www.rpped.com.br
REVISTA
PAULISTA
DE
PEDIATRIA
ORIGINAL
ARTICLE
Profile
of
patients
with
genitourinary
anomalies
treated
in
a
clinical
genetics
service
in
the
Brazilian
unified
health
system
Ilanna
Fragoso
Peixoto
Gazzaneo
a,
Camila
Maia
Costa
de
Queiroz
a,
Larissa
Clara
Vieira
Goes
a,
Victor
José
Correia
Lessa
a,
Reinaldo
Luna
de
Omena
Filho
b,
Diogo
Lucas
Lima
do
Nascimento
b,
Reginaldo
José
Petroli
a,
Susane
Vasconcelos
Zanotti
a,
Isabella
Lopes
Monlleó
a,∗aUniversidadeFederaldeAlagoas(Ufal),Maceió,AL,Brazil
bUniversidadeEstadualdeCiênciasdaSaúdedeAlagoas(Uncisal),Maceió,AL,Brazil
Received27February2015;accepted11June2015 Availableonline25December2015
KEYWORDS Genitalia; Sexual
differentiation/ genetics; Etiology
Abstract
Objective: Todescribethe profileofpatientswith genitourinaryabnormalitiestreatedata tertiaryhospitalgeneticsservice.
Methods: Cross-sectionalstudyof1068medicalrecordsofpatientstreatedbetweenApril/2008 andAugust/2014.A totalof115casessuggestiveofgenitourinaryanomalieswere selected, regardlessofage.A standardizedclinicalprotocolwasused,aswellaskaryotype,hormone levels and genitourinary ultrasound for basic evaluation. Laparoscopy, gonadal biopsy and molecularstudieswereperformedinspecificcases.Patientswithgenitourinarymalformations wereclassifiedasgenitourinaryanomalies(GUA),whereastheothers,asDisordersofSex Dif-ferentiation(DSD).Chi-square,FisherandKruskal---Wallistestswereusedforstatisticalanalysis andcomparisonbetweengroups.
Results: 80subjectsmettheinclusioncriteria,91%withDSDand9%withisolated/syndromic GUA.TheagewasyoungerintheGUAgroup(p<0.02),butthesegroupsdidnotdifferregarding externalandinternalgenitalia,aswellaskaryotype.Karyotype46,XYwasverifiedin55%and chromosomalaberrationsin17.5%ofcases.Ambiguousgenitaliaoccurredin45%,predominantly in46,XXpatients(p<0.006).DisordersofGonadalDifferentiationaccountedfor25%and con-genitaladrenalhyperplasia,for17.5%ofthesample.Consanguinityoccurredin16%,recurrence in12%,lackofbirthcertificatein20%andinterruptedfollow-upin31%ofcases.
∗Correspondingauthor.
E-mail:[email protected](I.L.Monlleó).
http://dx.doi.org/10.1016/j.rppede.2015.06.024
Conclusions: PatientswithDSDpredominated.Ambiguousgenitaliaandabnormalsexual differ-entiationweremorefrequentamonginfantsandprepubertalindividuals.Congenitaladrenal hyperplasia was the most prevalent nosology. Youngerpatients were more common in the GUAgroup.Abandonmentandlowerfrequencyofbirthcertificateoccurredinpatientswith ambiguousormalformedgenitalia.Thesecharacteristicscorroboratetheliteratureandshow thebiopsychosocialimpactofgenitourinaryanomalies.
©2015SociedadedePediatriadeSãoPaulo.PublishedbyElsevierEditoraLtda.Thisisanopen accessarticleundertheCCBYlicense(https://creativecommons.org/licenses/by/4.0/).
PALAVRAS-CHAVE Genitália;
Diferenciac¸ão sexual/genética; Etiologia
Perfildepacientescomanormalidadesgeniturináriasatendidosemservic¸o degenéticaclínicanosistemaúnicodesaúde
Resumo
Objetivo: Descrever o perfil de pacientes com anormalidades geniturinárias atendidos em servic¸odegenéticadehospitalterciário.
Métodos: Estudo transversal de 1.068 prontuários de pacientesatendidos entre abril/2008 e agosto/2014.Foram selecionados 115casos sugestivos deanomalias geniturinárias, inde-pendentemente daidade. Usaram-se protocolo clínico padronizado, cariótipo, hormôniose ultrassonografiageniturináriaparaavaliac¸ãobásica.Laparoscopia,biopsiagonadaleestudos moleculares foramfeitos em casos específicos. Pacientes com malformac¸ões geniturinárias foram classificados como defeitos geniturinários (DGU), os demais, como distúrbios da diferenciac¸ão do sexo (DDS). Usaram-se qui-quadrado, Fisher e Kruskal-Wallis para análise estatísticaecomparac¸ãoentreosgrupos.
