SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Original
Article
Can
ethanol
be
used
as
an
adjuvant
to
extended
curettage
in
order
to
reduce
the
recurrence
rate
of
aneurysmal
bone
cyst?
夽
Saeed
Solooki,
Yaghoob
Keikha,
Amir
Reza
Vosoughi
∗ShirazUniversityofMedicalSciences,BoneandJointDiseasesResearchCenter,Shiraz,Iran
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received20December2015 Accepted28April2016 Availableonline20July2016
Keywords:
Aneurysmalbonecyst Ethanol
Alcohol Neoplasms
a
b
s
t
r
a
c
t
Objective:Thebesttreatmentofaneurysmalbonecyst(ABC)isstillunclear.Thisstudyaimed toevaluatetheusefulnessofextendedcurettageandethanolasanadjuvanttoreducelocal recurrenceofABCs.
Methods:Retrospectively,68casestreatedforprimaryandsecondaryABCscausedbybenign tumorsfrom2003to2013wereenrolledtoafollow-upvisitbetweenonetotenyearsafter thesurgery.Thetreatmentprotocolwasen-blocresection,biopsyandcurettage,extended curettageconsistedofcurettage,high-speedburring,ethanol96%,andelectrocauterization (combinedfour-stepalcohol-usingapproach)followedbydefectfilling,consecutively.
Results:Among 36 patients with primary ABCs (16 male, 20 female, mean age of 16 years,range3–46years),29casesweretreatedwiththecombinedfour-stepalcohol-using approach, fourpatientswithresection,andthreewithbiopsyandcurettage.Thirty-two caseshadsecondary ABCsonbenignlesions(17male, 15female). Therecurrencerate was5.88inallprimaryandsecondaryABCcases;tworecurrencesamong29patientswith primaryABCs(6.9%)andonerecurrenceamongthe22caseswithsecondaryABCs(4.5%).
Conclusions: Itcouldbesuggestedthatthecombinedfour-stepalcohol-usingapproachmay resultinaverylowrecurrencerateofprimaryandsecondaryABClesions.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
O
etanol
pode
ser
usado
como
adjuvante
na
curetagem
ampla
a
fim
de
reduzir
a
taxa
de
reincidência
de
cisto
ósseo
aneurismático?
Palavras-chave:
Cistoósseoaneurismático Etanol
r
e
s
u
m
o
Objetivo:Aindanãosesabequalomelhortratamentoparacistosósseosaneurismáticos (COA).Esteestudotevecomoobjetivoavaliarautilidadedacuretagemestendidaedoetanol comoadjuvanteparareduzirareincidêncialocaldeCOAs.
夽
StudywascarriedoutinBoneandJointDiseasesResearchCenter,ShirazUniversityofMedicalSciences,Shiraz,Iran.
∗ Correspondingauthor.
E-mail:[email protected](A.R.Vosoughi).
http://dx.doi.org/10.1016/j.rboe.2016.04.007
Álcool Neoplasmas
Métodos: Retrospectivamente,68casosquereceberamtratamentoparaCOAsprimáriose secundárioscausadosportumoresbenignosentre2003e2013foramchamadosparauma consultadeseguimento,emumintervaloentreumedezanosapósacirurgia.Oprotocolode tratamentofoiressecc¸ãoembloco,biópsiaecuretagem;acuretagemestendidaconsistiuem curetagem,broqueamentoemaltavelocidade,etanol96%eeletrocauterizac¸ão(abordagem combinadaemquatroetapasusandoálcool),seguidadopreenchimentododefeito,deforma consecutiva.
Resultados: Entreos36pacientescomCOAsprimárias(16dosexomasculino,20dosexo feminino,idademédia de16anos,intervalo3-46anos),29casosforamtratadoscoma abordagemcombinadaemquatroetapasusandoálcool,quatropacientescomressecc¸ãoe trêscombiópsiaecuretagem.TrintaedoiscasosapresentavamCOAssecundáriasemlesões benignas(17dosexomasculino,15dosexofeminino).Ataxadereincidênciafoide5,88em todososcasosdeCOAsprimáriasesecundárias;duasreincidênciasforamobservadasentre 29pacientescomCOAsprimária(6,9%)eumareincidênciaentreos22casos(4,5%)deCOAs secundária.
