REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
OfficialPublicationoftheBrazilianSocietyofAnesthesiologywww.sba.com.br
REVIEW
ARTICLE
Perioperative
cardiac
arrest:
an
evolutionary
analysis
of
the
intra-operative
cardiac
arrest
incidence
in
tertiary
centers
in
Brazil
Matheus
Fachini
Vane
a,∗,
Rafael
Ximenes
do
Prado
Nuzzi
a,
Gustavo
Fabio
Aranha
a,
Vinicius
Fernando
da
Luz
a,
Luiz
Marcelo
Sá
Malbouisson
a,
Maria
Margarita
Castro
Gonzalez
b,
José
Otávio
Costa
Auler
a,
Maria
José
Carvalho
Carmona
aaDisciplineofAnesthesiology,HospitaldasClínicasdaFaculdadedeMedicinadaUniversidadedeSãoPaulo,SãoPaulo,SP,Brazil bHeartInstitue(InCor),HospitaldasClínicasdaFaculdadedeMedicinadaUniversidadedeSãoPaulo,SãoPaulo,SP,Brazil
Received14April2014;accepted26June2014 Availableonline7February2015
KEYWORDS
Intra-operative complications; Heartarrest; Cardiopulmonary resuscitation; Anesthesia
Abstract
Background: Greatchangesinmedicinehavetakenplaceoverthelast25yearsworldwide. Thesechangesintechnologies,patientrisks,patientprofile,andlawsregulatingthemedicine haveimpactedtheincidenceofcardiacarrest.Ithasbeenpostulated thattheincidenceof intraoperativecardiacarresthasdecreasedovertheyears,especiallyindevelopedcountries. The authorshypothesizedthat, asintherest ofthe world,theincidenceofintraoperative cardiacarrestisdecreasinginBrazil,adevelopingcountry.
Objectives:The aimofthisstudy was tosearchthe literaturetoevaluate thepublications thatrelatetheincidenceofintraoperativecardiacarrestinBrazilandanalyzethetrendinthe incidenceofintraoperativecardiacarrest.
Contents:Therewere4articlesthatmetourinclusioncriteria,resultingin204,072patients undergoingregionalorgeneralanesthesiaintwo tertiaryandacademichospitals,totalizing 627casesofintraoperativecardiacarrest.Themeanintraoperativecardiacarrestincidence forthe25yearsperiodwas30.72:10,000anesthesias.Therewasadecreasefrom39:10,000 anesthesiasto13:10,000anesthesiasintheanalyzedperiod,withtherelatedlethalityfrom 48.3%to30.8%.Also,themaincausesofanesthesia-relatedcauseofmortalitychangedfrom machinemalfunctionanddrugoverdosetohypovolemiaandrespiratorycauses.
Conclusions:Therewasaclearreductionintheincidenceofintraoperativecardiacarrestin thelast25yearsinBrazil.Thisreductionisseenworldwideandmightbearesultofmultiple
∗Correspondingauthor.
E-mail:[email protected](M.F.Vane).
http://dx.doi.org/10.1016/j.bjane.2014.06.007
factors, includingnewlawsregulatingthemedicineinBrazil,incorporationoftechnologies, betterhumandevelopmentlevelofthecountry,andbetterpatientcare.
© 2014SociedadeBrasileirade Anestesiologia.Publishedby ElsevierEditoraLtda.Allrights reserved.
PALAVRAS-CHAVE
Complicac¸ões intraoperatórias; Paradacardíaca; Reanimac¸ão cardiopulmonar; Anestesia
Paradacardíacaperioperatória:umaanáliseevolutivadaincidênciadeparada cardíacaintraoperatóriaemcentrosterciáriosnoBrasil
Resumo
Justificativa: Nosúltimos25anosocorreramgrandesmudanc¸asnamedicinaemtodoomundo. Essasmudanc¸asdetecnologias,riscosdopaciente,perfildopacienteeleisqueregulam medica-mentostiveramimpactonaincidênciadeparadacardíaca(PC).Postula-sequeaincidênciade parada cardíaca intraoperatória (PCI)tem diminuído ao longodos anos, especialmente em paísesdesenvolvidos.Anossahipótesfoique,comonorestodomundo,aincidênciadePCI estádiminuindonoBrasil,umpaísemdesenvolvimento.
Objetivos: Oobjetivo deste estudofoi pesquisareavaliar naliteraturaaspublicac¸ões que relacionamaincidênciadePCInoBrasileanalisaratendêncianaincidênciadePCI.