Resultados: Preencheramos critérios de inclusão 80 sujeitos,91% comDDSe 9% comDGU isolados/sindrômicos.AidadefoimenornogrupoDGU(p<0,02),masessesgruposnão diferi-ram quanto agenitáliaexterna, internae cariótipo.Verificou-se cariótipo46,XY em 55% e aberrac¸õescromossômicasem17,5%doscasos.Ambiguidadegenitalocorreuem45%, predomi-nouempacientes46,XX(p<0,006).Distúrbiosdadiferenciac¸ãogonadalrepresentaram25%e hiperplasiaadrenalcongênita;17,5%daamostra.Consanguinidadeocorreuem16%,recorrência em12%,ausênciaderegistrocivilem20%einterrupc¸ãodoseguimentoem31%doscasos.
Conclusões: Predominaram pacientescomDDS. Ambiguidade genital e diferenciac¸ãosexual anômalaforammaisfrequentesentrerecém-nascidosepré-púberes.Hiperplasiaadrenal con-gênitafoianosologiamaisprevalente.PacientesmaisjovenspertenciamaogrupoDGU.Menor frequênciaderegistrocivileabandonoocorreramempacientescomgenitáliaambíguaou mal-formada.Essascaracterísticascorroboramaliteraturaeevidenciamoimpactobiopsicossocial dasanormalidadesgeniturinárias.
©2015SociedadedePediatriadeSãoPaulo.PublicadoporElsevierEditoraLtda.Esteéumartigo OpenAccesssobalicençaCCBY(https://creativecommons.org/licenses/by/4.0/deed.pt).
Introduction
Genitourinary abnormalities (GUA) represent 35---45% of birthdefectsandincludeawiderangeofstructural abnor-malities of the urinary and reproductive tracts, whose collectiveoccurrencereflectstheirembryologicaloriginand commongeneticcontrol.1---3 The clinicalspectrumextends
from minor anomalies such as glandular hypospadias to severe conditions such as bladder exstrophy. The clini-calpresentationmay beisolatedor associatedwithother anatomicaldefectsandpresentsyndromicconditions.The etiology comprises genetic causes resulting from chro-mosomal, monogenic or multifactorial abnormalities, not genetic,associatedwithexposuretoteratogens,andthere alsotheunknowncauses.1,4
DisordersofSexDifferentiation(DSD)areaspecialgroup of GUA in which the development of genetic, gonadal or
anatomicalsexisatypicalorincongruous.Clinical manifes-tationsrangefrom classicalgenitalambiguity, manifested atbirth,toinfertilityinadults.4,6---11 Clinicalheterogeneity
andtheuseofdifferentinclusioncriteria,collecting meth-ods,codingandrecordingofGUAaccountforwidevariations inprevalence. Withtheexception ofminorabnormalities, suchasisolatedhypospadiaswithaprevalenceof1:250live births,some disordersmay beasrare as1:100,000, asin cloacalexstrophy.12,13IntheSDDgroup,aglobalprevalence
of1---2:10,000birthsisassumed,2,4,9,11whichputthese
con-ditionsinthegroupofso-calledrarediseases,recentfocus of health care policies in genetics in the National Health System(SistemaÚnicodeSaúde---SUS).14
epidemiologicalandclinicalchallenge.So,withtheprospect of subsidizing health care improvement proposals in this area,theobjectiveofthisstudywastodescribethe clin-icalprofileofpatientswithGUAtreatedinclinicalgenetics serviceatatertiaryhospitalintheSUS.
Method
Descriptive and cross-sectional study based on analysis of 1068 digital medical records of patients seen in the Servic¸o de Genética Clínica of the Hospital Universitário Professor AlbertoAntunes of the UniversidadeFederal de Alagoas(SGC/HUPAA/UFAL)betweenApril2008andAugust 2014. This service, unique in the state, serves the entire SUS demand. The cases are referred via Coordenac¸ão de Regulac¸ãodaAssistência,withan averagevolumeofeight newcasesperweek.Patientsundertheageof18whohave morphogenesisdefectswithorwithoutassociationwith psy-chomotorretardation/intellectualdisabilitiescomprisethe predominantgroup.
Atotalof115eligiblecasesweremappedfromthesearch ofthefollowingdescriptors,regardlessofageatfirst medi-calconsultation:genitalambiguity;micropenis;hypospadias (any grade); posterior labial fusion; gynecomastia; crypt-orchidism; clitoromegaly; primary amenorrhea; secondary sexualunderdevelopment; gonadal dysgenesis.Cases with incompletedescriptionoftheexternalgenitalmorphology, karyotypeabsence,and conclusivediagnosis of conditions outsidetheGUAspectrum,suchasinguinalherniasand Noo-nansyndrome,wereexcluded.Thefinalsampleconsistedof 80subjects.
Datawereobtainedusingtheownprotocolof theGUA clinicconsistingofhistoryofpresentcomplaintand gesta-tionalhistory,geneticandenvironmentalrisk factors,and generalphysicalexaminationwithemphasisongenital mani-festations.Thisprotocolwasestablishedin2009andapplied prospectivelyto70(87%)cases.Datafromtheremaining10 (13%)patientstreatedin2008wereobtainedfromthedigital medicalrecordoftheservice.
