated
totheposteriorpharyngealwall.Inordertomaintainclear
airwayinanesthetizedpatients,airway-supporting
maneu-versmayberequiredduringfiberopticbronchoscopy.Also
employment of intubating airways like Berman or
Ovass-apian,directlaryngoscopy,lingualtractionandsupraglottic
airwaydevices(LaryngealMaskAirway,I-GelorIntubating
LaryngealMask,etc.)arethealternativewaysofresolving
thisproblem.3,4
The effects of airway supporting maneuvers on glottis
viewduringFOBarenotstudiedandthereisalackof knowl-edgeinpediatricgroupofpatients.Theaimofthisstudyis
todeterminetheeffectsofairwaysupportingmaneuverson
glottisviewduringflexibleFOBinpediatricpatients.
Materials
and
methods
ThestudyprotocolwasapprovedbytheInstitutionalEthical
CommitteeofBezmialemVakifUniversity.Pediatricpatients
Table 1 Anterior laryngopharyngeal (LP) view 4 point Chengetal.5scale.
Grade Description
1 Fullviewofepiglottis,rimaglottidis,corniculate cartilagesandanteriorcommissure.
2 Tipofepiglottisandpartialviewofrimaglottidis andcorniculatecartilagesarevisiblebutanterior commissureofthecordsisnotvisible.
3 Onlytipofepiglottisandcorniculatecartilages arevisiblebutnoneofrimaglottisseen. 4 Onlyfloppyepiglottisseenonposteriorpharynx
butnovisualizationofrimaglottidisand corniculatecartilages.
ofAnesthesiologists(ASA) scoreIor IIscheduled for
flexi-bleFOBbetweenNovember2013andApril2014includedin
thisstudy.Intubatedpatients,patientswithtracheostomy,
patientsrequiringmechanicalventilationsupport,patients
with difficult intubation suspect (Mallampati score 3---4,
micrognathia, craniofacial abnormalities and other
situa-tions related with difficult intubation) and patients with
restrictedneckmobilityorpatientswithcautionsfor neck
mobility were excluded. Patient who had any
contraindi-cations tothe drugs usedin this study wereexcluded. In
accordance withthe Declaration of Helsinki, the purpose
andmethodofthestudyweresufficientlyexplainedtothe
parentsorlegalrepresentativesofeachpatient.Thestudy
wasconductedafterobtaininginformedwrittenconsent.
After usual preoperative fasting interval due to ASA
Guidelines(2hforclearfluids,4hformothermilk,6hfor
diarymilk,formulasandotherfoods).Anintravenous
can-nula inserted at the dorsum of the hand andall patients
premedicated with midazolam 0.03mg/kg and atropine
0.01mg/kg(0.1mgminimum).Topicalanesthesiawith
lido-caine 10% wasapplied tothe nasal mucosaof the nostril
to facilitate FOB for at least 5min before the
interven-tionalprocess.Anesthesiainductionwasmadewithpropofol
1mg/kgandketaminehydrochloride1mg/kgandhypnotic
drugs were utilized to provide deep sedation or general
anesthesia as an adjunct to topical anesthesia for
flexi-blefiberopticbronchoscopy.Patientswerereceivedoxygen
support5L/minwithfacemask afterinitialhypnoticdrug
doseadministration.
Afterinitialadministration,patientswerereceived
con-tinuousketamineandpropofolinfusionswith6---10mg/kg/h
infusionrates.TheRamsaySedationscalewasemployedto
score thesedation level for all patients. The goal wasto
achieveasedationlevelof5or6beforetheprocess.Under
adequatesedationlevelwithsufficientspontaneous
venti-lationwithSpO2>95%FOBprocedurestarted.Patientswere
supine andhead was neutralpositionedduring transnasal
advancement of FOB. Following transnasal advancement
with FOB, anterior and posterior laryngopharyngeal view
evaluated according to 4 and 3 grade scales respectively
adopted from Chenget al.5 study (Tables 1 and 2). After
achievingof the bestview ofanterior or posterior glottis
withneutralposition,additionalairway-supporting
maneu-vers(mentionedbelow)appliedrandomlyandthebestview
Table2 PosteriorLaryngopharyngealview3pointCheng etal.5scale.
