w w w . r b o . o r g . b r
Original
Article
Extracapsular
approach
for
arthroscopic
treatment
of
femoroacetabular
impingement:
clinical
and
radiographic
results
and
complications
夽
Bruno
Dutra
Roos
∗,
Milton
Valdomiro
Roos,
Antero
Camisa
Júnior,
Ezequiel
Moreno
Ungaretti
Lima,
Diego
Paulo
Gyboski,
Lucas
Schirmer
Martins
HospitalOrtopédicodePassoFundo,PassoFundo,RS,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory: Received23April2014 Accepted1August2014 Availableonline3July2015
Keywords: Femoroacetabular impingement/diagnosis Femoroacetabular impingement/etiology Femoroacetabular impingement/treatment Arthroscopy
a
b
s
t
r
a
c
t
Objectives:Toevaluatetheclinicalandradiographicresultsandcomplicationsrelatingto patientsundergoingarthroscopictreatmentforfemoroacetabularimpingementbymeans ofanextracapsularapproach.
Methods:BetweenJanuary2011andMarch2012,49patients(50hips)underwent arthro-scopictreatmentforfemoroacetabularimpingement,performedbythehipsurgeryteamof theOrthopedicHospitalofPassoFundo,RioGrandedoSul.Fortypatients(41hips)fulfilled alltherequirementsforthisstudy.Themeanfollow-upwas29.1months.Thepatientswere assessedclinicallybymeansoftheHarrisHipscore,asmodifiedbyByrd(MHHS),the Non-ArthriticHipscore(NAHS)andtheinternalrotationofthehip.Theirhipswerealsoevaluated radiographically,withmeasurementoftheCEangle,dimensionsofthejointspace,alpha angle,neck-headindex,degreeofarthrosisandpresenceofheterotopicossificationofthe hip.
Results:Outofthe41hipstreated,31(75.6%)presentedgoodorexcellentclinicalresults. Therewasameanpostoperativeincreaseof22.1pointsfortheMHHS,21.5fortheNAHSand 16.4◦fortheinternalrotationofthehip(p<0.001).Regardingtheradiographicevaluation, correctiontonormalvalueswasobservedforthealphaangleandneck-headindex,witha meanpostoperativedecreaseof32.9◦andmeanincreaseof0.10,respectively(p<0.001). Conclusion:Arthroscopictreatmentoffemoroacetabularimpingementbymeansofan extra-capsularapproachpresentedsatisfactoryclinicalandradiographic resultsovera mean follow-upof29.1months,withfewcomplications.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
夽
WorkperformedattheHospitalOrtopédicodePassoFundo,CentrodeEstudosOrtopédicos,FaculdadedeMedicina,Universidadede PassoFundo,PassoFundo,RS,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](B.D.Roos).
http://dx.doi.org/10.1016/j.rboe.2015.06.011
Abordagem
extracapsular
para
tratamento
artroscópico
de
impacto
femoroacetabular:
resultados
clínicos,
radiográficos
e
complicac¸ões
Palavras-chave: Impacto
femoroacetabular/diagnóstico Impacto
femoroacetabular/etiologia Impacto
femoroacetabular/tratamento Artroscopia
r
e
s
u
m
o
Objetivos: Avaliar os resultados clínicos e radiográficos e as complicac¸ões relativos a pacientessubmetidosatratamentoartroscópicodeimpactofemoroacetabularcomouso daabordagemextracapsular.
Métodos:Entrejaneirode2011emarc¸ode2012,49pacientes(50quadris)foramsubmetidosa tratamentoartroscópicodeimpactofemoroacetabularpelaEquipedeCirurgiadoQuadrildo HospitalOrtopédicodePassoFundo(RS).Preencheramtodososrequisitosnecessáriospara estetrabalho40pacientes(41quadris).Oseguimentomédiofoide29,1meses.Ospacientes foramavaliadospeloHarrisHipScoremodificadoporByrd(MHHS),Non-ArthriticHipScore (NAHS)equantoàrotac¸ãointernadoquadril.Tambémforamavaliadosradiograficamente. Aferiu-seoânguloCE,adimensãodoespac¸oarticular,oânguloalfa,oíndicecolo-cabec¸a, ograudeartroseeapresenc¸adeossificac¸ãoheterotópicadoquadril.
