REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
OfficialPublicationoftheBrazilianSocietyofAnesthesiologywww.sba.com.br
SCIENTIFIC
ARTICLE
Comparison
of
the
effects
of
magnesium
sulphate
and
dexmedetomidine
on
surgical
vision
quality
in
endoscopic
sinus
surgery:
randomized
clinical
study
Akcan
Akkaya
a,∗,
Umit
Yasar
Tekelioglu
a,
Abdullah
Demirhan
a,
Murat
Bilgi
a,
Isa
Yildiz
a,
Tayfun
Apuhan
b,
Hasan
Kocoglu
aaDepartmentofAnesthesiologyandReanimation,AbantIzzetBaysalUniversityMedicalSchool,Bolu,Turkey bDepartmentofHead&NeckSurgery,AbantIzzetBaysalUniversityMedicalSchool,Bolu,Turkey
Received23November2013;accepted15January2014 Availableonline21February2014
KEYWORDS
Endoscopicsinus surgery; Magnesium; Dexmedetomidine; Hypotension
Abstract
Backgroundandobjectives: Evenasmallamountofbleedingduringendoscopicsinussurgery cancorrupttheendoscopicfieldandcomplicatetheprocedure.Varioustechniques,including inducedhypotension,canminimizebleedingduringendoscopicsinussurgery.Theaimofthis study was tocompare thesurgicalvision quality, haemodynamic parameters,postoperative pain,andothereffectsofmagnesium, ahypotensiveagent,withthatofdexmedetomidine, whichwasinitiallydevelopedforshort-termsedationintheintensivecareunitbutalsoisan alpha2agonistsedative.
Method: 60patientsbetweentheagesof18and45yearsweredividedintoeitherthe mag-nesiumgroup (GroupM)orthe dexmedetomidinegroup (GroupD). In GroupM,magnesium sulphatewasgivenatapre-inductionloadingdoseof50mgkg−1over10minandmaintained
at15mgkg−1h−1;inGroupD,dexmedetomidinewasgivenat1mcgkg−110minbefore
induc-tionandmaintainedat0.6mcgkg−1h−1.Intraoperatively,thehaemodynamicandrespiratory
parametersand6-pointintraoperative surgicalfieldevaluationscalewererecorded.During thepostoperative period,an11-pointnumericalpain scale,theRamsaysedationscale, the nausea/vomitingscale,theadverseeffectsprofile,anditchingparameterswerenoted.
Results:GroupDshowedasignificantdecreaseinintraoperativesurgicalfieldevaluationscale scalescoreandheartrate.Theaverageoperationtimewas50min,andGroupMhadahigher numberofprolongedsurgeries.Nosignificantdifferencewasfoundintheotherparameters.
Conclusions:Duetoitsreductionofbleedingandheartrateinendoscopicsinussurgeryand itspositive impactsonthedurationofsurgery,weconsiderdexmedetomidine tobeagood alternativetomagnesium.
©2014SociedadeBrasileiradeAnestesiologia.PublishedbyElsevier EditoraLtda.Allrights reserved.
∗Correspondingauthor.
E-mails:[email protected],[email protected](A.Akkaya).
0104-0014/$–seefrontmatter©2014SociedadeBrasileiradeAnestesiologia.PublishedbyElsevierEditoraLtda.Allrightsreserved.
PALAVRAS-CHAVE
Cirurgiaendoscópica sinusal;
SulfatodeMagnésio; Dexmedetomidina; Hipotensão
Comparac¸ãodosefeitosdesulfatodemagnésioedadexmedetomidinasobrea qualidadedavisibilidadeemcirurgiaendoscópicasinusal:estudoclínicorandomizado
Resumo
Justificativaeobjetivo: Umaquantidade,mesmopequena,desangramentoduranteacirurgia endoscópicapodealterarocampoendoscópicoedificultaroprocedimento.Váriastécnicas, incluindohipotensãoinduzida,podemminimizarosangramentoduranteacirurgiaendoscópica. O objetivo deste estudo foi comparar a qualidade da visibilidade cirúrgica, os parâmetros hemodinâmicos,adornoperíodopós-operatórioeoutrosefeitosdosulfatodemagnésio,um agentehipotensor,comosdadexmedetomidina,inicialmentedesenvolvida parasedac¸ãoem curtoprazoemunidadedeterapiaintensiva,masquetambéméumsedativoagonistaalfa-2.