Grade Description
1 Corniculatecartilagesandarytenoidslocated upwardfromposteriorpharynxandbothbase cornersofrimaglottidisarenotvisible. 2 Corniculatecartilagesandarytenoidslocated
upwardfromposteriorpharynxandonlyonebase sidecornerofrimaglottidismayvisible.
3 Corniculatecartilageslocatedonposterior pharynxandarytenoidcartilagesarenotvisible.
ofglottiswitheachmaneuversdocumentedwithvideo
cap-tureimages.
The same bronchoscopist whohad more than 10years
ofexperienceinpediatric flexibleFOBperformed all
pro-cedures and an experienced anesthesiologist apart from
anesthesiamanagement whois blindedfrompatient
posi-tioningandairwaysupportingmaneuversdidtheevaluation
of glottis view from video capture images after the FOB
procedures.
Themaneuversare
1. Jawtrustwithteethprotrusionmaneuver(JTTP),
2. Jawtrustwithopenedmouthmaneuver(JTOM),
3. Headtiltchinliftmaneuver(HTCL),
4. Tripleairwaymaneuver(TA).
Aftercapturing imagesof anteriorandposterior
laryn-gopharyngeal view with 4 different airway supporting
maneuvers, the study finalized and FOB procedure was
accomplished.
Statisticalanalysis
Kruskal---Wallistestwasusedtodetectdifferencesingrades
ofLPtissueseenwiththedifferentairwaysupporting
tech-niques.Ap-valuelessthan0.05wasdefinedasstatistically significant.
Results
DemographicdataforallpatientsareshownintheTable3.
Allbronchoscopieswereaccomplishedsuccessfullyvianasal
approach.Ingeneral,whencomparedwithneutralposition
bothfourairwaysupportingmaneuvers(JTTP,JTOM,HTCL,
TA)clinically and statistically(p<0.05) improved anterior andposteriorlaryngopharyngealviewviaflexiblefiberoptic
bronchoscopy. HTCL and TA maneuvers showed the most
improved glottis view, however there were no significant
differencefoundbetweenJTTP---JTOMmaneuvers(p>0.05)
andHTCL---TAmaneuvers.JTTP,JTOM,HTCL,TAmaneuvers
Table3 Patientdemographics.
Age 6.12±4.72
Weight 22.45±16.34
Table4 Statisticalanalysisofglottisviewscoreswithdifferentmaneuversin0---2yearsofagepatients(n=38).
Maneuver Score Neutral JTTP JTOM HTCL TA
Neutral(anterior) 2.79±1.01 1 0.04 0.02 0.00 0.00
JTTP(anterior) 2.32±0.87 0.04 1 NS 0.00 0.00
JTOM(anterior) 2.19±0.87 0.02 NS 1 0.007 0.00
HTCL(anterior) 1.40±0.50 0.00 0.00 0.007 1 NS
TA(anterior) 1.29±0.46 0.00 0.00 0.00 NS 1
Neutral(posterior) 2.29±0.77 1 0.039 0.008 0.00 0.00
JTTP(posterior) 1.95±0.70 0.039 1 NS 0.00 0.00
JTOM(posterior) 1.79±0.62 0.008 NS 1 0.002 0.00
HTCL(posterior) 1.37±0.54 0.00 0.00 0.002 1 NS
TA(posterior) 1.23±0.43 0.00 0.00 0.00 NS 1
Valuesaremean±standarddeviation.
JTTP,jawtrustwithteethprotrusion;JTOM,jawtrustwithopenedmouth;HTCL,headtiltchinlift;TA,tripleairwaymaneuver;NS, notsignificant(p>0.05).