Micropenis was defined as penile length less than 2.5 standarddeviationsforage;cryptorchidism,asextra-scrotal positionofthetestis;andgenitalambiguitywereclassified accordingtoPrader’scriteria5:P1---Genitalia
indistinguish-ablefromfemale,exceptforenlargedphallus;P2---Phallus furtherenlarged, labioscrotal fusion and without urogeni-tal sinus; P3---Phallus of penileappearance, almost total labioscrotal fusion andperineal opening of theurogenital sinus; P4---Enlarged phallus,complete labioscrotal fusion and penoscrotal urogenital sinus opening; P5 --- Phallusof penileappearance,completelabioscrotalfusion,urogenital sinusopeninginthebodyofthephallusorbalanicarea.15
Thebasiccomplementaryevaluationincludedperipheral bloodkaryotypewithGTGbandingandbandresolutionsof 400---450.Atleast40metaphasesperpatientwereanalyzed intheHumanCytogeneticsLaboratoryattheUniversidade Estadual de Ciências da Saúde de Alagoas (UNCISAL), in additiontodirectedhormonaltests,ultrasoundofthe gen-itourinary tract (GUT) and, if necessary, laparoscopy and gonadalbiopsy.
Investigation of the following genes was done in part-nership with the Grupo Interdisciplinar de Estudos da
Determinac¸ão e Diferenciac¸ão doSexo(GIEDDS) and Cen-trodeBiologiaMoleculareEngenhariaGenética(CBMEG)of theUniversidadeEstadualdeCampinas (UNICAMP): andro-gen receptor (AR), nuclear receptor subfamily 5, group
A, member 1 (NR5A1); steroid-5-alpha-reductase, alpha polypeptide 2 (SRD5A2); sex determining region Y (SRY);
cytochrome P450, family 21, subfamily A, polypeptide 2 (CYP21A2),andhydroxysteroid(17-beta)dehydrogenase3 (HSD17B3).
Casesofgenitourinary malformationswereclassifiedas genitourinary defects (GUD) and the others as Disorders of Sex Differentiation (DSD). The independent variables and their categories of analysis include the demographic and clinical characteristics and the genetic characteris-tics.Thecollecteddemographicandclinicalcharacteristics were: external genital morphology (ambiguous, feminine appearance, male appearance, or malformed), GUT find-ings (Müllerian derivatives, Wolffian derivatives, renal anomalies), age (<1; 1---9; 10---19; >19 years), how the child is raised (family definition of social gender role as male, female, or not defined, regardless of civil regis-tration), civil registration (male, female, unregistered), follow-up interruption/interruption reasons (change of address,death, withdrawal).Genetic characteristics eval-uatedwere:inbreeding,recurrenceandmaternalage≥35 years(yesorno),karyotype(46,XY;46,XX;other),presence ofpathogenicmutation/polymorphisminthestudiedgenes (yesorno).
DataweretabulatedandanalyzedusingMicrosoftExcel andEpi-InfoTMversion3.5.2softwares.Descriptiveanalysis
withfrequencydistribution,measuresofcentraltendency, anddispersionwasperformed.Fisher’sexacttest and chi-squarewereusedforanalysisof categoricalvariablesand Kruskal---Wallis test for equality of means. A significance levelof 5% (p<0.05)was considered. This study had ethi-calapproval on09/10/2013 (CAAE 17197113.8.0000.5013; Opinion390.134).
Results
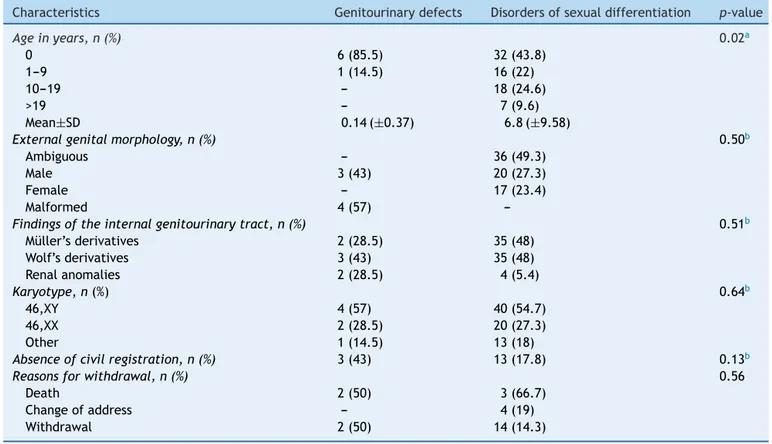
Among80GUAsubjectsinthesample,73(91%)weredefined ashavingDSDdiagnosedandtheotherashavingGUDalone orsyndromic.Table1showsthedistributionofgeneral char-acteristicsofsubjectsaccordingtothesegroups.
Theageatpresentationrangedfromzeroto38,with55 (69%)undersixyears.Theaverageagewasfourmonthsin GUDgroupand6.8yearsinDSDgroup(p<0.02).Inthe lat-ter,therewasameanagedistributiongradientinrelation tothegenitalmorphology,of2.9±6.4yearsinthe ambigu-ousgenitaliagroup,6.5±10.2yearsinthegenitaliaofmale appearance group, and 5.5±9.1 years in the genitalia of femaleappearancegroup(p<0.01).