Conteúdo: Descobrimosquatroartigosqueatenderamoscritériosdeinclusão,resultandoem 204.072 pacientes submetidos à anestesia regional ou geral em dois hospitais terciários e acadêmicos,totalizando 627casos dePCI.A médiade incidênciadePCI para operíodode 25 anosfoide30,72:10.000anestesias.Houveumadiminuic¸ãode39:10.000anestesiaspara 13:10.000anestesiasnoperíodoanalisado,comletalidaderelacionadade48,3%para30,8%. Alémdisso,asprincipaiscausasdemortalidaderelacionadasàanestesiamudaramdemau fun-cionamentodemáquinaseoverdosedemedicamentosparahipovolemiaecausasrespiratórias. Conclusões: Houveumaclarareduc¸ãonaincidênciadePCInosúltimos25anosnoBrasil.Essa reduc¸ão éobservadaem todoo mundo epode sero resultadode vários fatores,incluindo novasleisqueregulammedicamentosnoBrasil,incorporac¸ãodetecnologias,melhornívelde desenvolvimentohumanodopaísemelhorassistênciaaopaciente.
©2014SociedadeBrasileira deAnestesiologia.PublicadoporElsevierEditoraLtda.Todosos direitosreservados.
Introduction
Cardiacarrest(CA)isthemostseriouspotentiallyreversible adverse event that can be present in the perioperative period setting. It is assumed that in-hospital arrest is an eventthathas greaterchance ofsurvival thaninpatients admittedforothermedicalconditions,withasurvivalrate ofabout15%,whileout-hospitalarrestshavepositive out-comesof 2---5% in most studies.1,2 Usually, in-hospitalCAs
areprecededbyhypotension,metabolicorelectrolyte
dis-turbances,andrespiratoryinsufficiency,andarepotentially
preventable or modifiable, making a greater survival rate
forin-hospitalCA.3---6
Regarding intraoperative cardiac arrest (ICA), its
inci-dencevariesfrom2.56to44casesper10,000procedures,
witha30-daymortalitythatcanreachupto70%.3,7---11These
differences in incidencemay varygreatly mainly because
thestudiedperiodvariessignificantlyfrom2to10yearsand
thereisalackofadequateepidemiologicalrecording.12The
importanceofthelengthofthestudytimeiscrucial,since
improvementsintechnologiesandinclinicalpracticesmay
haveimpactedthestudyperiod.13 Also,withtheemphasis
onpatientsafetyinanesthesiasincetheearly 1980s,and
withmoreconcentratedeffortstowardpatientsafetysince
the 1990s, a reduction of the incidence of perioperative
mortalitywasobserved.9,13,14
Thepatientrisksandprofilehavealsochangedoverthe
years,asthereisatrendinsubmittingpatientswithgreater
ageandcomorbiditiestosurgery.15---17PatientswithASAIII
orgreaterareresponsiblefor 92---96%of thepatientsthat
presented ICA.18,19 Anesthetic-related and
perioperative-relatedmortalitieshave decreased overthe past50years
consistently,despitetheincreaseinbaselineASAstatusand
patientcomplexity.
Also,thestudiedcountryhasanimpactintheincidence
ofICA.Thegreatestandmostconsistentdeclinewasseenin
developedcountries,ascanbeseenbysomestudiesin
Swe-denandintheUnitedStates.9,13,14,20Indevelopingcountries,
thereisalackofstudiesanalyzingthetrendsinICA.
The authors hypothesized that, as in the rest of the
world,theincidenceofICAisdecreasinginBrazil.Theaim
ofthis study wastosearchthe literatureto evaluatethe
publicationsthatrelate theincidenceofICAin Braziland
comparewiththoseseeninothercountries.
Methods
Inourstudy,ICAwasdefinedasthecardiacarrestpresent
attheoperatingroom.
We reviewed the scientific literature from MEDLINE,
search terms: Intra-operative, perioperative, CA, Brazil,
tertiaryhospitals,anesthesiacomplications,anesthesia
out-comes,cardiopulmonaryresuscitationandanestheticdeath.
Thetermswereusedcombinedandisolated.Articles
repor-tingICAcasesin tertiaryBrazilianhospitalswereincluded
andanalyzed.Also,thereferencesonthefoundtextswere
evaluatedforpossiblerelevantpapers.Datawereanalyzed
descriptively.
Inclusion
criteria
SincethegoalofthisstudywastoevaluatethetrendofICA
inBrazil,onlyBrazilianpaperswereconsideredforanalysis,
includingbothretrospectiveandprospectivestudies.Allof
thestudies were needed tomentionthe ICA incidencein
theoperatingrooms(ORs) ordiagnosticprocedure rooms,
fromallpatientssubmittedtoregionalorgeneral
anesthe-sia.Also,themortalityrates,causes,andoutcomesofCPR
hadtobepresent.