Resultados: Dos41quadristratados,31(75,6%)apresentaramresultadosclínicosbonsou excelentes.Observou-seumaumentomédiopós-operatóriode22,1pontosparaoMHHS, 21,5paraoNAHSe16,4◦narotac¸ãointernadoquadril(p<0,001).Quantoàavaliac¸ão radio-gráfica,observou-secorrec¸ãoparaíndicesconsideradosnormaisdoânguloalfaeíndice colo-cabec¸a,comdiminuic¸ãomédia de 32,9oe aumentomédiopós-operatóriode 0,10, respectivamente(p<0,001).
Conclusão:Otratamentoartroscópicodoimpactofemoroacetabularcomousodaabordagem extracapsularapresentouresultadosclínicoseradiográficossatisfatóriosemseguimento médiode29,1meses,compoucascomplicac¸ões.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Femoroacetabularimpingement(FAI)istodayrecognizedasa frequentlyoccurringconditionofhippainamongtheyoung population, withpossibledegenerative consequences.Both ofthe knownmechanismsforimpingement(camor inclu-sionandpincerorimpaction)arerelatedtopain,restriction oftherangeofmotionanddiminishedtoleranceofexercise amongtheindividualsaffected.1–7 Severalstudieshavenow suggestedthatsomeofthehiposteoarthrosiscasesthat previ-ouslywereconsideredtobeidiopathicaresecondarytoFAI.1–3 Conservativetreatmentcanbeattemptedfirstandconsists ofmodificationofhigh-impactphysicalactivities,avoidance ofload-bearingactivitiesassociatedwithexcessiveflexional andtorsionalmovements(whichwouldincreasethedemand on the joint) and lastly, use ofanti-inflammatory drugs.4,7 When the conservative treatment only brings temporary relief,surgicaltreatmentisindicated.4,7 Someauthors have statedthatbecausethisisamechanicalpathological condi-tion,delayingsurgicaltreatmentofFAImaynotbebeneficial forthepatient. However,thereisstill noconsensusinthe literatureinrelationtothismatter.1–7
In 1988, Dorfmann et al.8 described subdivision of the hipjoint into twocompartmentslimited bythe acetabular labrum: the central and peripheral compartments. Within thisconcept,thecompartmentsareaccessedarthroscopically indifferentmanners.Thecentralcompartmentisaccessed throughapplicationoftractiontothelowerlimbinorderto allowinspectionoftheintra-articularspace.8Morerecently,
thelateralcompartmentofthehipwasdescribedsuchthat this enabled viewingofthe peritrochantericspace and the sciaticnerve.9
Arthroscopic treatmentofFAIhas beenwidely dissemi-natedbecausethispresentsrapidrehabilitationandprovides good access to the hip joint. Some forms of arthroscopic accesstothispathologicalconditionhavebeendescribedin theliterature.Whatdifferentiatesthesemethodsisthejoint compartmentthatwouldbeaccessedfirst.Theapproachwith aninitialaccesstothecentralcompartmentistheformmost commonlydescribed.4–7Inarthroscopicapproacheswith ini-tialaccesstotheperipheralcompartment(intracapsularand extracapsularapproaches),afterfirstaccessingthis compart-ment,traction isappliedto thelimbinorderthe view the centralcompartment.10–13
Theobjectiveofthepresentstudywastoevaluatethe clin-ical and radiographicresults and complicationsrelating to patientsundergoingarthroscopictreatmentforFAIusingan extracapsularapproach.
Materials
and
methods
arthroscopic treatment with initial access to the central compartment (four cases); loss from follow-up (one case); follow-uplessthan12months(nocases).Allthepatientswere calledbackforreassessment.Thisstudywasapprovedbythe researchethicscommittee.
Inaccordancewiththecriteriaestablished,40patients ful-filledallthenecessaryrequisites.Ofthese,36(87%)weremale. Themeanagewas36.12years(SD=9.1;range:21–47years). Therighthipwasoperatedin20cases(48.78%)andtheleft hipin21cases(51.21%).Onecasewastreatedbilaterally,at differenttimes.