Métodos: Foramalocados60pacientesentre18e45anosemdoisgrupos:GrupoM(magnésio) eGrupoD(dexmedetomidina).NoGrupoM,sulfatodemagnésiofoiadministradopré-induc¸ão auma dosedecargade50mgkg−1 por10minutos emantidacom15mgkg−1h−1;noGrupo
D,dexmedetomidinafoiadministradaaumadosede1mcgkg−110minutosantesdainduc¸ão
emantidacom0,6mcgkg−1h−1.Noperíodointraoperatório,foramregistradososparâmetros
hemodinâmicoserespiratórioseaavaliac¸ãodocampocirúrgicocomumaescaladeseispontos. Duranteoperíodopós-operatórioforamregistradososvaloresdaescalanuméricade11pontos paraavaliarador,aescaladesedac¸ãodeRamsay,aescaladeavaliac¸ãodenáusea/vômito,o perfildosefeitosadversosepruridos.
Resultados: OGrupoD apresentoureduc¸ãosignificativadafrequênciacardíaca edoescore naescala de avaliac¸ão docampo cirúrgicointraoperatório.A média dotempo cirúrgicofoi de50minutoseoGrupoMapresentouumnúmeromaiordecirurgiasprolongadas.Nãohouve diferenc¸asignificativaemoutrosparâmetros.
Conclusão:Porcausadareduc¸ãodataxadesangramentoedafrequênciacardíacaemcirurgia endoscópicaedosimpactospositivossobreadurac¸ãodacirurgia,consideramos dexmedeto-midinacomomelhoropc¸ãoqueosulfatodemagnésio.
©2014SociedadeBrasileira deAnestesiologia.PublicadoporElsevierEditoraLtda.Todosos direitosreservados.
Introduction
Endoscopicsinussurgery(ESS)isaformofsurgical interven-tioninwhichsurgicalvisualizationmaydiminishcompletely withonlyasmallamountofbleeding.1Thissurgeryisdone
under endoscopic magnification in a narrow area where manipulationisdifficult.
Therefore,hypotensivebleedingcontrolduringthe oper-ationmayhelptoincreasesurgicalvisualization.Different anaesthetic techniques and drugs arebeing explored and tested tohelp tosolve thisproblem.2-4 Magnesium is one
drug used for this purpose, and its positive effects on the control of postoperative bleeding have been clearly defined.5,6 Magnesium is an
N-methyl-d-aspartate (NMDA)
receptorantagonistthatreducestheneedforanalgesicand sedative drugs. Dexmedetomidine is also an alpha 2 ago-nist;it hassedative, amnestic, andanalgesic properties.7
Additionally, it has a decongestant effect and induces hypotension in tympanoplasty surgeries.8,9
Dexmedetomi-dine has been also used in ESS patients under local anesthesia,10,11aswellasinseptoplastyandtympanoplasty
patientsundergeneralanaesthesia;ithasbeenstatedthat it decreases the bleedingscore and reducesthe required amountoffentanyl.12
Therefore,inourstudywecomparedtheeffectsof mag-nesium and dexmedetomidine, which areused duringESS in patients undergeneral anaesthesia,primarily on surgi-calvisionqualityandonhaemodynamicsandpostoperative analgesia.
Methods
Aftertheapproval ofthe University ofAbant IzzetBaysal Clinical Research Ethics Committee, document number 2011/97,we enrolled60patientsof theAmericanSociety of Anesthesiologists (ASA) risk classification I---II accord-ingtothe pre-anaesthetic evaluation, ranging from18 to 45 years of age who were scheduled to have an elec-tivefunctionalESSoperation.Thepatientswererandomly divided into two groups of 30 people: the magnesium group (Group M) and the dexmedetomidine group (Group D). The control group without hypotensivedrugs wasnot used due to ethical concerns, and the two agents were compared.Patientswhowere allergictoanyof thedrugs that would be used in the study, those who had hyper-magnesaemia,wereopioid-dependent,hadseverecardiac, renal,neurological, and liver diseases, and had a history ofpostoperativenausea/vomitingwereexcluded fromthe study.
Prior to surgery, the patients were taken to the preoperative preparation room, and 0.5mg atropine sul-phate(Atropineampoule,0.5mgmL−1,Biofarma,Istanbul,
Turkey) andmidazolam 0.1mgkg−1 (Dormicum1mgmL−1,
Roche müstahzarlari san, Istanbul, Turkey) were applied intramuscularly30min beforethe patients were taken to theoperatingtable.
In theoperating room,all patientswho weregiven O2
at 2Lmin−1 with a nasal cannula received
electrocardio-gram monitoring, and the heart rate (HR), mean arterial pressure (MAP), peripheral oxygen saturation (SpO2), and
respiratoryrate (RR)were alsomonitored (DragerInfinity XLmonitor).Anaesthesiawasinducedwith50mcgfentanyl (fentanyl citrateflakon 50mcgmL−1, Meditera Ltd.