Allarticlesfoundwerereadandclassifiedaccording to
thedurationperiod,numberofpatients,numberand
inci-denceofarrests,mortality,etiologyandoutcomes.
Exclusion
criteria
SincetheaimofthisreviewwastoanalyzeICA,studiesthat
presentonlyanesthesia-relatedandintraoperative-related
mortalitieswerenotincluded.
Results
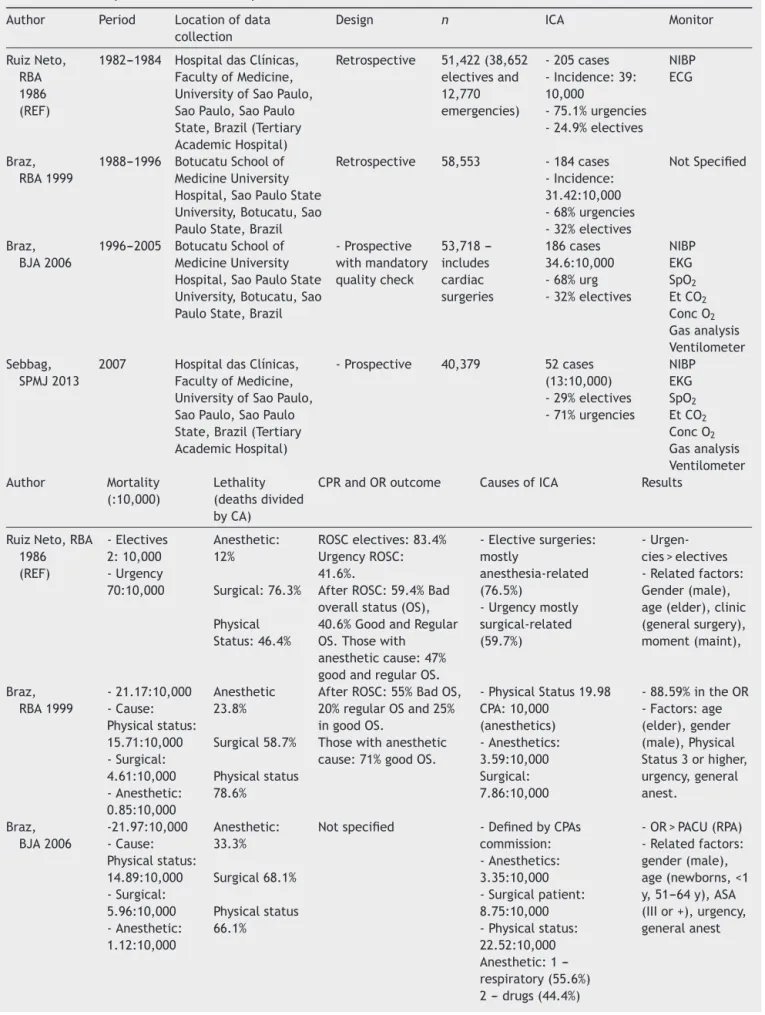
There were only 4 studies that met the inclusion
crite-ria(Table 1). The firststudy wasperformed by Ruiz Neto
etal.,whichanalyzedtheincidenceofICAover theyears
1982---1984, among 51,422 patients undergoing general or
regionalanesthesia.Thesecondandthirdstudieswere
con-ductedbyBrazetal.,whichanalyzedtheincidenceofICA
duringtheyears1988---1996 and1996---2005,reviewingthe
incidenceofICAin58,553and53,718patients,respectively.
The fourth study wasperformed by Sebbaget al.,during
theyear2007,whichincluded40,437patients.21 Together,
these studies analyzed the incidence of 204,072 patients
undergoingregionalorgeneralanesthesiaintwotertiaryand
academichospitals,whichresultedin627casesofICA.The
meanICAincidenceforthe25yearsperiodwas30.72:10,000
anesthesias(Table2).