Regarding clinical matters, the patients were evaluated beforeandaftertheoperationusingtheHarrisHipScore,as modifiedbyByrd14(MHHS),Non-ArthriticHipScore15(NAHS) andthedegreeofinternalrotationofthehipaffected(with theuseofagoniometerformeasurements).
From the Harris Hip Score as modified by Byrd,14 the resultswerestratifiedaspoor(MHHS<70points),fair(MHHS 70–79points),good(MHHS80–89points)andexcellent(MHHS 90–100).4
Allthepatientswereevaluatedbymeansofradiographs (anteroposterior(AP)viewofthepelviswiththepatient stand-ingupright,Dunn45◦,Dunn90◦andLequesnefalseprofile),16 andalsomagneticresonanceimaging(MRI)inorderto diag-nose chondral and labral lesions. FAI of pincer type was diagnosedthroughmeasuringthedegreeofcoverageofthe femoralheadandacetabularversiononAPradiographsofthe pelvisintheuprightstandingpositionandLequesnefalse pro-file.FAIofcamtypewasdefinedasanalphaanglegreaterthan 50◦onDunn45◦radiographs.17
The following were measured before the operation: Tönnis18 classification for coxarthrosis; center-edge angle (CE); dimensionofthe smallestjoint spacein millimeters
inAPviewofthepelvisintheuprightstandingposition16,18; alphaangle,asdescribedbyMeyerinDunn45◦view17(˛);and
head-neckindex(HNI)inDunn90◦view.16Lateinthe post-operativeperiod,tomakecomparisonswiththepreoperative measurements,thedimensionofthesmallestjointspacein millimeters(˛)wasmeasured.Inaddition, thepresenceof
heterotopicossificationofthehipwasevaluatedinaccordance withBrookeretal.19Toavoidinterandintraobservererrors, themeasurementswerefollowedupbytwosurgeonsfromthe hipgroup.Intheeventofdiscordanceofmorethan3◦inthe angularmeasurementsor1mmintheminimumjointspace, anewevaluationwasmade,thistimebyathirdsurgeon,and fromthisaconsensuswasreachedregardingthe measure-ment.Itwasconsideredthatthemeanmagnificationofthe APradiographsofthepelviswas15%,andthiswasquantified ontheequipmentatthehospitalservice.
Thestatisticalmethodusedforanalyzingthepaired vari-ables(MHHS,NAHS,internalrotation,˛andHNIbeforeand
aftertheoperation)wastheMann–Whitneytest.Theresults wereconsideredtobestatisticallysignificantwhenp<0.05.
Surgical
technique-extracapsular
arthroscopic
approach
Theextracapsularapproachinitiallyaccessedtheperipheral compartmentand,justlikethe arthroscopicapproachwith
initial accessto the central compartment, it could be per-formed withthe patient inthe supineor lateral decubitus position.Standardequipmentforhiparthroscopy,suchas30◦ and 70◦ viewing devices,specificcannulae, radiofrequency, shavers,radioscopyandatractiontablewereused.
The extracapsular approach followed the access to the peripheralcompartmentdescribedbySampson10and Horis-bergeretal.11ThistechniquebecamepopularinSpainunder thename“fromoutsidetoinside”.12Itisdifferentiatedfrom theintracapsularapproach13(whichbeginsintheperipheral compartmentinternally tothejoint capsule)sinceit starts externallytothehipcapsule.
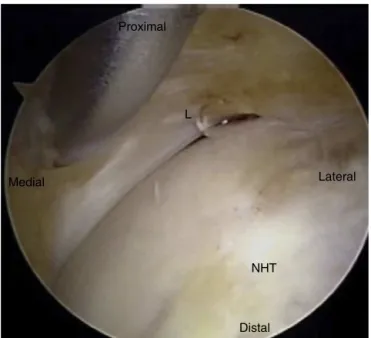
With the hip extendedand usingtwo arthroscopic por-tals, the anterior joint capsule and iliocapsularis muscle weredissectedusingradiofrequencyandashaver,until ade-quateexposurehadbeenachieved.Identificationofthereflex portionoftherectusfemorismusclemarkedthelocationof the acetabular labrum (Fig. 1). Capsulotomy wasthen per-formedlongitudinallyasfarasthefemoralneck,whichmay alsobeextendedasnecessaryduringtheoperation(Fig.2). Capsulectomy was then performed, followed by femoral and/oracetabularosteochondroplasty.Thelimbwasplaced undertractionatthetimeofinspectionofthecentral com-partmentandlabralrefixationwhennecessary,inaccordance withFryerandDomb20(Fig.3).Aftertheprocedure,suturing ofthecapsulecouldbedoneifnecessary.