Istan-bul,Turkey), 1.5mgkg−1 propofol (Propofol 1% Fresenius,
Istanbul, Turkey), and 0.5mgkg−1 rocuronium bromides
(Esmeron5mgflakon,Organon,Istanbul).Anaesthesiawas maintained with 50% O2, 50% N2O, and 1.5% sevoflurane
(Sevorane,Abbott,Istanbul,Turkey).Musclerelaxationwas maintainedwith0.15mgkg−1rocuroniumbromideandused
whenneeded.
Patients were randomly divided into twoequal groups by the closed card method by a supervisor who did not participatein the other sequencesof the study.In Group M,theinfusion ofmagnesiumsulphate wasstarted before induction at a loading dose of 50mgkg−1 for 10min, and
then was sustained throughout the operation at a main-tenance dose of 15mgkg−1h−1 intravenously. In Group D,
before induction, 1mcgkg−1 for 10min of
dexmedetomi-dinewasgivenby infusion, andduringthe operation,the maintenance dose of 0.6mcgkg−1h−1 was administered.
After induction, the operation table was positioned in a 10◦reverseTrendelenburgposition,and1mLoflocal anaes-theticwasappliedtothepterygopalatine fossa(Lidocaine hydrochloride20mgmL−1,Epinephrinebase0.0125mgmL−1
(Jetokainampoule2mL,Adeka,Istanbul)).Theintubation tubewasfixed withadhesivetapearoundthemouth. Pos-itive end-expiratory pressure (PEEP) was limited to 1cm H2O. The total duration of the operation was recorded.
At the end of surgery, the muscle relaxation effect was antagonized with the use of atropine 0.01mgkg−1 and
neostigmine 0.05mgkg−1. Surgical team, postoperative
measurementteams(anesthesiologyassistants)andpatients wereunawareofthedrugsthathadbeenused.
Patientswere followed upprior tointubation and also 1,2, 3,5, 10, 15,20, 30, 40,50, 60, 70,80, and 90min afterintubationintermsofMAP,RR,SpO2,nausea/vomiting,
itching,adverseeffects,complicationsofanaesthesia,and surgicalcomplications.At theendof theoperation,when thebodytemperatureofthepatientswas>36degrees Cel-sius and their modified Aldrete score was=9, they were extubated,andpostoperativefollow-upwasdone.Patients were evaluated before extubation and 0, 5, 10, 20, 30, 60min after extubation in terms of MAP, RR, SpO2,
nau-sea/vomiting, itching, adverse effects, complications of anaesthesia, and surgical complications. In the postop-erativeperiod,4-point nausea/vomitingscale for nausea, 11-unitNumericalPainScoring(NPS11)13forpainevaluation,
RamsaySedation Scale for the sedationdegree, and Intra OperativeSurgicalFieldEvaluation(IOSFE)Scale14 to
mea-surebleedingatthesurgicalareawereemployed.Thisscale wasused because any blood aspirated from the bleeding
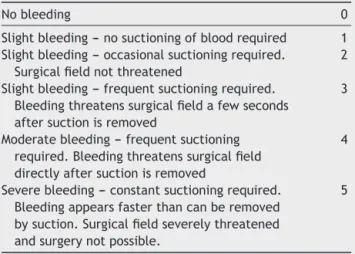
Table 1 Intraoperative surgical field evaluation scale: IOSFE:BoezaartScale.
Nobleeding 0
Slightbleeding---nosuctioningofbloodrequired 1 Slightbleeding---occasionalsuctioningrequired.
Surgicalfieldnotthreatened
2
Slightbleeding---frequentsuctioningrequired. Bleedingthreatenssurgicalfieldafewseconds aftersuctionisremoved
3
Moderatebleeding---frequentsuctioning required.Bleedingthreatenssurgicalfield directlyaftersuctionisremoved
4
Severebleeding--- constantsuctioningrequired. Bleedingappearsfasterthancanberemoved bysuction.Surgicalfieldseverelythreatened andsurgerynotpossible.
5
areamixeswiththewashingsolution,andtheamountof liq-uidescapingtothestomachgreatlyvariesfrompatientto patientandpreventsmathematicalcalculationsfrombeing doneonthebasisoftheliquidaccumulatedintheaspirator alone. Table 1 shows the IOSFE scale. Nausea and vomi-ting scale was described asfollows: no nausea/vomiting, mildnausea/vomiting(treatmentnotindicated),moderate nausea/vomiting (treatment indicated) and severe nau-sea/vomiting(resistivetotreatment).