AspresentedinTable2,theincidenceofICAdecreased
along the years, mainly after 2005. In the period of
1982---1984, the incidence of ICA had its greatest value
forbothoverallandemergencyarrests.During1988---2005,
the overall incidence of ICA decreased when compared
to the study performed by Ruiz-Neto et al., mainly due
to a fall in the emergency incidence of ICA. In 2007, a
great decrease in the incidence of ICA and lethality was
noticed, having an incidence of 13 ICA per 10,000
anes-thetics, withan immediatelethality of 30.8%.21 Although
the two studies performed by Braz et al. included
car-diacsurgery and PACU arrests,the study done by Sebbag
et al. did not. Cardiac surgery ICA and PACU arrests
were responsible, respectively, for 14.8% and 5.4% of
the total arrests during the years 1996---2005; 3.85% and
6.52%intheyears1988---1996.18,21,22Recalculatingthe
inci-dence ofICA,excludingcardiac surgeryandPACUarrests,
therewasanincidenceof 21.9:10,000anesthetics for the
years 1988---1996, 28.1:10,000 anesthetics for the years
1996---2005,and13:10,000in2007,againshowinga
reduc-tionofICAinthelastyears.7,18,21,22
Duringthefirstyearsoftheanalyzedperiod(1982---1984),
76.7% of ICA that occurred during elective surgeries was
related toanesthesiaand thecomorbidities were
respon-sibleforonly5.9%.Inthefollowingyears(1988---2007),ASA
physicalstatusgainedgreatimportance,beingmore
impor-tantthansurgicalor anestheticcausesofICA.Anesthesia,
aftertheyear1984,greatlydecreaseditsimportanceasthe
causeofICA,beinglessimportantthatsurgicalcausesand
ASAstatus.7,18,21,22Theincidenceoftheeventduringallof
theanalyzedperiodswashigherduringgeneralanesthesia
thanwithsubdural,epidural,sacralorregionalanesthesia.
ThemeanageofICAshowedanincreaseduringtheperiod
of1982---2007.Theagegroupthathadthegreatestincidence
ofICAintheyears1982---1984wasbetween20and49years
(27.4%),whileinthefollowingyears,theagegroupsgreater
than40yearshadthegreatestincidenceofICA.
The main causesof ICA alsovariedalong the analyzed
years. Duringthe years1982---1984, the main factors that
led to ICA were related to the surgery. Those related to
anesthesia were mainly anesthetic overdose, hypoxemia,
cardiocirculatory collapse after regional anesthesia, and
anesthesia machinemalfunction. In the years1988---1996,
hypoxia and hypoventilation were the leading cause of
anesthesia-relatedICA.Thesecausesresultedmainlyfrom
vomitaspiration,thoughnodifficultairwaywasmentioned.
Thesecond maincauseofICAduringthissameperiodwas
cardiocirculatorycollapseafterregionalanesthesia.22Inthe
years 1996---2005, the leading causeof anesthesia-related
ICA was also hypoventilation, but mainly due to difficult
airway.Hypoventilationwasfollowedbymedication-related
problems,whichincludedanestheticoverdosageandfluid
overload.Duringtheyear2007,themostcommoncauseof
thestudiedadverseeventswashypovolemia(42%),followed
byrespiratory(21%)andmetabolic(21%)disturbancesand
theICAmainlyoccurredduringthemaintenanceperiodof
generalorcombinedanesthesia.18,21,22
WhenanalyzingthelethalityoftheCA(calculated
divid-ing the number of deaths by the total CAs), in the years
1982---1984,itwas12%foranesthesia,76.3%forsurgeryand
46.4%forcomorbidities.InthestudyofBrazetal.duringthe
periodof1988---1996,theanestheticlethalityofICAwas24%
withanoveralllethalityof67.3%.Intheyears1996---2005,
theanesthesia-relatedlethalitykeptonraisingto33%,with
anoveralllethalityof63.4%.ThestudyperformedbySebbag
etal.doesnotprovideenoughdatatocalculate
anesthesia-relatedlethality,but 40%ofthe ICAwasat leastpartially
attributabletoanesthesia.Theoverallimmediatelethality
was30.8%,whichis apronouncedreductionfromthelast
studiedperiod(1996---2005).18,21,22
Theproportionofanesthesia-relatedCAtothetotal
num-ber of anesthesia also presented with changes along the
studiedperiod.Intheyears1982---1984,thisproportionwas
14.39:10,000 (7), while from 1988 to1996, it reduced to
0.85:10,000.Afterthisnadir,theproportionof
anesthesia-relatedCAtothetotalnumberofanesthesiakeptonraising
Table1 Summaryofthestudiesandrespectiveresults.
