448 LETTERSTOTHEEDITOR
Opening
snap
off
ampoules
---
a
safer
and
uncomplicated
method
Abertura
de
ampolas
de
vidro
---
Um
método
mais
simples
e
seguro
DearEditor,
Anaesthetic drugs are often available in glass ampoules whichneedtobe‘snappedopen’alongthecolouredbands or dot around the neck. Different manoeuvres can be employed for opening these ampoules like snapping with thumbandindexfinger(withorwithoutusinggauzepieces), scratchingtheneckofthevialwithfileorbaseofanother vial and snapping open,1 using scissors2 or knife. If done
properly, the neck of the ampoules snap open cleanly without producing spikes or glass shards. However, quite oftenseriouscutscanoccuronthefingers,ensuing lacer-ations necessitating suturing, infection susceptibility, loss of work days,rehabilitation, andresidual pain.3 Ampoule
opening is classified as a high risk event4 with broken
ampoulescausing 54% of the reportedincidentsin anaes-thesia personnel.5 Ampoule cuts are known to occur in
6%anaestheticsessions.6Eventhoughspecializedampoule
opening devicesexist, they maynot be always available, whichcanprovedangerousduringemergencies.Wedescribe asimple,inexpensiveandsafemethodofopeningampoules, usingthebarrelofasyringewhichisbeingroutinely prac-ticedin our institution thereby preventingpossible sharp injuries.
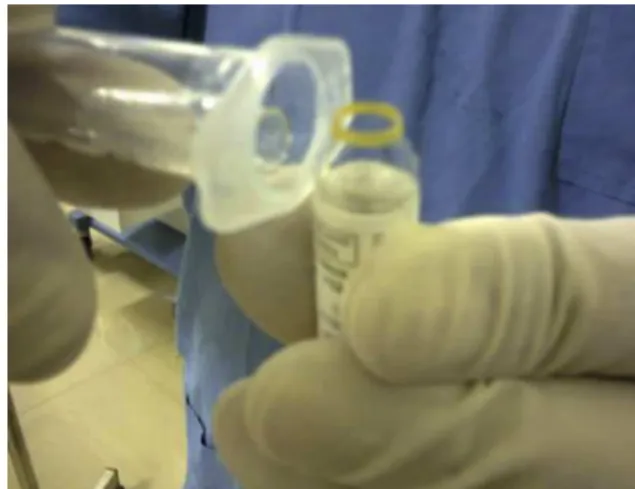
The barrel of a syringe (plunger removed from the syringe)is taken in the dominant hand and inverted and withthenon-dominanthand.Theconicaltipoftheampoule is inserted inside the hollow cylindrical space inside the barrel (Fig. 1). The depth of insertion of the ampoule insidethe hollowissoadjusted that theconstrictedneck of the ampoule having the coloured marking is in close proximity to the lower circumferential edge of the bar-rel’shollow.Holding thebase oftheampoulesteady with the non-dominant hand, a steady pull is appliedtowards the clinicianwhile the barrel is pushed away with domi-nanthand(withtheconicalheadinsideit)withcontinuous andeven pressure, keepingthe edge in contact withthe
Figure1 Insertingtheconicaltipoftheampouleinsidethe hollowcylindricalspaceofthebarrel
Figure2 Thesharpbroken conical tipoftheampouleand theglassshardsremaininginsidethehollowbarrelafteraclean breakforwhichcantappingoutanddiscardingwithoutbringing themincontactwiththefingers
neck. Alight pressureappliedcorrectly willcleanlycrack theampouleopenalong thecolouredline. Thesharp bro-kenconicaltipoftheampouleandtheglassshardsremain insidethe hollowbarrel whichcanbetappedoutand dis-carded safely without bringing them in contact with the fingers(Fig.2).
Advantageofthistechniqueincludeslowcost,easy avail-ability of syringes in the hospital, utilization of a single barrel for multiple ampoules andkeeping fingers clear of glassshardsandslivers.However,limitationofthismethodis thatonlythoseampouleswhichhavevolumeslessthan5mL withetchedringsontheneckcanbeopenedeasily.Itisnot feasibletoopenlargerampoules(greaterthan5mLvolume) withthismethod.Forbiggerampoules,alargersyringe(of 10mL)canbepossiblyused.Aslightlyhigherdegreeof pres-suremayberequiredfor snappingofftheampoulebythis methodascomparedtomanualsnappingoftheneckwith fingerswhichmorethancompensatesfortheadvantageof avertingsharpinjuries.
References
1.CohenY,GlantzL,EzriT.Breakingglassvials.Anaesthesiology. 1997;86:1215.
2.KogaK,HiroseM.Scissorsasapropofolampoule‘snapper’? Anaes-thesia.1999;54:919---20.
3.BajwaSJ, Kaur J. Risk and safetyconcerns inanesthesiology practice: thepresent perspective.Anesth Essays Res. 2012;6: 14---20.
4.SmithDR,LeggatPA.Needlestickandsharpsinjuriesamong nurs-ingstudents.JAdvNurs.2005;51:449---55.
5.Pulnitiporn A, Chau-in W, Klanarong S, et al. The Thai Anesthesia. Incidents Study (THAI Study) of anes-thesia personnel hazard. J Med Assoc Thai. 2005;88: S141---4.