Ambiguousgenitaliaoccurredin36(45%)cases,followed bygenitaliaofmaleappearance,femaleappearance,and malformed,withoutpreferential distributionbetweenDSD andGUDgroups.GUTwasevaluatedin75patients.Wolffian derivativeswerepresentin38(51%)subjects,sixofwhom hadassociatedrenalanomalies.
Table1 Distributionofdemographic,clinical,andcytogeneticcharacteristicsofsubjectsinrelationtodisordergroup. Characteristics Genitourinarydefects Disordersofsexualdifferentiation p-value
Ageinyears,n(%) 0.02a
0 6(85.5) 32(43.8)
1---9 1(14.5) 16(22)
10---19 --- 18(24.6)
>19 --- 7(9.6)
Mean±SD 0.14(±0.37) 6.8(±9.58)
Externalgenitalmorphology,n(%) 0.50b
Ambiguous --- 36(49.3)
Male 3(43) 20(27.3)
Female --- 17(23.4)
Malformed 4(57)
---Findingsoftheinternalgenitourinarytract,n(%) 0.51b
Müller’sderivatives 2(28.5) 35(48) Wolf’sderivatives 3(43) 35(48) Renalanomalies 2(28.5) 4(5.4)
Karyotype,n(%) 0.64b
46,XY 4(57) 40(54.7)
46,XX 2(28.5) 20(27.3)
Other 1(14.5) 13(18)
Absenceofcivilregistration,n(%) 3(43) 13(17.8) 0.13b
Reasonsforwithdrawal,n(%) 0.56
Death 2(50) 3(66.7)
Changeofaddress --- 4(19)
Withdrawal 2(50) 14(14.3)
aKruskal---Wallis.
b Fisher’sexacttest.
DSDandGUDgroupsforthepresenceofcytogenetic abnor-malities.
Table 2 shows the distribution of external and inter-nalgenitalmanifestationsinrelationtokaryotype.Genital ambiguitywasmorefrequentinthe46,XXgroup(p<0.006). Sixpatients withMüllerianderivatives hadYchromosome demonstrablebycytogeneticsormoleculartechnique.
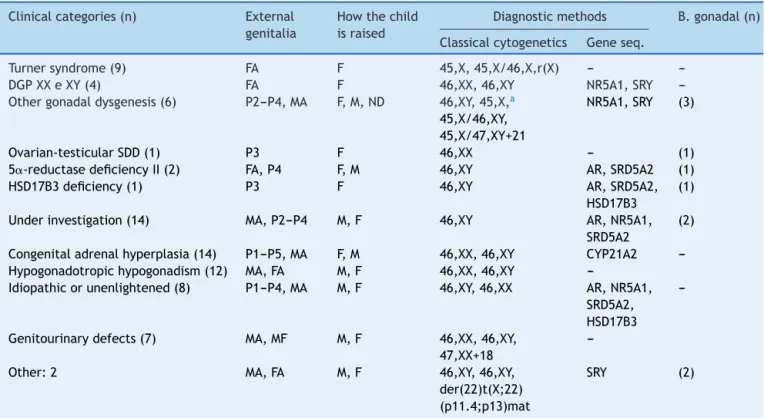
Table 3 shows the clinical categories. All found chro-mosomal abnormalities had pathogenic relationship with theirphenotypes.Regardingtheinvestigatedgenes, muta-tions/polymorphismswerefoundin15(18.8%)casestodate. Twenty-two (27.5%) patients remain under diagnostic investigation, only one of them with 46,XX karyotype. Among the rest, 14 have hormonal profile suggestive of defectinandrogensynthesisoractionandsevenremainas idiopathicorunclear.Nopathogenicmutationwasfoundso farinthegenesinvestigatedinthesesubjects.
Asagroup,thedisordersofgonadaldifferentiationwere the most common, accounted for 20 (25%) cases. Among these, it was found the largest number of cytogenetic abnormalities and oneof the lowest frequency of genital ambiguity.
Congenital adrenal hyperplasia was the most frequent nosologicaldiagnosis in the sample (17.5%). In this, asin thegroup of defectsin androgen synthesis or action, the highestfrequencyofgenitalambiguitywasfound.
Consanguinitywasfoundin11(16%)families,nine(12%) withrecurrence of the disorder, all from the DSD group. Maternalage≥35yearsoccurredineight(10%)cases,only oneoftheseinGUDgroup.
Sixteen(20%)childrenhadnocivilregistrationandonly one had the social gender role not defined, without sta-tistical differencesbetweenDSDandGUD groups(p<0.13) (Table1).However,thelackofcivilregistrationwashigher in cases of ambiguity or external genital malformation (p<0.02).
There was interruption of outpatient follow-up in 25 (31%)cases,mainlybywithdrawal.Thisresultdidnotdiffer betweenGUDandDSDgroups(Table1),aswellasbetween thoseliving inthe cityor in thecountry(p<0.20).On the otherhand,itwassignificantlylowerinpatientswithgenital ambiguityormalformedgenitalia(p<0.01).