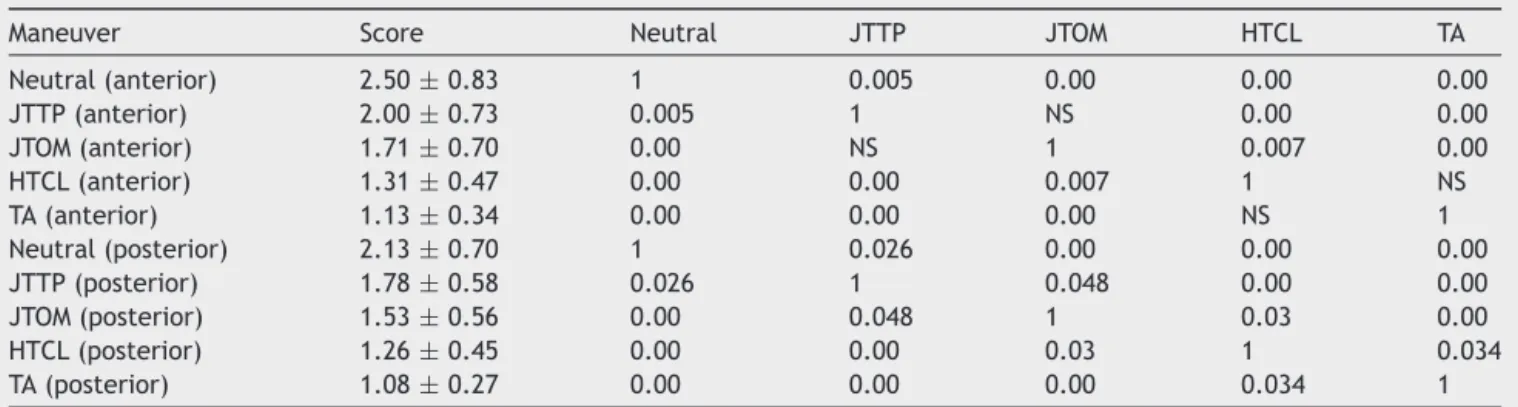
Table5 Statisticalanalysisofglottisviewscoreswithdifferentmaneuversin2---6yearsofagepatients(n=38).
Maneuver Score Neutral JTTP JTOM HTCL TA
Neutral(anterior) 2.50±0.83 1 0.005 0.00 0.00 0.00
JTTP(anterior) 2.00±0.73 0.005 1 NS 0.00 0.00
JTOM(anterior) 1.71±0.70 0.00 NS 1 0.007 0.00
HTCL(anterior) 1.31±0.47 0.00 0.00 0.007 1 NS
TA(anterior) 1.13±0.34 0.00 0.00 0.00 NS 1
Neutral(posterior) 2.13±0.70 1 0.026 0.00 0.00 0.00
JTTP(posterior) 1.78±0.58 0.026 1 0.048 0.00 0.00
JTOM(posterior) 1.53±0.56 0.00 0.048 1 0.03 0.00
HTCL(posterior) 1.26±0.45 0.00 0.00 0.03 1 0.034
TA(posterior) 1.08±0.27 0.00 0.00 0.00 0.034 1
Valuesaremean±standarddeviation.
JTTP,jawtrustwithteethprotrusion;JTOM,jawtrustwithopenedmouth;HTCL,headtiltchinlift;TA,tripleairwaymaneuver;NS, notsignificant(p>0.05).
resultedrespectively moreimprovementinposterior glot-tisview during FOB in 2---6 years of age group (p>0.05). Statistical analysis of the view of anterior and posterior laryngopharyngealtissuesshowedattheTables4---6.
In 0---2 years of age group; at anterior LP view scores
bothfourairwaysupportingmaneuvers(JTTP,JTOM,HTCL,
TA) clinically and statistically (p<0.05) improved
ante-rior and posterior laryngopharyngeal view via flexible
fiberopticbronchoscopywhencomparedwithneutral
posi-tion. Howeverthere were nosignificant differencefound
betweenJTTPandJTOMmaneuvers(p>0.05).HTCLandTA
maneuversshowedstatisticallysignificantdifferencewhen
Table6 Statisticalanalysisofglottisviewscoreswithdifferentmaneuversin6---15yearsofagepatients(n=45).
Maneuver Score Neutral JTTP JTOM HTCL TA
Neutral(anterior) 2.47±0.90 1 0.015 0.009 0.00 0.00
JTTP(anterior) 2.00±0.83 0.015 1 NS 0.00 0.00
JTOM(anterior) 1.93±0.75 0.009 NS 1 0.00 0.00
HTCL(anterior) 1.22±0.42 0.00 0.00 0.00 1 NS
TA(anterior) 1.11±0.31 0.00 0.00 0.00 NS 1
Neutral(posterior) 2.11±0.65 1 0.01 0.001 0.00 0.00
JTTP(posterior) 1.76±0.60 0.01 1 NS 0.00 0.00
JTOM(posterior) 1.62±0.61 0.001 NS 1 0.00 0.00
HTCL(posterior) 1.13±0.34 0.00 0.00 0.00 1 NS
TA(posterior) 1.02±0.15 0.00 0.00 0.00 NS 1
Valuesaremean±standarddeviation.
compared with both JTTP and JTOM (p<0.05) but there werenosignificantdifferencefoundbetweenHTCLandTA maneuvers(p>0.05).