Conclusão: Sugere-sequeaabordagemcombinadaemquatroetapasusandoálcoolpode resultaremumataxadereincidênciamuitobaixaemlesõesCOAsprimáriasesecundárias. ©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Aneurysmalbonecyst(ABC),ararebenignandlocally aggres-sivebonelesion,isablood-filledcavitywithinanexpanded regionofthebonewiththinningofthesurroundingcortex.1
ItwasfirstdescribedbyJaffeandLichtenstein2in1942.Itmay
presentasaprimarybonecystorasecondarylesionarising from other osseousconditions like giant cell tumor, chon-droblastoma,fibrousdysplasia,osteoblastoma,non-ossifying fibroma, telangiectatic osteosarcoma.3,4 Although precise
pathogenesisofABCremainsunclear,multipletheorieshave beenproposed.Theyhavebeendescribedthatspecific translo-cationaleventsonchromosome16and17asthemainetiology ofprimaryABCs,5,6andintraosseousorsubperiosteal
hemor-rhagebecauseofabnormalvenouscirculationasacauseof secondaryABCs.7ABCtumorsarefrequentlyseeninthefirst
twodecadesoflifewithslightfemalepredominance.Itmay occurinallbones,butmetaphysisofthelongbonesanddorsal elementsofthevertebraearethemostcommonsites.8,9
Treatment of ABClesions in the long bones commonly is extended curettage with bone grafting or wide en-bloc resectionoftumor.3,8,10 Someauthorshaveusedadjuvants
inducinghydrogenperoxide,8phenol,11
polymethylmethacry-late bone cement,12 liquid nitrogen,13 argon beam,14 and
high-speedburring15inordertodecreasetherecurrencerate
ofABClesions.1Themainpurposeofthisstudyisto
evalu-atetheusefulnessofethanolasanadjuvantinacombined four-stepprocedureincludingcurettage,high-speedburring, ethanol96%andelectrocauterizationfollowedbygraftingto reducelocalrecurrenceofprimaryandsecondaryABCs devel-opedonbenigntumors.
Methods
and
materials
Afterapproval ofthe study bythe ethic committeeof our university,aretrospectivereviewofmedicalclinicalrecords
wasperformed oncasestreatedforABCfrom2003to2013 bytheseniorauthoratthemainorthopediccenterofsouth ofIran.AfterexclusionofcaseswithsecondaryABCsarising frommalignanttumors,68patients,withrangeoffollow-up visit of1to 10 years,signedthe preparedwrittenconsent form. They consisted of 36 cases with primary ABCs and 32 patientswithsecondaryABCsonbenigntumors. Demo-graphicdata(ageatthetimeofthesurgery,gender),primary symptomofthepatient,exactlocationofABClesion, patho-logicreports,andfurthersurgerieswerereviewedaccording tothemedicalrecordsandavailableimages.Themostrecent takenX-rayradiographswereconsideredtoevaluatecuringor recurrence.
Table1–DistributionofABClesionsbyanatomicsite.
Femur Tibia Humerus Radius Foot Fibula Hand Ulna Clavicle Pelvis Patella
PrimaryABC 11 6 5 3 3 2 2 1 1 1 1
SecondlyABC 13 9 5 – 1 1 1 1 1 1 –
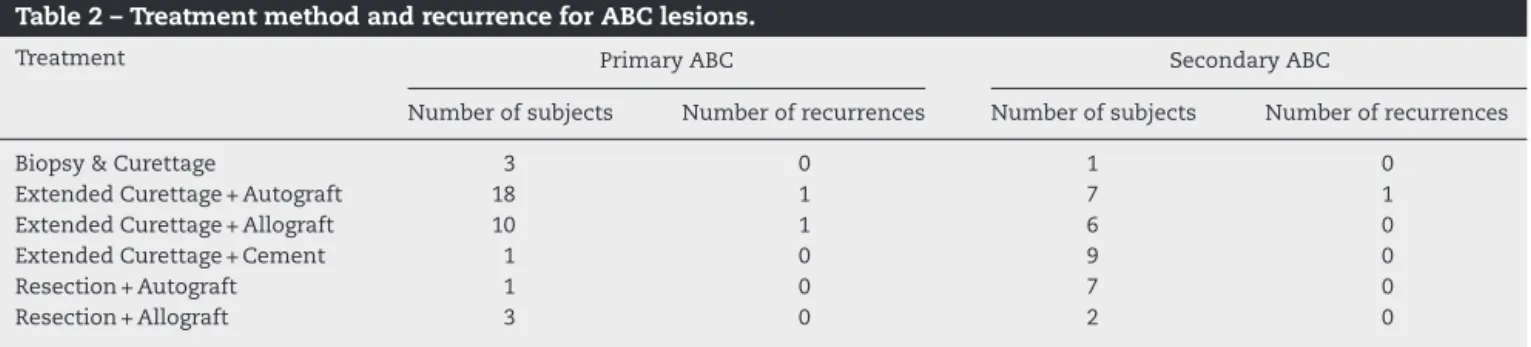
Table2–TreatmentmethodandrecurrenceforABClesions.