In case of intraoperative anaesthetic depth failure, 1mcgkg−1offentanyl(fentanylcitrate,flakon50mcgmL−1,
MediteraLtd.,Istanbul,Turkey)intravenously(IV)was avail-able.
Forpostoperativeanalgesia,1mgkg−1ofpethidineHCL
was given intramuscularly (IM) (Aldolan ampoule 100mg, 2mL, Liba Ilac Sanayi) when the NPS11 value was 4 or more; for nausea/vomiting, 0.25mgkg−1 IV of
metoclo-pramide(Avilampoule,50mg,2mL,Istanbul,Turkey)was onhand.
StatisticalanalysiswasdoneviatheSPSS11.5statistical package(SPSS,Chicago,IL,USA).FortheIOSFEscale,the Mann---WhitneyUtestwasusedtocomparethemeanvalues betweengroups.Calculationswereperformedwith indepen-dent ttestsforthe averageofnumerical datadistributed normally andwiththe Chi-square test using a cross-table forthefrequencyanalysisofdata,suchasthepercentage ofmalesvs.females.Whencalculatingthenumberof par-ticipantstoincludeinthestudy,thefollowingparameters wereused:theIOSFEScale,whichwastheprimaryoutput, neededtohaveanaveragevalueof2or3betweensimilar studygroups;theapproximatestandarddeviationshouldbe close to1.1; the alpha error margin should be 0.05 with theconsiderationofbipolarprobabilityandabnormal logis-ticcharacterofthedistribution;thepower value(1-beta) neededtobe0.95;andthesamplesizewascalculatedas30 pergroup.
Results
Table2 Theaveragevalueofpatients’age,weight,anddurationofoperation.
Eachgroup’sn=30 Age Weight DurationofOp.
Mg
Mean±SD 42.9±15.1 74.9±12.1 50.2±18.6
%95CI 37.3---48.5 70.4---79.4 43.2---57.1
Dex
Mean±SD 42.5±16.1 74.9±13.4 51.0±14.8
%95CI 36.5---48.6 69.9---79.9 45.5---56.5
SD,standarddeviation;CI,confidenceinterval.
female/maleratiowas8/22inGroupMand12/18inGroup D,andtherewasnosignificantdifferencebetweenthetwo (p=0.273).
Meanarterialpressure(MAP)analysisrevealed thatthe bloodpressurewaslowerforashortperiodoftimeinGroup D at the 35th and65thmin. The p-values of the minutes atwhichasignificantdifferencewasobservedaregivenin
Fig.1.The datashownat theleftsideof thedashedline indicatethatthefirst88%ofthecaseswerecompletedin lessthan70min.
No differencewasdetected duringand afterthe oper-ation in the values of SpO2 and respiratory rates, or
from extubation until the first postoperative hour in the values of the nausea/vomiting scale and the NPS11. None of the patients needed intraoperative fentanyl or postoperative analgesic, anti-emetics, or anti-pruritic agents.
IntheanalysisofHR,fromthepre-intubationperioduntil the 20thmin and at the 35th, 40th, and 45thmin, it was observedthattheHRwassignificantlyslowerinGroupD.As showninFig.2,thecourseoftheHRvaluesatthefollowing minutesispresentedwithp-valuesandtheline,indicating that88%ofthecaseswerecompleted.
Itwasnotedthattheconfidenceintervalofthesurgery durationwaswiderinGroupD.
Thelongestcasewas90mininGroupM,andthe short-estcase was20min, ofwhich therewasonecase in both thegroups.Sixcases inGroupMandonein GroupD took longerthan70min.Whenthesefrequencieswerecompared, asignificantdifferenceinfavour ofGroupD wasobserved (p=0.044). The percentage ofthe casesthat lastedmore than70minwassignificantlyhigherinGroupMthaninGroup D.