Discussion
The SGC/HUPAA/UFALisareferral serviceforpeoplewith birthdefectsinthestatesince2003.Asurveyperformedin 2007oftheactionsinvolvedinthecareofpatientswith gen-italambiguityinthishospitalrevealedsomeobstaclessuch aslackofinformation,difficultaccesstotests, discontinua-tionoffollow-up,anddisconnectionbetweentheservices.16
The intention of changing thisreality determined in 2008 thebeginningofanintegratedoutpatientclinicofgenetics and psychoanalysisin the SGC/HUPAA/UFAL.17 The results
discussedherecomesfromthesystematiccareofpatients providedatthisclinic.
Table2 Distributionofsubjectsaccordingtoexternalandinternalgenitalscharacteristicsinrelationtokaryotype. Characteristics 46,XY
n(%)
46,XX n(%)
Othern(%) p-value Chi-square
Externalgenitalmorphology
Ambiguous 19(43.2) 15(68.1) 2(14.2)
Prader1 1(2.3) 1(4.5) ---Prader2 1(2.3) 2(9.1) 1(7.1) Prader3 5(11.3) 11(50) 1(7.1) Prader4 12(27.3) --- ---Prader5 --- 1(4.5)
---Male(micropenis,hypospadiasand/orcryptorchidism) 22(50) --- 1(7.1)
Female(normal,childorhypoplastic) 2(4.5) 5(22.8) 10(71.6)
Malformed 1(2.3) 2(9.1) 1(7.1)
Total 44(55) 22(27.5) 14(17.5) 0.006
Findingsofinternalgenitourinarytract <0.001
Müller’sderivatives 3(7.5) 22(100) 12(92.3) Wolf’sderivatives 37(92.5) --- 1(7.7)
Table3 Distributionofclinicalcategoriesaccordingtoexternalgenitalmorphology,howthechildisraised,anddiagnostic methodsused.
Clinicalcategories(n) External genitalia
Howthechild israised
Diagnosticmethods B.gonadal(n) Classicalcytogenetics Geneseq.
Turnersyndrome(9) FA F 45,X,45,X/46,X,r(X) --- ---DGPXXeXY(4) FA F 46,XX,46,XY NR5A1,SRY ---Othergonadaldysgenesis(6) P2---P4,MA F,M,ND 46,XY,45,X,a
45,X/46,XY, 45,X/47,XY+21
NR5A1,SRY (3)
Ovarian-testicularSDD(1) P3 F 46,XX --- (1) 5␣-reductasedeficiencyII(2) FA,P4 F,M 46,XY AR,SRD5A2 (1)
HSD17B3deficiency(1) P3 F 46,XY AR,SRD5A2, HSD17B3
(1)
Underinvestigation(14) MA,P2---P4 M,F 46,XY AR,NR5A1, SRD5A2
(2)
Congenitaladrenalhyperplasia(14) P1---P5,MA F,M 46,XX,46,XY CYP21A2 ---Hypogonadotropichypogonadism(12) MA,FA M,F 46,XX,46,XY
---Idiopathicorunenlightened(8) P1---P4,MA M,F 46,XY,46,XX AR,NR5A1, SRD5A2, HSD17B3
---Genitourinarydefects(7) MA,MF M,F 46,XX,46,XY, 47,XX+18
---Other:2 MA,FA M,F 46,XY,46,XY, der(22)t(X;22) (p11.4;p13)mat
SRY (2)
P1,ambiguousgenitaliaPradergradeI;P2,ambiguousgenitaliaPradergradeII;P3,ambiguousgenitaliaPradergradeIII;P4,ambiguous
genitaliaPradergradeIV;P5,ambiguousgenitaliaPradergradeV;MA,genitaliaofmaleappearance±micropenis,glandularhypospadias,
andcryptorchidism;FA,normalgenitaliaoffemaleappearance,infantileorhypoplastic;MF:malformedgenitalia;F,childraisedas
female;M,childraisedasmale;ND,notdefinedhowthechildisraised;AR,androgenreceptor;NR5A1,nuclearreceptorsubfamily5,
groupA,member1;SRD5A2,steroid-5-alpha-reductase,alphapolypeptide2;SRY,sexdeterminingregionY;CYP21A2,cytochromeP450,
family21,subfamilyA,polypeptide2;HSD17B3,hydroxysteroid(17-beta)dehydrogenase3.
population,13 this resultis notsurprising, as thecommon
practiceisnotreferringthesepatientsforetiological inves-tigation.Ontheotherhand,thesmallnumberofcaseswith syndromic GUD may reflect the rarity and severe clinical course of these conditions usuallyassociated with death. However,oncerecognized,thesecasesareusuallyreferred forevaluationatanearlyage,asseeninthiscohort.