Treatment PrimaryABC SecondaryABC
Numberofsubjects Numberofrecurrences Numberofsubjects Numberofrecurrences
Biopsy&Curettage 3 0 1 0
ExtendedCurettage+Autograft 18 1 7 1
ExtendedCurettage+Allograft 10 1 6 0
ExtendedCurettage+Cement 1 0 9 0
Resection+Autograft 1 0 7 0
Resection+Allograft 3 0 2 0
voidofperiarticularlesionsandsecondaryABCsongiantcell tumors.Treatingofpathologicalfractureswasalittledifferent; afterextendedcurettage,thefracturewasreducedandfixed. Aftercoveringtheperipheryofthefracturebymultiplegauzes andusingsuctiontubetoreducetheriskofethanolleakage, ethanolwasspilledinthelesion.Afterelectrocauterization, bonegraftwasimpactedinthedefect.
AfteranyrecurrencefoundonX-ray,othermodalitiessuch
asCT scanor magneticresonance imagingwas requested,
basedonthecharacteristicsofthelesion.Ifitwasbigwith pos-sibilityoffractureinthefuture,surgerywasdoneaccording tothecombinedfour-stepalcohol-usingapproach.
Results
PrimaryABC
ThirtysixpatientswithhistologicallyconfirmedprimaryABC weretreated.Therewere16male(44%)and20female(56%) withamean ageof16 years(range3–46years)atthetime ofsurgery.Halfofthesubjectswerebetween10and20years ofage(19%ofcases<10yearsofage,31%ofcases>20years
of age). Twenty one cases (58%) had lesion on the
right-sidedlimbsofthebodyand15hadABCsofleftlimbs(42%).
Table1showsdistributionofABClesionsbytheanatomicsite. Onpresentation, 12 subjects referredwith pathologic frac-ture,10casescamewithmassand11hadpain.ABClesions werefoundinthreecasesincidentally.Treatmentmethodand recurrenceratearedescribedinTable2.
Totally,wehad tworecurrentABCsintheseriestreated withcombinedfour-stepalcohol-usingapproach(6.9%).The firstcasewasasix-year-oldboywithABCofdistalofright radiustreatedwith extendedcurettageand allograft inser-tion.Hedevelopedlocalrecurrenceoflesiononeyearafter surgery.Thesecondsubjectwasathree-year-oldgirl under-wentextendedcurettageandautograftforABCofdistalradius ofleftupperlimb.
SecondaryABC
ThirtytwocaseshadsecondaryABCsonbenignlesions(male: 17,female:15). Themeanageofthepatientswas29years,
witharangeof7–51years.Twosubjects(6%)hadageofless than10years,12patients(38%)werebetween10and20years ofage,and 18cases(56%)were olderthan 20yearsofage. TheanatomicallocationsforthesecondaryABClesionsare listedinTable1.Thecomplaintsofthepatientsatthetimeof initialvisitwerepainin23cases,massin6subjects, patho-logic fracture in2 patients, and incidental finding in one. Primarylesionsweregiantcelltumorin13cases(40%),fibrous dysplasiain7subjects(22%),chondroblastomain6(19%), non-ossifyingfibromain5(16%)andhistiocytomainonepatient (3%).Nineoutof13caseswithgiantcelltumorwerecured withextendedcurettageandcementwithoutrecurrence,as showninTable2.Onlyonecaseamong13treatedwith com-binedfour-stepalcohol-usingapproachhadrecurrenceofthe lesion. Thispatient was acase ofsecondary ABCon non-ossifying fibroma. Frozen-sectionbiopsy duringthesecond surgeryapprovedrecurrenceofABConhealednon-ossifying fibroma;socombinedfour-stepalcohol-usingapproachwas carriedout.