Author Period Locationofdata collection
Design n ICA Monitor
RuizNeto, RBA 1986 (REF)
1982---1984 HospitaldasClínicas, FacultyofMedicine, UniversityofSaoPaulo, SaoPaulo,SaoPaulo State,Brazil(Tertiary AcademicHospital)
Retrospective 51,422(38,652 electivesand 12,770 emergencies)
-205cases -Incidence:39: 10,000
-75.1%urgencies -24.9%electives
NIBP ECG
Braz, RBA1999
1988---1996 BotucatuSchoolof MedicineUniversity Hospital,SaoPauloState University,Botucatu,Sao PauloState,Brazil
Retrospective 58,553 -184cases -Incidence: 31.42:10,000 -68%urgencies -32%electives
NotSpecified
Braz, BJA2006
1996---2005 BotucatuSchoolof MedicineUniversity Hospital,SaoPauloState University,Botucatu,Sao PauloState,Brazil
-Prospective withmandatory qualitycheck 53,718 ---includes cardiac surgeries 186cases 34.6:10,000 -68%urg -32%electives
NIBP EKG SpO2 EtCO2 ConcO2 Gasanalysis Ventilometer Sebbag,
SPMJ2013
2007 HospitaldasClínicas, FacultyofMedicine, UniversityofSaoPaulo, SaoPaulo,SaoPaulo State,Brazil(Tertiary AcademicHospital)
-Prospective 40,379 52cases (13:10,000) -29%electives -71%urgencies
NIBP EKG SpO2 EtCO2 ConcO2 Gasanalysis Ventilometer Author Mortality (:10,000) Lethality (deathsdivided byCA)
CPRandORoutcome CausesofICA Results
RuizNeto,RBA 1986 (REF) -Electives 2:10,000 -Urgency 70:10,000 Anesthetic: 12% Surgical:76.3% Physical Status:46.4%
ROSCelectives:83.4% UrgencyROSC: 41.6%.
AfterROSC:59.4%Bad overallstatus(OS), 40.6%GoodandRegular OS.Thosewith anestheticcause:47% goodandregularOS.
-Electivesurgeries: mostly
anesthesia-related (76.5%)
-Urgencymostly surgical-related (59.7%)
- Urgen-cies>electives -Relatedfactors: Gender(male), age(elder),clinic (generalsurgery), moment(maint), Braz, RBA1999 -21.17:10,000 -Cause: Physicalstatus: 15.71:10,000 -Surgical: 4.61:10,000 -Anesthetic: 0.85:10,000 Anesthetic 23.8% Surgical58.7% Physicalstatus 78.6%
AfterROSC:55%BadOS, 20%regularOSand25% ingoodOS.
Thosewithanesthetic cause:71%goodOS.
-PhysicalStatus19.98 CPA:10,000 (anesthetics) -Anesthetics: 3.59:10,000 Surgical: 7.86:10,000
-88.59%intheOR -Factors:age (elder),gender (male),Physical Status3orhigher, urgency,general anest. Braz, BJA2006 -21.97:10,000 -Cause: Physicalstatus: 14.89:10,000 -Surgical: 5.96:10,000 -Anesthetic: 1.12:10,000 Anesthetic: 33.3% Surgical68.1% Physicalstatus 66.1%
Notspecified -DefinedbyCPAs commission: -Anesthetics: 3.35:10,000 -Surgicalpatient: 8.75:10,000 -Physicalstatus: 22.52:10,000 Anesthetic:1 ---respiratory(55.6%) 2---drugs(44.4%)
Table1(Continued)
Author Mortality (:10,000)
Lethality (deathsdivided byCA)
CPRandORoutcome CausesofICA Results
Sebbag, SPMJ2013
Upto30days ---10:10,000
-Overall immediate lethality: 30.8% -30-days lethalitywas 75%
-69%successfulCPRs Survivors:
-39%in24h -25%in30d -elect53% -emerg14%
-Definedretrospectively -Physicalstatus(52%) -Surgical(8%) -Anesthetic(40%)
-Relatedfactors: gender(male) -Physicalstatus (ASAIIIor+) -Emergency(71%) -Generalanest (90%)
ECG,continuouselectrocardiogram;NIBP,non-invasivebloodpressure;SpO2,pulseoximeter;OS,overallstatus;OR,operatingroom;
CPA,cardio-pulmonaryarrest;ROSC,returnofspontaneouscirculation;PACU,post-anesthesiacareunit.
1996---2005 and 5:10,000 in 2007).18 Although the number
ofICAandtheoverall lethalitygreatly decreasedin2007,
theproportionofanesthesia-relatedCAtothetotalnumber
ofanesthesiaincreased.18,21,22
Discussion
Alongthe25yearsanalyzedbythisreview,theincidenceof
ICApresentedwithchanges.Therewasobservedadecrease
inICAinBrazil,especiallyinthelastdecade.
In the 1980s, other studies around the world showed
that ICA ranged from 1 to 23 arrests/10,000 anesthesias
while,inBrazil,intheyears1982---1984,theincidenceofICA
washigherthan the worldwideincidence, with39:10,000
anesthesias.7,9,10,13,23,24Thisworldwideincidencewasfound
instudiesperformedindevelopedcountries,whichincluded
France,UnitedStatesofAmerica,SwedenandNetherlands.
