www.jped.com.br
ORIGINAL
ARTICLE
Can
procalcitonin
be
a
diagnostic
marker
for
catheter-related
blood
stream
infection
in
children?
夽
Yasemin
Ozsurekci
a,∗,
Kamile
Oktay
Arıkan
a,
Cihangül
Bayhan
a,
Eda
Karada˘
g-Öncel
a,
Ahmet
Emre
Aycan
a,
Venhar
Gürbüz
a,
Güls
¸en
Hasc
¸elik
b,
Mehmet
Ceyhan
aaDepartmentofPediatricInfectiousDiseases,FacultyofMedicine,HacettepeUniversity,Ankara,Turkey bDepartmentofMicrobiology,FacultyofMedicine,HacettepeUniversity,Ankara,Turkey
Received12August2015;accepted4November2015 Availableonline27April2016
KEYWORDS
Biomarkers; Bloodstream infection; Children;
C-reactiveprotein; Procalcitonin
Abstract
Objective: Thepotentialroleofprocalcitonin(PCT)inthediagnosisofcatheter-related blood-streaminfection(CRBSIs)isstillunclearandrequiresfurtherresearch.Thediagnosticvalueof serumPCTforthediagnosisofCRBSIinchildrenisevaluatedhere.
Method: ThisstudywasconductedbetweenOctober2013andNovember2014,andincluded patientswithsuspectedCRBSIfrom1monthto18yearsofagewhowerefebrile,withnofocusof infection,andhadacentralvenouscatheter.LevelsofPCTandotherserummarkerswere mea-sured,andtheirutilityasCRBSImarkerswasassessed.Additionally,theclinicalperformance ofanew,automated,rapid,andquantitativeassayforthedetectionofPCTwastested.
Results: Amongthe49patients,24werediagnosedwithCRBSI.ThePCT-KryptorandPCT-RTA valuesweresignificantlyhigherinprovenCRBSIcomparedtothoseinunprovenCRBSI(p=0.03 andp=0.03,respectively).TherewerenodifferencesinwhitebloodcellcountandC-reactive protein(CRP)levelsbetweenprovenCRBSIandunprovenCRBSI.Amongthe24patientswith CRBSI,CRPwassignificantlyhigheramongthosewithGram-negativebacterialinfectionthanin thosewithGram-positivebacterialinfections.PCT-Kryptorwasalsosignificantlyhigheramong patients with Gram-negative bacterial infectionthan inthose withGram-positive bacterial infections(p=0.01andp=0.02,respectively).
Conclusions: TheauthorssuggestthatPCTcouldbeahelpfulrapiddiagnosticmarkerinchildren withsuspectedCRBSIs.
©2016SociedadeBrasileiradePediatria.PublishedbyElsevierEditoraLtda.Thisisanopen accessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/licenses/by-nc-nd/
4.0/).
夽
Pleasecitethisarticleas:OzsurekciY,OktayArıkanK,BayhanC,Karada˘g-ÖncelE,EmreAycanA,GürbüzV,etal.Canprocalcitoninbe adiagnosticmarkerforcatheter-relatedbloodstreaminfectioninchildren?JPediatr(RioJ).2016;92:414---20.
∗Correspondingauthor.
E-mail:[email protected](Y.Ozsurekci).
http://dx.doi.org/10.1016/j.jped.2015.11.004
PALAVRAS-CHAVE
Biomarcadores; Infecc¸ãodacorrente sanguínea;
Crianc¸as;
ProteínaCreativa; Procalcitonina
Aprocalcitoninapodeserummarcadordediagnósticodeinfecc¸õesdecorrente sanguínearelacionadasacateteremcrianc¸as?
Resumo
Objetivo: Opossívelpapel daprocalcitonina (PCT)nodiagnóstico deinfecc¸õesde corrente sanguínearelacionadasacateter(ICSRCs)aindanãoestáclaroeprecisasermaispesquisado. Ovalordiagnóstico daPCT séricaparaodiagnóstico deICSRCemcrianc¸aséavaliadoneste estudo.
Método: Esteestudofoifeitoentreoutubrode2013enovembrode2014eincluiupacientes comsuspeitadeICSRCdeum mêsa18 anosdeidade queestavamfebris,não tinhamfoco de infecc¸ão etinhamcateter venosocentral. Forammedidos osníveis de PCT ede outros marcadoresséricos,cujautilidadecomomarcadoresdeICSRCfoiavaliada.Adicionalmente,foi testadoodesempenhoclínicodeumnovoensaioquantitativoautomatizadoerápido paraa detecc¸ãodePCT.
Resultados: Dentre49pacientes,24foramdiagnosticadoscomICSRC.OsvaloresdePCT-Kryptor ePCT-RTAforamsignificativamentemaioresemICSRCscomprovadasdoqueemICSRCsnão com-provadas(p=0,03ep=0,03,respectivamente).Nãohouvediferenc¸anacontagemdeglóbulos brancosenosníveisdeproteínaCreativa(PCR)entreICSRCscomprovadaseICSRCsnão compro-vadas.Dentreos24pacientescomICSRC,aPCRerasignificativamentemaiorentreaquelescom infecc¸ãobacterianagram-negativadoquenaquelescominfecc¸ãobacterianagram-positiva.O PCT-Kryptortambémfoisignificativamentemaiorentrepacientescominfecc¸ãoporbactérias gram-negativasdoquenaquelescominfecc¸ãoporbactériasgram-positivas(p=0,01ep=0,02, respectivamente).