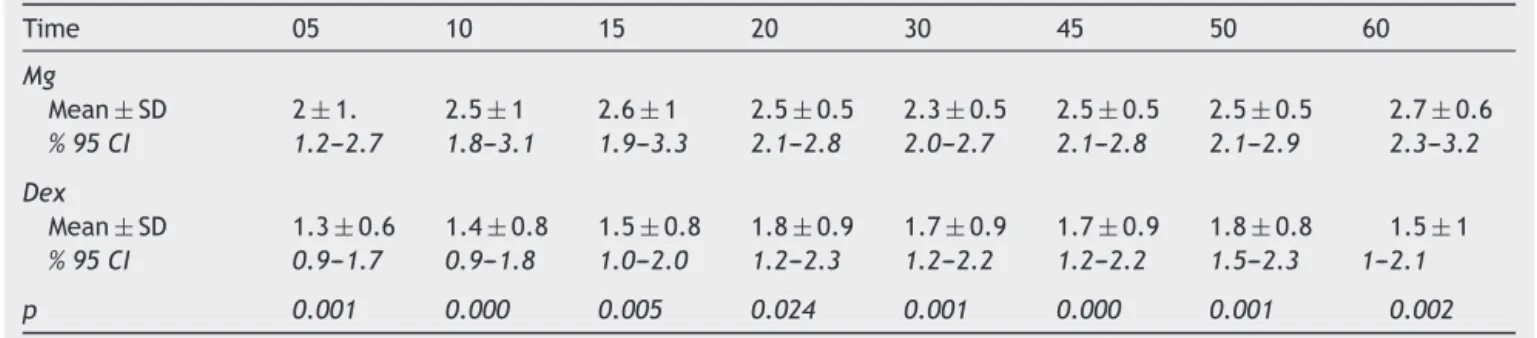
ThetargetoutputofourstudywastheIOSFEscale,and it had a significantly low level statistically in Group D at the5th,10th,20th,30th,45th,and60thmin, asshownin
Table3.Inbothgroups,theinternationalnormalizedratio (INR)valuesofpatientswerelowerthan1.33.
Discussion
Inour study,nosignificant difference wasfound in terms ofage,weight,gender,anddurationofoperationbetween thetwogroups.ForHR,significantandmeaningful deceler-ationswereobservedinGroupDfromtheoperation’sstart
Cases of %88 in the left side of the dashed line
Minute Mg
Dex
–5 0 120
100
80
60
40
20
0
5 10 15 20 25 30 35 40 45 50 55 60 65 70 75 80 85 90
Table3 TheIOSFEScale:Mean±SD,%95CIandP-values.
Time 05 10 15 20 30 45 50 60
Mg
Mean±SD 2±1. 2.5±1 2.6±1 2.5±0.5 2.3±0.5 2.5±0.5 2.5±0.5 2.7±0.6
%95CI 1.2---2.7 1.8---3.1 1.9---3.3 2.1---2.8 2.0---2.7 2.1---2.8 2.1---2.9 2.3---3.2
Dex
Mean±SD 1.3±0.6 1.4±0.8 1.5±0.8 1.8±0.9 1.7±0.9 1.7±0.9 1.8±0.8 1.5±1
%95CI 0.9---1.7 0.9---1.8 1.0---2.0 1.2---2.3 1.2---2.2 1.2---2.2 1.5---2.3 1---2.1
p 0.001 0.000 0.005 0.024 0.001 0.000 0.001 0.002
SD,standarddeviation;CI,confidenceinterval.
untilthe45thmin. The decelerationslastedfora totalof 35min.Consideringthattheaveragedurationofthesurgical procedurewas50min,itcanbeinferredthat dexmedetomi-dineprovidedanotabledecreaseinHRduringthemajority ofthesurgerycomparedtomagnesium.Thepositiveeffects ofadecreaseinHRonbleedingareknown.2WhentheMAP
wascompared,nosignificant differencebetweenthe two drugsintermsofblood pressurewasidentifiedduetothe observation of decreases occurring only at the 35th and 65thmin, the total decrease time being 10min, and this timeremainingshorterinregardtoaverageoperationtime. We did not use a control group in the study because we considered it unethical not totry to control bleeding in the surgical field without active precautions, such as deliberatehypotensiontoreducebleeding; alsothe surgi-calteam demanded. Pre- and postoperative haemoglobin valueswerenotcomparedinthisstudybecausetheblood
lostduringESSislowenoughnottoexpectanysignificant laboratory measurement differencesevery time,although evensmallamountsrestrictsurgicalvisioninanarrow oper-ativefield.11,15,16Whilethetotalbloodlostdoesnotrequire
transfusion (100---300mL), numerous techniques toreduce bleedinghave beendeveloped duetotheloss ofvision in the surgical area when blood is present.5,11,17---21 Some of
thesearesteroids,tranexamicacid,deliberatehypotension agents, sevoflurane, total intravenous anaesthesia (TIVA), andvariouspatientpositions.Theliteraturehasshownthat alackofvisioninthesurgicalfieldextendsthedurationof theoperationandincreasestherateofcomplications.22---25In
themajorityofpublicationsthathaveinvestigatedtheissue, surgical field clarity outranked the amount of bleeding. Otherstudies11havebeenunabletofindasignificant
differ-encebetweenpostoperativehaemoglobinvaluesandhave identifieddifferencesinsurgicalfieldevaluation;similarly,
Cases of %88 in the left side of the dashed line
Minutes
Mg Dex
0 110.0
100.0
90.0
80.0
70.0
60.0
50.0
40.0
30.0
Pre-entubPost-entub
5 10 15 20 25 30 35 40 45 50 55 60 65 70 75 80 85 90
studies have found different levels of bleeding between twogroupsbuthaveindicatedthatthisdifferencedoesnot affectsurgicalvision.23Notallbloodleaksthatoccurduring
endoscopicsinussurgeryareobservedin thefrontpartof thesurgical area;the leakscansometimes findtheir way outsideofthevisiblefieldandreachthepharynx.This sit-uation explains why the amount of haemorrhage and the surgicalvisionqualityaresometimesirrelevant.