TheFrenchstudy,whichpresentedwiththehighestICA
inci-dence amongthe developed countries,reported that the
mainanesthesia-relatedcausehadanimportantrelationship
withmedicationuse,whichwasinagreementwiththemain
causefoundinBrazil,whichwasanestheticoverdose.7Inthe
USA,whichhadthelowestincidenceofICA,enhanced
intra-operative monitoring, the introduction of pulse oximetry
andcapnometry,theroutineuseofdisconnectalarms,and
ageneralawarenessof thereportedmishapwerepointed
asimportantstepstoreducetheoverall incidenceof ICA,
resultinginthelowestincidenceofthereportedstudies.13
Atthisperiod,pulseoximetry,monitoredend-tidalCO2,and
defibrillators were not obligated by any legislation tobe
present inside the operating room in Brazil, which could
have had a negativeimpact in the ICA,since it can help
detect situations that can lead to CA, such as ventilator
failuresanddisconnection.Anesthesiamachinefailurewas
listed among the top causes of ICA in Brazil and wasnot
citedasanexpressivecauseofICAbyotherarticlesduring
thisdecade.24SincethestudydonebyRuiz-Netoetal.does
notprovide furtherdetails onthetypeofmachinefailure
noritspecifiestheanesthesiamachineused,wecan
specu-latethattheincorporationofcapnographsoralarmscould
have reducedthe incidenceof ICAasexpectedbyKeenan
andBoyan,butsincemachinefailureisavastterm,we
can-notaffirm thisstatement.13 Also,thedescriptivestudy of
RuizNetoetal.wasperformedinatertiaryteaching
hospi-tal,inwhichpatientshavemorecomorbidities,withagreat
numberofurgentandemergencysurgeries,inpatientsASA
PIVandV,whichcouldhaveanimportantroleinincreasing
theICAduringthisperiod.7
In the following decade, ASA physical status was the
mainfactorrelatedtoICA,followedbyhypoxemiabecause
of vomit aspiration. During this period, anesthetic
over-dose was notlisted asoneof the most important factors
thatcouldleadICA.The mostnoticeablechangewasthat
anesthesiawasnolongerthemainfactorrelatedtoICAin
electivesurgeries.Also,therewasanoticeablereductionin
the number ofICA relatedto anesthesiaand surgery, but
an increase in those related to the patient physical
sta-tus, especially thosepatients categorized asASA PIII, IV
and V. The number of CA related to anesthesia over all
of the anesthetic procedures performed and
anesthesia-relatedmortalitysuffered agreatdecrease.Part ofthese
results may be related to the introduction of a
Brazil-ian legislation in 1993, which included as mandatory the
monitoringofbloodpressure,theuseofprecordial
stetho-scope,andthepresenceofdefibrillatorsandrescuedrugsin
Table2 Incidenceofcardiacarrest(elective,emergencyandoverall),overalllethalityalongtheyears.Valuesofincidenceof cardiacarrestandmortalityarepresentedper10,000anesthetics.Lethalityispresentedinpercentages.
Years Overallincidence ofcardiacarrest (:10,000)
Incidenceofcardiacarrest inemergencycases (:10,000)
Incidenceofcardiac arrestinelectivecases (:10,000)
Overall lethality
1982---1984 39.0 120.0 13.0 48.3%
1988---1996 31.4 45.4 19.2 67.3%
1996---2005 34.6 55.4 19.4 63.4%
theoperatingtheater(FederalMedicineCouncilResolution Number 1363/93).25 The monitoring of end tidal CO
2 was
stillreservedforcertainproceduresandpulseoximetrywas
mandatoryonlyinhospitalsthatusedoxygenconcentration
plants.Althoughthislegislationincreasedpatientsafetyand
couldtheoreticallyreducetheincidenceandthelethalityof
ICA,an increase inoverall- and anesthetic-related
lethal-ities and a decrease in the incidence of ICA were found
during these years. The incorporation of these
technolo-gies might have an impact in preventable and promptly
reversible causes of ICA, such as hypoxia that could be
prevented by the use of oxymeters or by disconnection
alarms. But, some causes of ICA (i.e. cardiac infarction)
could not be prevented by the presence of monitors or
alarms. Usually, theses causes have more difficult return
to the spontaneous circulation, which could explain why
thelethalityincreasedalong theanalysedyears:less
pre-ventablecausesofICA.Also,duringthisdecade,asreported
by other studies, a noticeable increase in the number of
high-risksurgicalelderlypatientswasreported,whichmight
explaintheincreaseinthelethality.9,26,27
In 2007, a great decreasein the incidence of ICA and
lethality was noticed, having an incidence of 13 ICA per
10,000anesthetics, withan immediatelethalityof 30.8%.