Discussion
The optimal methodof treatment for ABCis still unclear. Althoughdifferentmaterialinjectionsandpercutaneous scle-rotherapyhavebeenintroducedasanefficienttreatment,16–18
extendedcurettagewithorwithoutbonegraftingisthemost classically accepted mode oftreatment in the long bones. Wideen-blocresectionisanexcellentoptiontopreventany recurrencebutcomplexresectionoftumormustbelimited toexpandableboneslikedistalulnaorproximalfibula.Our resultsshowed100%localcontrolofABClesionsafter com-pleteresectionoftumorsfollowedbygrafting.Usingextensive surgery ofen-bloc resection associatedwith neurovascular damage,considerablemorbidity,andcompletereconstructive surgeriesarenotpracticalformanylocationsintheskeletal systemofhumanbeing.
Other than wide resection, curettage and bone graft showedfailureratesoflessthan30%.1,3,8,10,19,20Using
differ-entadjuvantsinordertoreducetherecurrenceratehavebeen associatedwithcontroversialresults.Kec¸ecietal.21 didnot
withoutadjuvants and patientstreated withcurettageand bonegraftingbesideburringor phenolusage.Ontheother hand,usingcurettage,burring,andbonegraftingresultedin lower recurrence rates.15,22 Alsoadding electrocautery and
phenol in addition toburring have been suggested bythe others.23Shiftingfromphenoltoethanolappearsrationaldue
toitscorrosiveeffects,chemicalburns,neurovascular dam-ages,mucosaldamagesoftherespiratorysystem,paralysisof peripheralnerveendings,andevensystemicpoisoning.24
Nowadays intracystic injection of alcohol (polidocanol) showedgoodresultswithalowrateofcomplications.22Evenit
isatechniqueofchoiceinsomecenters.1Ethanolisa
harm-lessand easily-availablematerialinmostoperationrooms. Theefficaciesofethanoltotreatgiantcelltumor,25 osteoid
osteoma,26 skeletal metastasis,27 and other bone lesions28
havebeendescribedintheliterature.Theefficacyofethanol hasnotbeendescribedyettoreducerecurrencerateofABC lesions.Wecouldsuggestusingalcoholasanadjuvanttotreat primaryandsecondaryABClesionswithrecurrencerateof about6%.Wehadjustonerecurrenceamong22cases(4.5%) withsecondaryABClesionsandtwoamong29patientswith primaryABC(6.9%).
Weacknowledgethelimitednumberofourpatientsand minimumfollow-upduration.But itisobvious thata min-imum oftwo years follow-upis requiredtodiagnose most ofrecurrencesofABClesions,becausemostofthemoccur within12–18months.29 Inthepresentedstudy,allpatients
treatedwithfour-stepalcohol-usingapproachwereevaluated 2yearspost-operatively.So,ourresultscouldbereliable.Just twopatientswithen-blocresectionwere assessedoneyear aftersurgery.
Conclusion
Itcouldbesuggestedthatfour-stepalcohol-usingapproach canreducerecurrencerateinpatientswithprimaryand sec-ondaryABClesions.Moreover,the recurrencerate islower thanothers reportedafterusingother adjuvantsinthe lit-erature.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. MascardE,Gomez-BrouchetA,LambotK.Bonecysts: unicameralandaneurysmalbonecyst.OrthopTraumatol SurgRes.2015;1011Suppl.:S119–27.
2. JaffeHL,LichtensteinL.Solitaryunicameralbonecystwith emphasisontheroentgenpicture:thepathological appearanceandpathogenesis.ArchSurg.1942;44:1004–25.
3. MankinHJ,HornicekFJ,Ortiz-CruzE,VillafuerteJ,Gebhardt MC.Aneurysmalbonecyst:areviewof150patients.JClin Oncol.2005;23(27):6756–62.
4. BorianiS,DeIureF,CampanacciL,GasbarriniA,BandieraS, BiaginiR,etal.Aneurysmalbonecystofthemobilespine: reporton41cases.Spine(PhilaPa1976).2001;26(1):27–35.
5.OliveiraAM,Perez-AtaydeAR,InwardsCY,MedeirosF,DerrV, HsiBL,etal.USP6andCDH11oncogenesidentifythe neoplasticcellinprimaryaneurysmalbonecystsandare absentinso-calledsecondaryaneurysmalbonecysts.AmJ Pathol.2004;165(5):1773–80.
6.LeithnerA,MachacekF,HaasOA,LangS,RitschlP,RadlR, etal.Aneurysmalbonecyst:ahereditarydisease?JPediatr OrthopB.2004;13(3):214–7.
7.KransdorfMJ,SweetDE.Aneurysmalbonecyst:concept, controversy,clinicalpresentation,andimaging.AJRAmJ Roentgenol.1995;164(3):573–80.