DSDgroupwasheterogeneousregardingtheageof refer-ral and clinical manifestations. The observed distribution gradient revealed that in infants and prepubescent there is a predominance of cases of genital ambiguity or signs suggestiveofabnormalsexualdifferentiation (micropenis, bilateralcryptorchidism,microrquidia,hypospadias,clitoral hypertrophy,posteriorlabialfusion,palpablemassesinthe labioscrotalpouchesoringuinalregion).Inadolescentsand adults, the most prevalent manifestations were pubertal delay,atypicalpubertaldevelopment,andinfertility.These resultscorroboratetheliterature.4,6---8,11
Despite this, the wide age range in the group with ambiguous genitalia, which included teenagers and one adult, and the lack of prior treatment in six patients in thisgroupdrewattention.Thisresultmayreflectthe under-diagnosisandunderreportingofGUA,aswellastheaccess difficultyandthedisconnectionbetweenthehealthservices inthestate.17,18
The other clinical aspects evaluated----external and internal genital morphology and presence or absence of cytogeneticabnormalities----hadsimilarbehaviorinGUDand DSDgroups.Consistentwiththeliterature,theanalysisof thesecharacteristics revealed that,although therewasa predominanceofsubjectswithambiguousgenitalia,derived fromWolffand46,XYkaryotype,noneoftheseparameters alonemaybeconsideredfordeterminationofdiagnosisand treatment.4,6---8,10,11,19---21
Thegroupwithgenitalambiguityisparticularly illustra-tiveofthissituation.NotethatinindividualswithPrader1---3 genitalia,alltypesofkaryotypeweredetected,whereasin thePrader4groupallhadtheXYsexpairandinthePrader 5groupthe sexpairwasXX.Furthermore,theY chromo-some wasfound in patients withnormal female genitalia appearanceandinpatientswithMüllerianderivatives,which supportsthe need for the use of variousresources in the diagnosticapproachofGUA.4,6---8,10,11,19---21
Theestablishmentofthenosologicaldiagnosisis admit-tedly a challenge, especially in the group with 46, XY karyotype,due toextensive clinical and laboratory over-lap.Evenwiththeadventofmolecularbiologytechniques toapproachseveralgenes involved in sexdifferentiation, thefrequency ofcases withnodiagnosisranges from33% to80%.4,22---24 Inthepresent study,thefrequency of46,XY
caseswithoutanestablishednosologicaldiagnosisisinline withtheliteraturedata.Thecompletionofthesequencing ofgenesselectedtoreassessthisresultispending.
Groups of DGD and hypogonadotropic hypogonadism groups have in the karyotypeand hormoneprofile signifi-cantresourcesfordiagnosisdefinition.AmongtheDGD,the karyotypeallowsclarifyTurnersyndromeandmixedgonadal dysgenesis.Furthermore,gonadalbiopsy,indicated accord-ingtostrictcriteriaofcost-benefit,is instructiveincases ofovariotestisDSDandsomegonadaldysgenesis.However, thepresenceofrenalabnormalitiesandotherbirthdefects inpatients withhypogonadism shouldinferthe possibility
ofKallmannsyndrome.6,11Allthischaracteristicswereseen
thisstudy.
Accordingtoexpected,amongalldiagnosticgroups,the lowestfrequencyofdisagreementbetweengenital morphol-ogy, karyotype, and how the child is raised was seen in patientswithhypogonadismandTurnersyndrome,whereas thebiggestdisagreementsoccurredinthesynthesisdefects orandrogenactionandcongenitaladrenalhyperplasia.4,10,25
Thelatter,whichcorroboratestheliterature,wasthemost frequentnosologicaldiagnosis.26,27
Thehigh frequency of consanguinityandrecurrence of thedisorderintheDSDgroupcomplieswiththerecognized contributionofautosomalrecessiveconditionsinthe etiol-ogyofthesedisorders.24,26,28ItisnoteworthythattheState
ofAlagoashashighfrequencyofconsanguinity,whichfavors theappearanceofraredisorders,asshowninsomecasesof thissample.Maternalage≥35yearsisanincreasedrisk fac-torforchromosomalaneuploidies.28Thiscorrelationcanbe
inferredintwooftheeightcasesofthissample.
The biological complexity of sex differentiation in humansoverlapsthechallengingpsychological,social,and ethicalissuesinvolvedinthesepatients’management.Thus, for therapeutic planning, one should take into account, in additiontoetiologic diagnosis,howthe child israised, the anatomical conditions for external genital morphol-ogy repair, the possibility of spontaneous puberty, and fertility.4,6---8,10,11 Thedefinitionofthechild’ssocialgender
role and civil registration are particularly important and shouldbeanalyzedcomprehensively. Inthepresentstudy, afamilywaitedforclarificationofdiagnosistodefinehow thechildwouldberaisedandthecivilregistrationandbegan follow-upwith65daysoflife,withoutnamingthechild.
Thefamilydefinitionofhowachild israised regarding socialgender revealstheattributesof awish.Awishthat involves the imaginary representations that are made of thechild’sanatomicalsexandtheplaceitoccupiesinthe family.29Thus,thewayinwhicheachsubjectwillapprehend
thebodyitselfandtheconstructionofpsychosexuality fol-lowsthedefinitionofhowthechildisraised, andnotthe anatomicalandbiologicalsex.29Inthisregard,thestudyof
oneofthesamplecases,30basedonthepsychoanalytic
the-ory, showedthat givena propernametoa child putsthe child,byvirtueofthat,inoneofthesexes.