AlthoughfewstudieshaveanalyzedtheICAincidencefrom
2005 up to now, this incidence lies in the middle of the
worldwideaverageforthisperiod,whichvariedfrom7to
44CAsper10,000anesthetics.11,28Thedecreaseinthe
inci-denceofICAmaybepartiallyexplainedbyanewlegislation
directed to anesthesia approved in the year 2006
(Fed-eralCouncil ofMedicine Resolution n◦ 1.802/2006).29 This
legislation required thatall patientshad a pre-anesthetic
consultbeforehospitaladmissionandestablishedthe
mini-mumworkingconditionstoperformanesthesia,whichmust
include, at least, non-invasive blood pressure
measure-ments, continuous ECG, pulse oximetry and capnography
forallpatients.Also,thisnewlegislationincludedminimum
monitorsforpost-anesthesiacareunit,whichincluded
non-invasivebloodpressureandpulseoximetry.Thislegislation
wasasteptowardanincreaseinpatientsafety,whichhas
beenaworldfocussinceearly1980sandwithmoreefforts
inthe1990s.Thisfocushasbeenparticularlyadoptedbyall
countries,butmainlyinhighhumandevelopmentindexed
countries.20
OnefacttoconsiderwhenanalyzingICAinBrazilisthatit
isadevelopingcountry,whichhasauniversalhealthsystem.
Thecountry’shumandevelopmentindex(HDI)isrelatedto
the rate of improvement in perioperative mortality
over-time,andthismightbearesultoftheabilityofwealthier
countries toincrease health-careinvestment in
technolo-gies,techniques,andtrainingnecessarytoimprovepatient
safety.20 As seen by anotherreview, thereis a worldwide
trendtoreducetheincidenceofICA,especiallyindeveloped
countries.20 Brazil isnoexception tothisrule,decreasing
from 39 ICA per 10,000 anesthetics to13 ICA per 10,000
anesthetics along these 25 years studied. Although Brazil
had, during the 1980s---1990s, a mean HDI of 0.56, which
wasclosetotheworldaverage(0.58)andfarfromveryhigh
(0.82)HDIcountries,itsincidenceofICAwasclosertothose
countrieswithlowHDI,beingmorethan30CAsper10,000
anesthetics.20 After the year 2000, especiallyin the year
2007,BrazilhadanincreaseintheHDI(0.71)andsatcloser
tohighHDI(0.74)countries,butitsincidenceofICAwasstill
farfromhighHDIcountries.20,30Thismightbeindicativeof
arelationshipbetweencountries’HDIandtheincidenceof
ICA,evensuggestingthattheincidenceofICAmightreflect
thecountry’shealthcaresystem.Thisisalsosupportedby
thefactthat,in2011,only4.1%ofthegrossnationalproduct
ofBrazilwasspentinthehealthsystem,whichislessthan
halfofwhattheUSAspentforpublichealth.30 Onefactto
consideristhatBrazilhasauniversalhealthsystem,while
USAdoesnot.
Althoughtherewerealmost 204,072patientsanalyzed,
which resulted in 627 cases of ICA, with an incidence
of 30.72:10,000 anesthesia during the 25 years period,
this review showed a decrease in ICA from 39:10,000 to
13:10,000.Allofthefourstudieswereperformedintertiary
teachinghospitals, whichmight have resulted in ahigher
incidenceofICA.Also,thesehospitalswerelocatedinthe
wealthierpartofBrazil,inonespecificstateofthecountry,
whichalsoisalimitationofthisreview.
Summary
TherewasareductionintheincidenceofICAinthelast25
yearsinBrazil.Thisreductionisseenworldwideandmight
bearesultofmultiplefactors,includingnewlawsregulating
themedicineinBrazil,incorporationoftechnologies,better
humandevelopmentlevelofthecountry,andbetterpatient
care.
Funding
Institutionalfunding.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.Girardi LN, BariePS. Improved survival after intraoperative cardiac arrest in noncardiac surgical patients. Arch Surg. 1995;130:15---8,discussion19.
2.Schneider2ndAP,NelsonDJ,BrownDD.In-hospital cardiopul-monaryresuscitation:a30-yearreview.JAmBoardFamPract. 1993;6:91---101.
3.Kazaure HS, Roman SA, Rosenthal RA, et al. Cardiac arrest among surgical patients: an analysis of incidence, patient characteristics, and outcomes in ACS-NSQIP. JAMA Surg. 2013;148:14---21.
4.Bedell SE, Deitz DC, Leeman D, et al. Incidence and char-acteristics of preventable iatrogenic cardiac arrests. JAMA. 1991;265:2815---20.
5.Ebell MH, Afonso AM. Pre-arrest predictors of failure to surviveafterin-hospitalcardiopulmonaryresuscitation:a meta-analysis.FamPract.2011;28:505---15.
6.MartinezJP.Prognosisincardiacarrest.EmergMedClinNAm. 2012;30:91---103.
8.Kawashima Y, Takahashi S, Suzuki M, et al. Anesthesia-related mortality and morbidity over a 5-year period in 2,363,038patientsinJapan.ActaAnaesthesiolScand.2003;47: 809---17.