Inourstudy,nostatisticaldifferencewasfoundinterms ofthemeandurationofsurgery(p=0.74).However,96.6%of thecasesinGroupDwerecompletedbefore70min,whereas inGroupM,thispercentagewas80%.Whenthedistribution of the casesof both groups that lasted morethan 70min wascomparedwiththetotal groupnumbervia frequency analysis,theprobabilityvaluewasp=0.044.Inotherwords, inGroupM,morepatientsrequiredaprolongedsurgery.This observationsupportedthelimitationofvisioninthesurgical field.
Inmanystudiesthathaveresearchedthedrugsusedto reducebleedinginendoscopicsinussurgery,theeffectsof the aforementioned drugs on the need for postoperative analgesics have also been investigated and presented as a secondary outcome. Somestudies have argued that the painwaslessin thesesurgeries.26 Inour study,regardless
of the group, all of the NPS11 values were=4, which is therecommendedvaluetoprovidepreemptiveanalgesicsin thepostoperativeperiod,sothatpointwasneverreached. WhentheNPS11valueswereanalyzed,nosignificant differ-encewasfoundatanyofthemeasurementpointsinthefirst postoperativehour.
Some publications suggest that TIVA is preferable to inhalation anaesthesia in endoscopic sinus surgery.27
Whether theyfitthe definitionof TIVAor not,the impor-tanceofevokedhypotensionprovidedbysomeintravenous agentsisobvious.20,21,28Propofolandremifentanilareonly
someofthem.
Magnesium is an agent that has been indicated to decreaseMAPundergeneralanaesthesiaandreducetheHR, aswellastolessentheneedforanaestheticsubstanceand toreducebleeding.Italsomakesapositivecontributionto thepostoperativepainscore.29
Magnesium also does not cause reflex tachycardia when used as an intraoperative hypotensive agent, does not produce reflex hypertension, and does not lower cardiac output.30 In a randomized, double-blind, and
placebo-controlledclinicaltrialconductedwith60patients scheduled for endoscopic surgery, they found a statisti-callysignificantlowerHRandMAPinthemagnesiumgroup than theydidin theircontrol group.5 Also,thequalityof
vision of the surgical field was higher in the magnesium group.Inthesamestudy,theoperativetimeinthecontrol group wassignificantlyprolonged, whereas inthe magne-siumgroup,thedurationofanaesthesiahadbeenprolonged depending on the postoperative awakening. However, in operations that require general anaesthesia, a partially disadvantageous feature of magnesium is that it reduces acetylcholine release31 and extends the effects of
neuro-muscularblockers;32somepublicationshavealsoindicated
differenteffectsonclottingmechanisms.33
Dexmedetomidineisadrugthatisnotyetapprovedinthe UnitedStatesbytheFoodandDrugAdministration(FDA)for useundergeneralanaesthesia.Inoneretrospectivestudy,
1134patientswhoreceiveddexmedetomidineinthe periop-erativeperiodwereexamined,andfavourableresultswere reported.34 Dexmedetomidine had been used both as an
adjuvant35toregionalanaesthesia,anintravenousaddition
toeliminate negative effects of intubation36,37 in general
anaesthesia,andasamethodtoprovidecontrolled hypoten-sion.
Jalonenand hiscolleagues hadused dexmedetomidine asan anaesthetic adjuvant inopen heart surgeryin coro-naryarterygrafting,andtheyfoundthatthehyperdynamic responsetosurgery andanaesthesiawassignificantly sup-pressed in the dexmedetomidine group compared to the controlgroupinan80-patientstudy.38Guvenetal.11
inves-tigatedtheeffectivenessofdexmedetomidineonbleeding, haemodynamicparameters,andpostoperativeanalgesiain their study that included over 40 patients scheduled for functionalendoscopicsinussurgeryinrandomized, prospec-tive,andcontrolgroups.Nodifferencewasfoundbetween pre-andpostoperativehaemoglobinvalues.However,they reported a significant difference in the bleeding score (p=0.019).Inourstudy,significantdifferenceswerefound inHRaswellassurgicalareaevaluationscaleintheGroup DcomparedtoGroupM.