Regardingcivilregistration,itisimportanttonotethat it does not always follows the gender definition by the family,asoneoftheconductsinnewbornsistoguide par-ents towait for the diagnostic conclusion toregister the child.Atthesametime,thelackofcivilregistrationmakes the access to SUS difficult, as it makes it impossible to obtainthedocumentsrequiredforthenationalhealthcard thatprovidesaccesstotestsandprocedures.Inthisstudy, approximately1/5ofthechildrencametotheclinicwithout acivilregistration;themajoritywascasesofgenital ambi-guityormalformedgenitalia.This resultsuggeststhatthe mostsignificantfactor inthedecisiontoregister thechild is theexternalgenitalmorphology andindicatestheneed toreview theaccesscriteriatoSUSincases inwhich the medicalconditioninterferesinthecivilregistry.
withmultiple malformations of the GUDgroup, outcomes consistent withthe literature considering the severity of conditions.26---28Thewithdrawalcasesincludepatientswho
did not return and change of telephone numbers and addresses. An interesting point to note is that the dis-tancebetweenthefamilyhomeandthefollow-upservice did not affect the withdrawal. On the other hand, simi-lartowhatoccurswiththecivilregistration,theexternal genital morphology was a determining factor. The lower withdrawal rates were observed in patients with genital ambiguityormalformation.Theseresultshighlightthe psy-chosocialimpactofexternalgenitalanatomyandindicate the need for greater investmentin welcoming tofamilies andeffortstomaintainthefollow-upofpatientswithless severeabnormalitiesinviewoftheimplicationsofno treat-mentinpubertyandadulthood.
The overall results allowed us to know the profile of GUA patients treated at the SGC/HUPAA/UFAL. The gath-ered informationprovidesubsidiestoimprovetheclinical protocolsinordertofacilitateandstreamlinethe manage-mentofcasesandapproachesdecisionsbasedonevidence andspecifichealthneedsofindividuals.Twoimportant lim-itationsof thestudyarethelarge numberofcaseswhose follow-upwasdiscontinuedandcasesstillundiagnosedthat, inthisgroup,dependsheavilyontheinvestigationofgenes not yet available in the SUS. Despite this, an aspect of greatimportancewastheestablishmentofpartnershipswith researchinstitutionstoaccesstodiagnostictests.Locally, the challenge before us is the effective incorporation of other specialties in this proposal, in the perspectiveof a multidisciplinaryapproachintune withtheguidelinesand principles of the Política Nacional deAtenc¸ão Integral às PessoascomDoenc¸asRaras.
Funding
Fundac¸ão de Amparo à Pesquisa do Estado de Alagoas (Fapeal). Convênio Ministério da Saúde/CNPq/Sesau-AL/Fapeal. Processo: 60030 000714/2013. Conselho Nacional de Desenvolvimento Científico e Tecnológico ---Programa Interinstitucional de Bolsas de Iniciac¸ão Cientí-fica (CNPq/Pibic) and Edital Universal (CNPq), Processo: 484491/2013-0.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgements
We would like to thanks the patients and parents with-out whomthis studywould not bepossible; Dr.Rosemary Barbosa Marinhofor the willingness to performthe ultra-soundtests; Dr.Ricardo Luis Simões Houly andDrs. Maria EduardaBaíaCorreiadeOliveiraandRafaellaLimaBorges de Mendonc¸a of the Servic¸o de Anatomia Patológica do HospitalUniversitárioProfessorAlbertoAntunesofthe Uni-versidadeFederaldeAlagoas;Dr.GilGuerra-JuniorandDr. AndreaTrevasMaciel-Guerra,oftheGrupoInterdisciplinar de Estudos da Determinac¸ão e Diferenciac¸ão do Sexo da
UniversidadeEstadualdeCampinas; Dra.MaricildaPalandi deMellooftheLaboratóriodeGenéticaMolecularHumana doCentro deBiologiaMolecular eEngenhariaGenéticada UniversidadeEstadualdeCampinas.
References
1.Stevenson RE, Hall JG. Human malformations and related anomalies.2nded.NewYork:OxfordUniversityPress;2006.
2.WoodwardM,NeilsonA.Disordersofsexdevelopment.Surgery. 2013;31:646---51.
3.ConnellMT,OwenCM,SegarsJH.Geneticsyndromesandgenes involvedinthedevelopmentofthefemalereproductivetract: a possible role for gene therapy. J Genet Syndr Gene Ther. 2013;4:127.
4.Hughes IA. Disorders of sex development: a new defini-tionand classification.BestPractResClinEndocrinolMetab. 2008;22:119---34.
5.PraderA. Der genitalbefund beimpseudo-hermaphroditismus femininus des kongenitalen adrenogenitalen syndrome. Helv PaediatActa.1954;9:231.
6.HughesIA,HoukC,AhmedSF,LeePA,LWPESConsensusGroup; ESPEConsensusGroup.Consensusstatementonmanagementof intersexdisorders.ArchDisChild.2006;91:554---63.