Proximal
RF
Medial
Lateral
JC
Distal
Proximal
L
Lateral Medial
NHT
Distal
Fig.2–Imageduringoperation,afterthecapsulehasbeen opened,identifyingthelabrumofthehip(L)andthe femoralneck-headtransition(NHT).
Aftertheoperation,weadvisedthatweightcouldbe par-tiallyborneonthelimb,withuseoftwocrutchesforthree weeks.Followingthis,full-weight-bearingwasallowed. Exer-cisesonabicycleorinaswimmingpoolwerestarted15days aftertheoperation.Physiotherapyforstrengtheningofthehip flexorandabductormuscleswasstartedthreeweeksafterthe
Proximal FH
FN
Distal
Medial Lateral
Fig.3–Imageduringoperationshowingresectionofthe cam-typedeformityandidentifyingthefemoralhead(FH) andfemoralneck(FN).
operation.Therehabilitationcanbechangedaccordingtothe patient’sstateofpain.Weusedprophylaxisagainst hetero-topicossificationconsistingofnaproxenfor30days.
The main theoretical advantages of arthroscopic approacheswithinitialaccesstotheperipheralcompartment are the lower risk of iatrogenic injury to the labrum and jointcartilage,shortertimeundertractionandeaseofaccess to the joint whenthe traction on the limbdoes notallow initialaccesstothecentralcompartment(prominentanterior acetabularwallorpresenceofanossifiedlabrum).10–13
Results
InrelationtotheevaluationoftheMHHSclinicalscore,the preoperativemeanwas65points(SD=9.8;range:38–77points) and the postoperative mean was 88 points (SD=11;range: 60–100points),i.e.withapostoperativeincreaseinthemean of22.1points.Inaccordancewiththecriteriaestablished,31 cases(75.60%)presentedgoodorexcellentclinicalresults,8 (19.51%)had fairresultsandthree(7.31%)hadpoorresults. RegardingtheNAHSclinicalscore,thepreoperativemeanwas observedtobe68.8points(SD=12.5;range:45–80points)and thepostoperativemeanwas92.5points(SD=10;range:60–100 points),i.e.withapostoperativeincreaseinthemeanof21.5 points.Theinternalrotationmeasurementsonthehip pre-sented apreoperative mean of 5◦ (SD=10◦; range: −15◦ to 30◦)andapostoperativemeanof20◦ (SD=12.5◦;range:5◦to 40◦),i.e.withapostoperativeincreaseinthemeanof16.4◦. Itwasseenthattherewerestatisticallysignificantdifferences (p<0.001)intheMHHSandNAHSclinicalscoresandhip inter-nalrotationmeasurements,frombeforetoaftertheoperation. Twenty-ninehips(70.73%)wereclassifiedaspresentingFAI ofcamtypeandtwelve(28.27%)asFAIofmixedtype.During thearthroscopicsurgicaltreatment,20cases(48.78%) under-wentfemoralosteochondroplastyalone.Intheremaining21 cases(51.21%),this wasassociatedwithother complemen-tary procedures such as: acetabular osteochondroplasty in the mixedFAIcases(12cases;29.26%);debridement ofthe labrum(sevencases;17.07%);acetabularchondral microfrac-ture in Outerbridge grade 4 chondral lesions (four cases; 9.75%);andlabralrefixationasindicatedbyFryandDomb20 (fivecases;12.19%).Themeanlengthoffollow-up was29.1 months(SD=12.4;range:12–36months).