9.Olsson GL, Hallen B. Cardiac arrest during anaesthesia. A computer-aidedstudyin250,543anaesthetics.Acta Anaesthe-siolScand.1988;32:653---64.
10.Chopra V, Bovill JG, Spierdijk J. Accidents, near accidents and complicationsduringanaesthesia.A retrospective analy-sis of a 10-year period in a teaching hospital. Anaesthesia. 1990;45:3---6.
11.Boonmak P, Boonmak S, Sathitkarnmanee T, et al. Surveil-lance of anesthetic related complications at Srinagarind Hospital, Khon Kaen University,Thailand.J MedAssoc Thai. 2005;88:613---22.
12.Goswami S, Brady JE, Jordan DA, et al. Intraoperative cardiacarrestsinadultsundergoingnoncardiacsurgery: inci-dence, risk factors, and survival outcome. Anesthesiology. 2012;117:1018---26.
13.KeenanRL,BoyanCP.Decreasingfrequencyofanesthetic car-diacarrests.JClinAnesth.1991;3:354---7.
14.SprungJ,Warner ME,ContrerasMG,etal.Predictorsof sur-vivalfollowingcardiacarrestinpatientsundergoingnoncardiac surgery:astudyof518,294patientsatatertiaryreferralcenter. Anesthesiology.2003;99:259---69.
15.RoquesF,NashefSA,MichelP,etal.Riskfactorsandoutcome inEuropeancardiacsurgery:analysisoftheEuroSCORE multi-nationaldatabaseof19030patients.EurJCardiothoracSurg. 1999;15:816---22,discussion822---3.
16.Ferguson Jr TB, Hammill BG, Peterson ED, et al. A decade of change-risk profiles and outcomes for isolated coronary arterybypassgrafting procedures,1990---1999:areportfrom theSTS National DatabaseCommittee and the DukeClinical ResearchInstitute.SocietyofThoracic Surgeons.AnnThorac Surg.2002;73:480---9,discussion489---90.
17.AlexanderKP,AnstromKJ,MuhlbaierLH,etal.Outcomesof car-diacsurgeryinpatients>or=80years:resultsfromtheNational CardiovascularNetwork.JAmCollCardiol.2000;35:731---8.
18.BrazLG,ModoloNS,doNascimentoJr P,etal.Perioperative cardiacarrest:astudyof53,718anaestheticsover9yrfroma Brazilianteachinghospital.BrJAnaesth.2006;96:569---75.
19.Newland MC, Ellis SJ, Lydiatt CA, et al. Anesthetic-related cardiac arrest and its mortality: a report covering 72,959 anestheticsover10years fromaUS teachinghospital. Anes-thesiology.2002;97:108---15.
20.Bainbridge D, Martin J, Arango M, et al. Perioperative and anaesthetic-related mortality in developed and developing countries: a systematic review and meta-analysis. Lancet. 2012;380:1075---81.
21.SebbagI,Carmona MJC,GonzalezMMC, et al. Frequency of intraoperativecardiac arrestand medium-termsurvival. Sao PauloMedJ.2013;131:309---14.
22.BrazJR,SilvaACM,CarlosE,etal.Cardiacarrestduring anes-thesiaatatertiaryteachinghospital(1988to1996).RevBras Anestesiol.1999;49:257---62.
23.PottecherT,TiretL,DesmontsJM,etal.Cardiacarrestrelated toanaesthesia:aprospectivesurveyinFrance(1978---1982).Eur JAnaesthesiol.1984;1:305---18.
24.OtteniJC,PottecherT,TiretL,etal.Arretcardiaquependant l’anesthesie et la periode de reveil. Donnees de l’enquete INSERM1978-1982[Cardiac arrestduring anesthesia and the recoveryperiod.DatafromtheINSERMsurvey1978---1982].Ann FrAnesthRéanim.1986;5:287---94.
25.Brazilian Federal Council of Medicine Resolution 1.363/93; 1993.
26.KlopfensteinCE,HerrmannFR,MichelJP,etal.Theinfluence ofanagingsurgicalpopulationontheanesthesiaworkload:a ten-yearsurvey.AnesthAnalg.1998;86:1165---70.
27.TiretL,DesmontsJM,HattonF,etal.Complicationsassociated withanaesthesia---aprospectivesurveyinFrance.CanAnaesth SocJ.1986;33:336---44.
28.ZuercherM,UmmenhoferW.Cardiacarrestduringanesthesia. CurrOpinCritCare.2008;14:269---74.
29.BrazilianFederalCouncilofMedicineResolution;2006. 30.WorldBank[databaseontheInternet]WorldDevelopment