InESS,agentsprovidingcontrolledhypotensionandTIVA have emerged with the purpose of surgical field clarity. Therefore,we tested thesuperiority oftwoagents, mag-nesiumand dexmedetomidine,against each otherfor this purpose.
Thistopicisasubjectthatisstillofinterest,andanother intravenousagent,remifentanil, isalsoincreasingly being used.39Inthefuture,webelievethatthenumberof
effec-tiveandreliabledrugsforESSwillcontinuetodevelop,but theinterestwill beclarified toconcentrateoninnovative methods.
Theresultsobtainedfromourresearchhaveshownthat dexmedetomidineprovidedbettervisualqualityofthe sur-gicalfieldcomparedtomagnesiumwhenusedinESSpatients under general anaesthesia. As a result, we believe that inendoscopic sinus surgeries,dexmedetomidine is agood alternativetomagnesiumduetoitshigherreducingeffect onbleedinginthesurgicalfieldandthegreatersuppression ofHRcomparedtomagnesium.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.Drozdowski A, Sieskiewicz A, Siemiatkowski A. Reduction of intraoperative bleeding during functional endoscopic sinus surgery.AnaesthesiolIntensiveTher.2011;XLIII:43---7.
2.MilonskiJ,Zielinska-BlizniewskaH,GolusinskiW,etal.Effects ofthreedifferenttypesofanaesthesiaonperioperative bleed-ing control in functional endoscopic sinus surgery. Eur Arch Otorhinolaryngol.2013;270:2045---50.
4.Kastl KG, Betz CS, Siedek V, et al. Control of bleeding following functional endoscopic sinus surgery using carboxy-methylated cellulose packing. Eur Arch Otorhinolaryngol. 2009;266:1239---43.
5.Elsharnouby NM, Elsharnouby MM. Magnesium sulphate as a technique of hypotensive anaesthesia. Br J Anaesth. 2006;96:727---31.
6.NaHS,ChungYH,HwangJW,etal.Effectsofmagnesium sul-phate on postoperativecoagulation, measured byrotational thromboelastometry.Anaesthesia.2012;67:862---9.
7.AfonsoJ,ReisF.Dexmedetomidine:currentroleinanesthesia andintensivecare.RevBrasAnestesiol.2012;62:118---33.
8.Richa F, Yazigi A, Sleilaty G, et al. Comparison between dexmedetomidineandremifentanilforcontrolledhypotension duringtympanoplasty.EurJAnaesthesiol.2008;25:369---74.
9.Paranjpe J.Dexmedetomidine: expandingroleinanesthesia. MedJDYPatilUniv.2013;6:5---13.
10.GoksuS, ArikH,Demiryurek S,et al.Effects of dexmedeto-midine infusionin patientsundergoingfunctional endoscopic sinus surgery under local anaesthesia. Eur J Anaesthesiol. 2008;25:22---8.
11.GuvenDG,DemiraranY,SezenG,etal.Evaluationofoutcomes in patients given dexmedetomidine in functional endoscopic sinussurgery.AnnOtolRhinolLaryngol.2011;120:586---92.
12.Ayoglu H, Yapakci O, Ugur MB, et al. Effectiveness of dexmedetomidineinreducingbleedingduringseptoplastyand tympanoplastyoperations.JClinAnesth.2008;20:437---41.
13.WilliamsonA,HoggartB.Pain:areviewofthreecommonlyused painratingscales.JClinNursing.2005;14:798---804.
14.Boezaart AP, van der Merwe J, Coetzee A. Comparison of sodiumnitroprusside-andesmolol-inducedcontrolled hypoten-sion for functional endoscopic sinus surgery. Can JAnaesth. 1995;42:373---6.
15.Pavlin JD, Colley PS, Weymuller Jr EA, et al. Propofol ver-susisofluraneforendoscopicsinussurgery.AmJOtolaryngol. 1999;20:96---101.
16.Manola M, De Luca E, Moscillo L, et al. Using remifen-tanil andsufentanilinfunctional endoscopicsinussurgeryto improvesurgicalconditions.ORLJOtorhinolaryngolRelatSpec. 2005;67:83---6.
17.AlbuS,GoceaA,MitreI.Preoperativetreatmentwithtopical corticoidsandbleedingduringprimaryendoscopicsinussurgery. OtolaryngolHeadNeckSurg.2010;143:573---8.
18.BeuleAG,WilhelmiF,KuhnelTS,etal.Propofolversus sevoflu-rane: bleedinginendoscopicsinus surgery.OtolaryngolHead NeckSurg.2007;136:45---50.