In2---6yearsofagegroup;atanteriorLPscoresshowed similar results like general score. All airway maneuvers clinically and statistically improved at posterior LP view scores. In contrast with general results; JTTP and JTOM, HTCL andTA scoresshowed statisticallysignificant results respectively.
In 6---15 yearsof age group;statistical analysisof both anteriorandposteriorLPviewscoresweresimilarwith gen-eralresultsand0---2yearsofagegroup.
Discussion
Accordingtoour study,comparedtotheneutralposition, allairway-supportingmaneuvers(JTTP,JTOM,HTCLandTA) improved both anteriorand posterior view of glottis dur-ingFOBinallpediatricagegroups.The bestmaneuversto improvebothanteriorandposteriorglottisviewin allage groupsareHTCLandTA.
Flexible FOB via nasal approach under deep sedation or general anesthesia in pediatric group of patients is widely practicedtechnique. Duringdeep sedationor gen-eralanesthesia,loss orreductionof muscletonein upper laryngopharyngealstructuresresultsposteriordisplacement oftongue,softpalateandepiglottisisthemainreasonfor airwayobstructionandlimitedvisibilityduringFOB,asFOB relies onaclear airspacearound bronchoscope’stip.This studywasaimedtodeterminetheeffectsoffourdifferent airwaysupportingmaneuversonglottisviewandtofindthe bestpositionforpatient’sheadandneckforaclearairway duringFOB.
Durgaetal.4showedthatjaw trustcombinedwith
lin-gualtractionresultsaclearairwaypassagefororotracheal
fiberopticintubation.UnfortunatelyDurgaetal.foundthat
jawtrustorlingualtractionfailtoproducefullclearairway
whenusedalone.Liftingtheepiglottisfromposterior
pha-ryngealwallis themajorfactorfor improvingthe viewof
anteriorlaryngopharyngealstructures.Chengetal.5showed
thatJTTP,JTOM,HTCLandTAimprovestheviewofanterior
laryngopharyngealtissuesrespectively.Ourfindingspartially
supportChengetal.study.Wefoundthatbothfour
maneu-versimprovedanteriorviewhoweverwedidn’t found any
differences between JTOM and JTTP and similarly there
were no difference found between HTCL and TA
maneu-versinourstudyexceptforposteriorglottisview2---6years
of age group. In Cheng et al. study as they used muscle
relaxantsandtheirpatientswerenotspontaneously
breath-ing their results were less improved compared with our
results.Differencebetweentheagegroupsintwostudiesis
anotherfactorforcomparison.InacrossoverstudyStacey
etal.3 compareddirectlaryngoscopyandjawtrusttoaid
Fiberopticintubation.Theyfoundthatdirectlaryngoscopy
producedbetterclearairwaypassagewhencomparedwith
jawtrustmaneuver.Unfortunatelytheycomparedonlytwo
methodstoassesstheireffectsonFiberopticview.Itis possi-bletofinddifferentresultsifothermaneuversthatweused
werealsoemployedintheirstudy.Ourstudybasedon
spon-taneous ventilating patients and the depth of anesthesia
mightbeinadequateforlaryngoscopy. Deepsedationwith
propofolandketamineiscommonlyusedinclinicalpractice
fortheproposeofhypnosisandanalgesiaforpediatric
bron-choscopicprocedures.6Ourfindingsshowedthatthemajor
factors,thathasinfluenceontheanteriordisplacementof
theepiglottisfrom posterior pharyngeal wallare anterior
movementofmandibulaandheadtiltpositioning.
Recent studyby Abramsonetal.7 assessed agerelated
changes of the upper airway by 3-dimentional computed
tomography.Theyfoundthatupperairwayparameterssuch
asvolume,surfacearea,length,meancross-sectionalarea
were increased in concordance with the increase in age.