8.DormansJP,HannaBG,JohnstonDR,KhuranaJS.Surgical treatmentandrecurrencerateofaneurysmalbonecystsin children.ClinOrthopRelatRes.2004;(421):205–11.
9.MendenhallWM,ZloteckiRA,GibbsCP,ReithJD,Scarborough MT,MendenhallNP.Aneurysmalbonecyst.AmJClinOncol. 2006;29(3):311–5.
10.LinPP,BrownC,RaymondAK,DeaversMT,YaskoAW. Aneurysmalbonecystsrecuratjuxtaphyseallocationsin skeletallyimmaturepatients.ClinOrthopRelatRes. 2008;466(3):722–8.
11.CapannaR,SudaneseA,BaldiniN,CampanacciM.Phenolas anadjuvantinthecontroloflocalrecurrenceofbenign neoplasmsofbonetreatedbycurettage.ItalJOrthop Traumatol.1985;11(3):381–8.
12.OzakiT,HillmannA,LindnerN,WinkelmannW.Cementation ofprimaryaneurysmalbonecysts.ClinOrthopRelatRes. 1997;(337):240–8.
13.MarcoveRC,ShethDS,TakemotoS,HealeyJH.Thetreatment ofaneurysmalbonecyst.ClinOrthopRelatRes.
1995;(311):157–63.
14.CummingsJE,SmithRA,HeckRKJr.Argonbeamcoagulation asadjuvanttreatmentaftercurettageofaneurysmalbone cysts:apreliminarystudy.ClinOrthopRelatRes.
2010;468(1):231–7.
15.WangEH,MarforiML,SerranoMV,RubioDA.Iscurettageand high-speedburringsufficienttreatmentforaneurysmalbone cysts?ClinOrthopRelatRes.2014;472(11):3483–8.
16.ShielsWE2nd,MayersonJL.Percutaneousdoxycycline treatmentofaneurysmalbonecystswithlowrecurrencerate: apreliminaryreport.ClinOrthopRelatRes.
2013;471(8):2675–83.
17.Lambot-JuhanK,PannierS,GréventD,PéjinZ,BretonS, BertelootL,etal.Primaryaneurysmalbonecystsinchildren: percutaneoussclerotherapywithabsolutealcoholand proposalofavascularclassification.PediatrRadiol. 2012;42(5):599–605.
18.BrosjöO,PechonP,HeslaA,TsagozisP,BauerH.
Sclerotherapywithpolidocanolfortreatmentofaneurysmal bonecysts.ActaOrthop.2013;84(5):502–5.
19.ReddyKI,SinnaeveF,GastonCL,GrimerRJ,CarterSR. Aneurysmalbonecysts:dosimpletreatmentswork?Clin OrthopRelatRes.2014;472(6):1901–10.
20.GibbsCPJr,HefeleMC,PeabodyTD,MontagAG,AithalV, SimonMA.Aneurysmalbonecystoftheextremities.Factors relatedtolocalrecurrenceaftercurettagewithahigh-speed burr.JBoneJtSurgAm.1999;81(12):1671–8.
21.Kec¸eciB,Küc¸ükL,IsayevA,SabahD.Effectofadjuvant therapiesonrecurrenceinaneurysmalbonecysts.Acta OrthopTraumatolTurc.2014;48(5):500–6.
22.VarshneyMK,RastogiS,KhanSA,TrikhaV.Issclerotherapy betterthanintralesionalexcisionfortreatinganeurysmal bonecysts?ClinOrthopRelatRes.2010;468(6):1649–59.
24.PiotrowskiJK.Evaluationofexposuretophenol:absorptionof phenolvapourinthelungsandthroughtheskinand excretionofphenolinurine.BrJIndMed.1971;28(2):172–8.
25.LinWH,LanTY,ChenCY,WuK,YangRS.Similarlocalcontrol betweenphenol-andethanol-treatedgiantcelltumorsof bone.ClinOrthopRelatRes.2011;469(11):3200–8.
26.el-MowafiH,RefaatH,KotbS.Percutaneousdestructionand alcoholisationforthemanagementofosteoidosteoma.Acta OrthopBelg.2003;69(5):447–51.
27.GangiA,KastlerB,KlinkertA,DietemannJL.Injectionof alcoholintobonemetastasesunderCTguidance.JComput AssistTomogr.1994;18(6):932–5.
28.FilippiadisDK,TuttonS,KelekisA.Percutaneousbonelesion ablation.RadiolMed.2014;119(7):462–9.