Inrelationtothepreoperativeradiographicevaluation,13 cases(31.7%)wereclassifiedasarthrosisofTönnisgrade0;21 (51.21%)asTönnis1;7(17.07%)asTönnis2;andnoneas Tön-nis3.ThemeanCEwas35.78◦(27◦–46◦).Noneofthepatients presentedCElessthan25◦(suggestiveofdevelopmental dys-plasiaofthehip).Thepreoperativemeanforthemeasurement ofthesmallestjointspacewas3.31mm(range:2–4mm)and therewas nostatisticallysignificantdifference in compari-sonwiththelatepostoperativemeasurement(p=1.000).None ofthepatientspresentedpreoperativemeasurementsofthe smallestjointspacethatwerelessthan2mm.Regarding˛,
Fig.4–Malepatientaged32years.Preoperativeinternalrotationof5◦.(A,B)PreoperativeradiographsshowingFAIofcam type,CE:27◦and˛:68◦.(C,D)Radiographsproduced3yearsand2monthsaftertheoperation,inwhichfemoral
osteochondroplastyhadbeenperformedinassociationwithlabraldebridement.Thepatientevolvedwell,tointernal rotationof18◦,withnormalizationof˛.
(SD=0.1;range:0.16–0.32).Statisticallysignificantdifferences (p<0.001)betweenthepreoperativeandpostoperative mea-surementsof˛andHNIwereobserved.Inlatepostoperative
assessments,noheterotopicossificationwasobservedin36 cases(87.80%),whilefourcases(9.75%)presentedossification classifiedasgrade1byBrooker19andonecase(2.43%)asgrade 3(Table1).
Ascomplications,wefoundonecase(2.43%)ofdeepvein thrombosis,onecase(2.43%)ofheterotopicossification classi-fiedasgrade3byBrooker19andonecase(2.43%)oftransitory paresthesiaofthepudendalnerve(withregression2months afterthe operation).Two cases(4.87%)presentedpersistent pain,andoneofthesenowhasbeenindicatedfortotalhip arthroplasty.Bothofthesecaseswerepatientswitharthrosis ofTönnisgrade2(Figs.4and5).
Discussion
The surgical treatment of FAI is based on remodeling the proximal femur and acetabulum, along with treatment of thechondralandlabrallesions,withtheaimofdiminishing the impingementofthefemurontheedgeofthe acetabu-lumandconsequentlyimprovingtherangeofmotionofthe hip.1–4
Fig.5–Malepatientaged37years.Internalrotationof0◦.(A,B)PreoperativeradiographsshowingFAIofmixedtype,CE:
32◦,˛:78◦andcrossingoftheacetabularlines.(C,D)Radiographsproduced1yearand3monthsaftertheoperation,in whichfemoralosteochondroplastyhadbeenperformedinassociationwithlabralrefixation.Thepatientevolvedwell,to internalrotationof15◦,withnormalizationof˛.
beenpositivewithregardtosymptomreliefandimprovement ofhip mobilityand thelevelofphysicalactivity,andthese suggestthatoverthelongterm,thejointwillbepreserved.1–4 Among the traditional techniques for treating FAI, the hipdislocationtechniquedescribedandpopularizedbyGanz etal.3iscurrentlyconsideredtobethegoldstandardfor treat-ingthispathologicalcondition.Thistechniqueprovideswide accesstotheacetabulumandfemurforrepairinganatomical abnormalitiesandisalsoconsideredtobeasafetechnique thatenablespreservationofthevascularizationofthefemoral head. However, the accompanying rehabilitation period is long,incomparisonwitharthroscopictechniques,21and com-plicationssuchaspseudarthrosisofosteotomyofthegreater trochantermayoccur,withthepossibilityoftheneedforanew surgicalinterventiontoremovethesynthesismaterial.1–4,21,22
Table1–Comparisonbetweenpreoperativeand postoperativeclinicalandradiographicmeasurements.
Evaluation Interquartile range
p
MHHS Preoperative 65.0 9.8 <0.001 Postoperative 88.0 11.0
NAHS Preoperative 68.8 12.5 <0.001 Postoperative 92.5 10.0
IR Preoperative 5.0 10.0 <0.001 Postoperative 20.0 12.5
˛ Preoperative 76.0 11.0 <0.001 Postoperative 44.0 12.5
mm Preoperative 3.0 1.0 1.000 Postoperative 3.0 1.0
HNI Preoperative 0.10 0.0 <0.001 Postoperative 0.20 0.1
MHHS,modifiedHarrisHipscore;NAHS,non-arthritichipscore; IR,internalrotationofthehip;˛,alphaangle;mm,dimensionof smallestjointspaceinmillimeters;HNI,head-neckindex.