Howevertheywerefoundnodifferenceregardingtosexin
airwayparameters.Kimetal.8foundthattherewere
pro-portionaldifferencebetweenchildrenolderthan12months
ofageandchildrenyoungerthan12monthsofageregarding
ultrasoundmeasurementsofsubglotticdiameterand
empir-icalformulaforendotrachealtubefitting.
Vialetetal.9foundthatslightheadextensionnarrowsthe
angledeltaandimprovesalignmentofthelineofvisionof
theglottisandlaryngealaxis.Thisdatasupportourfindings
that positions including head extension like HTCL and TA
arelikelytoimproveglottisviewweatherinbronchoscopy
orotherimagingmodalities.
Meieretal.10showedthatchinliftandjawtrust
maneu-vers combined with continuous positive airway pressure
(CPAP)improvetheglotticopeningviaflexiblenasal
laryn-goscopy and decrease stridor in spontaneously breathing,
anesthetizedchildren.HoweverBruppacheretal.11showed
that jaw trust has a superior effect to improve airway
patencyandventilationin childrenundergoing
adenoidec-tomywhencomparedwithchinliftandCPAP.
Reberetal.12investigatedJawtrust,Chinliftand
com-binationofthismaneuverswithCPAPin24childrenhaving
adenotonsillar hypertrophy. Similarly with our study chin
liftcombinedwithCPAPshowedthemostefficient
combi-nationtoreduce thestridorandimprovetheglottisscore
whencomparedwithjawtrust aloneor combination with
CPAP.
In conclusion, airway-supporting maneuvers improves
glottisviewduringFOB.HeadtiltchinliftandTripleairway
maneuverswerefound tobethemost efficientmaneuver
forbothanteriorandposteriorglottisviewduringpediatric
Fiberopticbronchoscopy.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.GodfreyS,AvitalA,MaayanC,etal.Yieldfromflexible bron-choscopyinchildren.PediatrPulmonol.1997;23:261---9.
2.Berkenbosch JW, Graff GR, Stark JM, et al. Use of a remifentanil---propofolmixtureforpediatricflexiblefiberoptic bronchoscopysedation.PaediatrAnaesth.2004;14:941---6.
3.StaceyMR,RassamS,SivasankarR,etal.Acomparisonofdirect laryngoscopyandjawthrusttoaidfibreopticintubation. Anaes-thesia.2005;60:445---8.
5.ChengKI,YunMK,ChangMC,etal.Fiberopticbronchoscopic viewchangeoflaryngopharyngealtissuesbydifferentairway supportingtechniques:comparisonofpatientswithandwithout openmouthlimitation.JClinAnesth.2008;20:573---9.
6.Bakan M, Topuz U, Umuto˘glu T, et al. Remifentanyl-based totalintravenousanesthesiaforpediatricrigidbronchoscopy: comparison of adjuvant propofol and ketamine. Clinics. 2014;69:373---7.
7.AbramsonZ,SusarlaS,TroulisM,etal.Age-Relatedchangesof theupperairwayassessed by3-dimensionalcomputed tomo-graphy.JCraniofacSurg.2009;20Suppl.1:657---63.
8.Kim EJ, KimSY, KimWO, etal. Ultrasound measurementof subglotticdiameterandanempiricalformulaforproper endo-tracheal tube fitting in children. Acta Anaesthesiol Scand. 2013;57:1124---30.
9.VialetR,NauA,ChaumoitreK,etal.Effectsofheadposture ontheoral,pharyngealandlaryngealaxisalignmentininfants andyoung childrenbymagnetic resonanceimaging.Paediatr Anaesth.2008;18:525---31.
10.MeierS,GeiduschekJ,PaganoniR,etal.Theeffectofchinlift, jawthrust,andcontinuouspositiveairwaypressureonthesize oftheglotticopeningandonstridorscoreinanesthetized, spon-taneouslybreathingchildren.AnesthAnalg.2002;94:494---9.
11.BruppacherH,ReberA,Keller JP,et al.Theeffectsof com-monairwaymaneuversonairwaypressureandflowinchildren undergoingadenoidectomies.AnesthAnalg.2003;97:29---34.