7.Guerra-Júnior G, Maciel-GuerraAT. Therole ofthe pediatri-cianinthemanagementofchildrenwithgenitalambiguities.J Pediatr(RioJ).2007;83Suppl.5:S184---9.
8.BarbaroM,WedellA,NordenströmA.Disordersofsex develop-ment.SeminFetalNeonatalMed.2011;16:119---27.
9.KimKS,KimJ.Disordersofsexdevelopment.KoreanJUrol. 2012;53:1---8.
10.HiortO,BirnbaumW,MarshallL,WünschL,WernerR,Schröder T,etal.Managementofdisordersofsexdevelopment.NatRev Endocrinol.2014;10:520---9.
11.Ostrer H.Disordersofsexdevelopment(DSDs): anupdate.J ClinEndocrinolMetab.2014;99:1503---9.
12.FeldkampML,BottoLD,AmarE,BakkerMK,Bermejo-Sánchez E,BiancaS,etal.Cloacalexstrophy:anepidemiologicstudy fromtheInternationalClearinghouseforbirthdefects surveil-lance and research. Am J Med Genet C Semin Med Genet. 2011;157C:333---43.
13.MartinsAV,AraujoEJ,SouzaJA,ColombeliEM,LimaRM,Ramos TC.Tratamentocirúrgicodahipospádiadistal.ArqCatarinMed. 2013;42:54---9.
14.Brasil-MinistériodaSaúde.Portarian(199,de30deJaneiro
de 2014. Altera, acresce e revoga dispositivos da Portaria
n(199/GM/MS,de30dejaneirode2014,queinstituiaPolítica
Nacionalde Atenc¸ãoIntegralàs Pessoascom Doenc¸as Raras,
aprova as Diretrizes para Atenc¸ão Integral às Pessoas com
Doenc¸asRarasnoâmbitodoSistema ÚnicodeSaúde(SUS)e
instituiincentivosfinanceirosdecusteio.Brasília:Ministérioda
Saúde;2014.
15.GabrichPN,VasconcelosJS,DamiãoR,SilvaEA.Avaliac¸ãodas medidasdocomprimentopenianodecrianc¸aseadolescentes. JPediatr(RioJ).2007;83:441---6.
16.Zanotti SV, Xavier HV. Atenc¸ão à saúde de pacientes com ambiguidadegenital.ArqBrasPsicol.2011;63:82---91.
17.ZanottiSV,MonlleóIL.Psicanáliseegenética:umaexperiência deinterlocuc¸ãonoSUS.In: RudgeAM,BessetV,editors. Psi-canáliseeoutrossaberes.RiodeJaneiro:CiadeFreud/FAPERJ; 2012.
18.MonlleóIL,ZanottiSV,AraújoBP,CavalcanteEFJr,PereiraPD, Barros PM,et al. Prevalência de anormalidades genitais em recém-nascidos.JPediatr(RioJ).2012;88:489---95.
fromtheScottishGenitalAnomalyNetworkRegister.SexDev. 2011;5:103---8.
20.SureshD,CrawfordJ,AxelradME,GunnSK,McCulloughL,Smith OB,etal.Assessingsexassignmentconcordancewithgenotype andphenotype.IntJPediatrEndocrinol.2013:7.
21.Cox K, Bryce J, Jiang J, Rodie M, Sinnott R, Alkhawari M, et al. Novel associations in disorders of sex development: findings from the I-DSD Registry. J Clin Endocrinol Metab. 2014;99:E348---55.
22.Abdullah MA, Saeed U, Abass A, Lubna K, Weam A, Ali AS, etal.DisordersofsexdevelopmentamongSudanesechildren: 5-yearexperienceofapediatricendocrinologyclinic.JPediatr EndocrinolMetab.2012;25:1065---72.
23.VanderZwanYG,CallensN,vanKuppenveldJ,KwakK,DropSL, KortmannB,etal.Long-termoutcomesinmaleswithdisorders ofsexdevelopment.JUrol.2013;190:1038---42.
24.AhmedSF,BashambooA,Lucas-HeraldA,McElreaveyK. Under-standingthegeneticaetiologyinpatientswithXYDSD.BrMed Bull.2013;106:67---89.
25.InacioM [tesededoutorado]Aspectospsicossociaisesexuais depacientescomdistúrbiosdodesenvolvimentosexualalongo prazo.SãoPaulo(SP):FMUSP;2010.
26.WitchelSF,AzzizR.Congenitaladrenalhyperplasia.JPediatr AdolescGynecol.2011;24:116---26.
27.Speiser PW, Azziz R, Baskin LS, Ghizzoni L, Hensle TW, Merke DP, et al. Congenital adrenal hyperplasia due to steroid21-hydroxylase deficiency:anEndocrine Society clin-ical practice guideline. J Clin Endocrinol Metab. 2010;95: 4133---60.
28.Globalreporton birthdefects.Thehidden tollof dyingand disabledchildren.NewYork:MarchofDimesBirthDefects Foun-dation;2006.
29.CeccarelliPR.Ocorpocomoestrangeiro.IDEPsicanalisee Cul-tura.2008;31:54---60.