constructing the portals. For example, these complica-tions may include injury to the lateral femoral cutaneous nerve or, more rarely, to the pudendal and sciatic nerves (0–12.9%).1–7,10–13
Philliponetal.6usedthearthroscopictechniquewithinitial accesstothecentralcompartmenttotreatFAIin112patients, withameanfollow-upof2.3years,andfoundthattherewas ameanincreaseintheMHHSof24points,without compli-cations.In arecent paper, Byrdand Jones4 usedthe same techniqueon100hips,withaminimumfollow-upof2years, andfoundthat79%oftheresultsweregoodorexcellent,with complicationsobservedin3%ofthecases.Inthe Brazilian literature,Poleselloetal.7publishedtheresultsfrom28hips thatweretreatedarthroscopically,withameanfollow-upof27 months,amongwhich15%weregoodand85%wereexcellent, withoutcomplications.
Dienstetal.23publishedtheresultsfrom48patientswho underwentarthroscopictreatmentofFAIbymeansofan intra-capsularapproach(i.e.withinitialaccesstothe peripheral compartment),withameanfollow-upof18months.Itwas foundthattheNAHSshowedameanincreaseof21points; therewerefewcomplications(4.2%);andtherewasonecase ofconversion to totalhip arthroplasty. Horisberger et al.11 appliedtheextracapsulararthroscopictechniqueto105hips in88patients,withameanfollow-upof2.3years,andfounda meanpostoperativeincreaseinNAHSof28points,witha com-plicationscomprisingneuropraxiaofthesciaticorpudendal nervein1.9%andneuropraxiaofthelateralcutaneousnerve ofthethighin11%.In8.6%ofthecases,therewasaneedto converttohiparthroplasty.
Inourstudy,weobtainedresultssimilartothosedescribed inthe literature.Weobservedpostoperative improvements in the clinical evaluations on the patients, suchthat they achievedadaptationstolevelsthatareconsideredtobe nor-malinrelationtotheradiographicpatternsmeasured,with maintenanceofthejointspace.Weneedtofollowupthese patientsforalongertimeinordertoaffirmwhetherthe clin-ical results and joint preservation after the operation will continuetobesatisfactory.
Thelimitationsofthepresentstudywerethesmallnumber ofpatients,thepredominanceofmalepatientsandtheshort meanlengthoffollow-up(29.1months).
Itisimportanttoemphasizethataffirmationthatchondral preservationinthehipjoint hasbeen achievedafter surgi-calcorrectionofFAIstillremainsamatterofcontroversyin theliterature.AlongitudinalstudybyHartofilakidisetal.,24 withfollow-upofupto40yearsamongasymptomaticpatients withthemorphologyofFAI,demonstratedthatevenwithout treatment,evolutiontoosteoarthrosisdoesnotoccur invari-ably(82.3%didnotpresentarthrosisafterameanfollow-upof 18.5years).Betterunderstandingofthenaturalhistoryofthis pathologicalconditionandidentificationofthemorphotypes ofFAIthathaveahigherchanceofevolvingtocoxarthrosis canbeexpectedtoprovideanswerstotheverymany ques-tionsthatcurrentlyexistandtohelpinfutureimprovement ofthebestindicationsforitstreatment.
Conclusion
Theclinicalandradiographicresultsfromarthroscopic treat-mentofFAIusinganextracapsularapproachweresatisfactory overameanfollow-upof29.1months,withfewcomplications.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.MatsudaDK,CarlisleJC,ArthursSC,WiekrsCH,PhilliponMJ. Comparativesystematicreviewoftheopendislocation, mini-open,andarthroscopicsurgeriesforfemoroacetabular impingement.Arthroscopy.2011;27(2):252–69.
2.GanzR,ParvizziJ,BeckM,LeuningM,NoltzliH,Siebenrock KA.Femoroacetabularimpingement:acausefor
osteoarthritisofthehip.ClinOrthopRelatRes. 2003;(417):112–20.
3.GanzR,GillTJ,GautierE,GanzK,KrugelN,BerlemannU. Surgicaldislocationoftheadulthip.Atechniquewithfull accesstothefemoralheadandacetabulumwithouttherisk ofavascularnecrosis.JBoneJointSurgBr.2001;83(8):1119–24.