LETTERSTOTHEEDITOR 449 RudrashishHaldar∗,SukhminderJitSinghBajwa,
JasleenKaur
DepartmentofAnaesthesia,GianSagarMedicalCollege andHospital,Banur,India
∗Correspondingauthor.
E-mail:[email protected](R.Haldar). Availableonline12March2014
http://dx.doi.org/10.1016/j.bjane.2014.02.006
Importance
of
maternal
body
temperature
recording
after
injection
of
meperidine
during
spinal
anesthesia
in
patients
undergoing
cesarean
section:
an
offering
for
conducting
clinical
studies
A
importância
do
controle
da
temperatura
corporal
materna
após
injec
¸ão
de
meperidina
durante
a
raquianestesia
em
pacientes
submetidas
à
cesariana:
uma
sugestão
para
conduzir
estudos
clínicos
DearEditor,
Shiveringrelated tospinal and epidural anesthesiais dis-tressingtoparturientwomenasitmaycausecardiovascular and metabolic disturbances. Shivering increases cardiac outputandcausestachycardia; also,hypothermia-induced shiveringincreasestotalbodyoxygenconsumptionandcould cause hypoxemia. These effects may place mothers and thefetuses at thegreatest risk duringdelivery.1 The rate
of shiveringvaried from36% to55% in different studies.2
Meperidineisa(Kappa)-receptoragonistandopioid(Mu)
receptorthatreducesthethresholdofvascularconstriction andisknowntotreatshiveringeffectively.3Hereweprovide
commentsonthreepointsontheimportanceofbody tem-peraturerecordingafterinjectionofmeperidine,basedon clinical research conductedon patients undergoingspinal anesthesiaforcesareansection.
First, intra-operative shivering is a particular feature ofthermoregulationinawakepatientsundergoingregional anesthesia(inresponsetosympatholysis,vasodilatationand increasedheat loss). Intra-operativeshivering is inhibited during general anesthesia; accordingly patients are more pronetohypothermiaandpost-operativeshivering.Hence, therearetwoimportant elements toregional anesthesia-inducedshivering:(1)thedesiredeffectofshivering,i.e., heat preservation by increased basal metabolic rate and (2) the unwanted effects of shivering (increased venous O2,desaturation,myocardialO2extraction,discomfortand
anxiety for patient, and possibly movement for surgeon andmonitoringartifactsfortheanesthesiologist(e.g., sys-tolicpO2,noninvasive bloodpressureand ECGartifactsin
intra-operativeshivering).4,5Therefore,theauthorsshould
measurematernalbodytemperature toassessthedesired effects.
Second,whenevervolumepre-loadingwith10mL/kgor 15mL/kgofroomtemperaturecrystalloidisemployed,the
maternal hypothermia could reasonably be expected to altershivering prevalence. Therefore, maternal tempera-turerecordingisveryimportant.
Third,ifmeperidinesuppressesshivering,itmayleadto lowerbodytemperaturefollowing regionalanesthesiaand thismayleadtomorehypothermiaandalsotomore shiv-eringlateron.Accordingly,appropriatebodytemperature recordingafterinjectionofmeperidineduringspinal anes-thesia in patients undergoing cesarean section should be consideredby authorsinfuturestudies formore accurate andreliablefindings.
References
1.KhawKS,KeeWDN,LeeSWY.Hypotensionduringspinal anaes-thesiaforcaesareansection:implications,detectionprevention andtreatment.FetalMaterMedRev.2006;17:69.
2.BhukalI,SolankiSL,KumarS,etal.Pre-inductionlowdose pethi-dinedoesnotdecreaseincidenceofpostoperativeshiveringin laparoscopicgynecologicalsurgeries.JAnaesthesiolClin Pharma-col.2011;27:349.
3.Delaunay L, Bonnet F, Liu N, et al. Clonidine comparably decreasesthethermoregulatorythresholdsforvasoconstriction andshiveringinhumans.Anesthesiology.1993;79:470---4.
4.ChunDH,KilHK,KimHJ,etal.Intrathecalmeperidinereduces intraoperativeshivering duringtransurethral prostatectomyin elderlypatients.KoreanJAnesthesiol.2010;59:389---93.
5.KhanZH,ZanjaniAP,MakaremJ,etal.Antishiveringeffectsof twodifferentdosesofintrathecalmeperidineincaesarean sec-tion:aprospectiverandomisedblindedstudy.EurJAnaesthesiol. 2011;28:202---6.
MohamedAminGhobadifara,∗,HassanZabetianb,
MohammadYasinKaramic,ZahraMosallanezhadd,
NavidKalanib
aDepartmentofStudentResearchCommittee,Jahrom
UniversityofMedicalSciences,Jahrom,Iran
bDepartmentofAnesthesiology,JahromUniversityof
MedicalSciences,Jahrom,Iran
cDepartmentofGeneralSurgery,MazandaranUniversity
ofMedicalSciences,Mazandaran,Iran
dDepartmentofObstetricsandGynecology,Shiraz
UniversityofMedicalSciences,Shiraz,Iran
∗Correspondingauthor.
E-mails:[email protected],[email protected]
(M.A.Ghobadifar).
Availableonline12March2014