19.Ko S.Does choiceofanesthetics affectintraoperative blood loss?KoreanJAnesthesiol.2012;63:295---6.
20.BoonmakS,BoonmakP,LaopaiboonM.Deliberatehypotension withpropofolunderanaesthesiaforfunctionalendoscopicsinus surgery(FESS).CochraneDatabaseSystRev.2013;6:CD006623.
21.YooHS,HanJH,ParkSW,etal.Comparisonofsurgical condi-tioninendoscopic sinussurgeryusing remifentanilcombined withpropofol,sevoflurane,ordesflurane.KoreanJAnesthesiol. 2010;59:377---82.
22.AbbasiH,BehdadS,AyatollahiV,etal.Comparisonoftwodoses oftranexamicacidonbleedingandsurgerysitequalityduring sinusendoscopysurgery.AdvClinExpMed.2012;21:773---80.
23.AtighechiS,AzimiMR,MirvakiliSA,etal.Evaluationof intraop-erativebleedingduringanendoscopicsurgeryofnasalpolyposis
afterapreoperativesingledoseversusa5-daycourseof corti-costeroid.EurArchOtorhinolaryngol.2013;270:2451---4.
24.ChaabanMR,Baroody FM, GottliebO, et al. Bloodloss dur-ingendoscopic sinus surgery withpropofol orsevoflurane: a randomizedclinicaltrial.JAMA OtolaryngolHead NeckSurg. 2013;139:510---4.
25.AhnHJ,ChungSK,DhongHJ,etal.Comparisonofsurgical condi-tionsduringpropofolorsevofluraneanaesthesiaforendoscopic sinussurgery.BrJAnaesth.2008;100:50---4.
26.BlackwellKE,RossDA,KapurP,etal.Propofolformaintenance ofgeneralanesthesia:atechnique tolimitbloodlossduring endoscopicsinussurgery.AmJOtolaryngol.1993;14:262---6.
27.KhoslaAJ,PernasFG,MaesoPA.Meta-analysisandliterature reviewoftechniquestoachievehemostasisinendoscopicsinus surgery.IntForumAllergyRhinol.2013;3:482---7.
28.Sieskiewicz A, Drozdowski A, Rogowski M. The assess-ment of correlation between mean arterial pressure and intraoperative bleeding during endoscopic sinus surgery in patients with low heart rate. Otolaryngol Pol. 2010;64: 225---8.
29.Koinig H, Wallner T, Marhofer P, et al. Magnesium sulphate reducesintra-andpostoperativeanalgesicrequirements. Anes-thesiaandanalgesia.1998;87:206---10.
30.Crozier TA, Radke J, Weyland A, et al. Haemodynamicand endocrineeffects ofdeliberate hypotension withmagnesium sulphate for cerebral-aneurysm surgery. Eur J Anaesthesiol. 1991;8:115---21.
31.WangH,LiangQS,ChengLR,etal.Magnesiumsulfateenhances non-depolarizingmusclerelaxant vecuroniumaction atadult muscle-type nicotinic acetylcholine receptor in vitro. Acta PharmacolSin.2011;32:1454---9.
32.HansGA,BosengeB,BonhommeVL, etal. Intravenous mag-nesiumre-establishes neuromuscularblockafterspontaneous recoveryfromanintubatingdoseofrocuronium:arandomised controlledtrial.EurJAnaesthesiol.2012;29:95---9.
33.SandersGM,SimKM.Isitfeasibletousemagnesiumsulphateas ahypotensiveagentinoralandmaxillofacialsurgery?AnnAcad MedSingapore.1998;27(6):780---5.
34.Ji F, Li Z, Nguyen H, et al. Perioperative dexmedeto-midine improves outcomes of cardiac surgery. Circulation. 2013;127:1576---84.
35.ElcicekK,TekinM,KatiI.Theeffectsofintravenous dexmedeto-midineonspinalhyperbaricropivacaineanesthesia.JAnesth. 2010;24:544---8.
36.KeniyaVM,Ladi S,NaphadeR. Dexmedetomidineattenuates sympathoadrenalresponsetotrachealintubationandreduces perioperative anaesthetic requirement. Indian J Anaesth. 2011;55:352---7.
37.YavascaogluB, Kaya FN, Baykara M, et al. A comparison of esmololand dexmedetomidine for attenuationofintraocular pressureandhaemodynamicresponsestolaryngoscopyand tra-chealintubation.EurJAnaesthesiol.2008;25:517---9.
38.JalonenJ,HynynenM,KuitunenA,etal.Dexmedetomidineas ananestheticadjunctincoronaryarterybypassgrafting. Anes-thesiology.1997;86:331---45.