4.ByrdJW,JonesKS.Arthroscopicmanagementof
femoroacetabularimpingement:minimum2-yearfollow-up. Arthroscopy.2011;27(10):1379–88.
5.ByrdJW.Hiparthroscopyutilizingthesupineposition. Arthroscopy.1994;10(3):275–80.
6.PhilipponMJ,BriggsKK,YenKM,KuppersmithDA.Outcomes followinghiparthroscophyforfemoroacetabular
impingementwithassociatedchondrolabraldysfunction: minimumtwoyearsfollowup.JBoneJointSurgBr. 2009;91(1):16–23.
7.PoleselloGC,QueirozMC,OnoNK,HondaEK,GuimarãesRP, RicioliJuniorW.Tratamentoartroscópicodoimpacto femoroacetabular.RevBrasOrtop.2009;44(3):230–8.
8.DorfmannH,BoyerT,HenryP,DeBieB.Asimpleapproachto hiparthroscopy.Arthroscopy.1988;4(2):2.
10.SampsonTG.Arthroscopictreatmentoffemoroacetabular impingement.TechOrthop.2005;20(1):56–62.
11.HorisbergerM,BrunnerA,HerzogRF.Arthroscopictreatment offemoroacetabularimpingementofthehip:anew
techniquetoaccessthejoint.ClinOrthopRelatRes. 2010;468(1):182–90.
12.MargaletE,MediavillaI,MarínO.Nuevoabordajeartroscópico delacirugíadecadera:técnicaout-inside.Cuadernos Artroscopia.2010;41(1):27.
13.DienstM,SeilR,KohnDM.Safearthroscopicaccesstothe centralcompartmentofthehip.Arthroscopy.
2005;21(12):1510–4.
14.GuimarãesRP,AlvesDPL,AzuagaTL,OnoNK,HondaE, PoleselloGC,etal.Traduc¸ãoeadaptac¸ãotransculturaldo HarrisHipScoremodificadoporByrd.ActaOrtopBras. 2010;18(6):339–42.
15.ChristensenCP,AlthausenPL,MittlemanMA,LeeJA, McCarthyJC.Thenonarthritichipscore:reliableand validated.ClinOrthopRelatRes.2003;7(406): 5–83.
16.ClohisyJC,CarlisleJC,BeauléPE,KimYJ,TrousdaleRT,Sierra RJ,etal.Asystematicapproachtotheplainradiographic evaluationoftheyoungadulthip.JBoneJointSurgAm. 2008;90Suppl4:47–66.
17.MeyerDC,BeckM,EllisT,GanzR,LeunigM.Comparisonof sixradiographicprojectionstoassessfemoralhead/neck asphericity.ClinOrthop.2006;(445):181–5.
18.BusseJ,GasteigerW,TönnisD.Anewmethodfor roentgenologicevaluationofthehipjoint–thehipfactor. ArchOrthopUnfallchir.1972;72(1):1–9.
19.BrookerAF,BowermannJW,RobinsonRA,RileyRHJr.Ectopic ossificationfollowingtotalhipreplacement.Incidence,and methodofclassification.JBoneJointSurgAm.
1973;55(8):1629–32.
20.FryR,DombB.Labralbaserefixationinthehip:rationaleand techniqueforananatomicapproachtolabralrepair. Arthroscopy.2010;269suppl:S81–9.
21.BotserIB,SmithTW,NasserR,DombBG.Opensurgical dislocationversusarthroscopyforfemoroacetabular impingement:acomparisonofclinicaloutcomes. Arthroscopy.2011;27(2):270–8.
22.BeckM,LeuningM,ParvizziJ,BoutierV,WyssD,GanzR. Anteriorfemoroacetabularimpingement:partII.Midterm resultsofsurgicaltreatment.ClinOrthopRelatRes. 2004;(418):67–73.
23.DienstM,KusmaM,SteimerO,HolzhofferO,KohnD. Arthroscopicresectionofthecamdeformityof
femoroacetabularimpingement.OperOrthopTraumatol. 2010;22(1):29–43.
24.HartofilakidisG,BardakosNV,BabisGC,GeorgiadesG.An examinationoftheassociationbetweendifferent morphotypesoffemoroacetabularimpingementin