Conclusões: SugerimosqueaPCTpodeserummarcadordediagnósticorápidoútilemcrianc¸as comsuspeitadeICSRCs.
©2016SociedadeBrasileiradePediatria.PublicadoporElsevierEditoraLtda.Este ´eumartigo OpenAccesssobumalicenc¸aCCBY-NC-ND(http://creativecommons.org/licenses/by-nc-nd/4.
0/).
Introduction
Central venous catheters (CVCs) are generally used to administerintravenousfluids,medications,bloodproducts, and parenteral nutrition fluids, to monitor hemodynamic status, and to provide hemodialysis.1 Catheter-related
bloodstream infections (CRBSIs) are the leading cause of nosocomiallyacquiredsepsisincludingneonatalsepsis,2and
are associated with significant morbidity, mortality, and hospital costs.1,3 Early diagnosis of CRBSIs and
appropri-ate treatment may reduce the associated morbidity and mortality.4,5 The laboratory criteria for diagnosing CRBSIs
are precise; however, differences in the definitions and methodologiesamongvariousstudieshavemadeitdifficult tocomparethe results.1,6Confirmationof CRBSIsrequires
theidentificationof microorganismsrecovered fromblood andcathetertips.Althoughbloodcultureisthebestmethod for the diagnosis of bloodstream infections, test results arenotrapidlyavailable.Additionally, only15---25%of the CVC tips that reach the microbiology laboratory turn out tobeculture-positive.Furthermore,notallCRBSIsrequire thecatheter tobewithdrawn.7,8Therefore, thediagnosis
ofCRBSIsbyconservativemethods(withoutcatheter with-drawal)appearstobemorereasonableinclinical settings toavoidunnecessaryremovalofthevascularcatheterand antibioticoveruse.9
Sincetheremovalofsuchdevicesis oftenachallenge, trueCRBSIshouldbeconfirmedtodistinguishitfrom con-taminated blood cultures, catheter colonization without
concomitantbloodstreaminfection,orfever fromanother source.Variousmethodshavebeenpreviouslyusedto diag-noseCRBSIwithoutcatheterremoval.1Earlyandestablished
biomarkersmaybeusefulfordiagnosis,prognosis,and mon-itoringofresponsetotherapy.10Commonlyusedbiomarkers
such as white blood cells (WBCs) or C-reactive protein (CRP) lack adequate specificity for the diagnosis of bac-terialinfections.9Serumprocalcitonin (PCT),a116-amino
acidpolypeptide,hasrecentlyemergedasabiomarkerfor thediagnosis of variousbacterial infections. It wasfound tohavea higherdiagnostic accuracywhencomparedwith othercommonlyusedlaboratoryparameters,suchasWBC andCRP.11---13PCTlevelsarefoundtobelowerintheserum
ofhealthyhumans,but aresignificantlyelevated inthose sufferingfromsevereinfections,particularlysepsis.14,15 To
thebestoftheauthor’sknowledge,onlyafewstudieshave assessedthe rationale behindPCT levelsfor the accurate diagnosisofCRBSIs,16,17especiallyinchildren.
Thus,thepresentstudyaimedtoevaluatetheaccuracy ofPCTforthediagnosisofCRBSIsinchildren.Furthermore, theclinical performance of a new, automated, and rapid quantitativeassaywasalsoexamined.
Materials
and
methods
hadacentralvenous catheterwereenrolledinthe study. Theinvestigationwasreviewedandapprovedbythe ethi-calcommitteeoftheZekai TahirBurakMaternityTeaching Hospital,MinistryofHealth,Ankara,Turkey.
Clinical suspicion of CRBSI was based on the onset of thefollowing features suggestive of infection:(a) clinical manifestationsof infection(fever, chills, and/or hypoten-sion);(b)useofcentralvenouscatheterforover48h;and (c)nootherapparentsourceofinfection.1Incasedof
sus-pectedCRBSI,pairedbloodsamplesfromthecatheterand aperipheralveinwereobtainedandsubmittedforculture test.1
According to previously published guidelines, a defini-tivediagnosisof CRBSIrequireseitherthe isolationofthe sameorganism fromtheperipheral blood culture andthe cultureofthecathetertiporpositiveculturefromboththe catheterhubandbloodfromperipheralvein,meetingthe CRBSIcriteria.1,16
Patientswith any active infection other than CRBSI or thosewhoshowedculture negativitydespitethesuspicion ofCRBSIwere excludedfromthe study(13 patients).Ifa patienthadmorethanoneepisodeofsuspectedCRBSIduring thestudyperiod,onlythefirstepisodewasincluded.
For monitoring purposes, patients with proven CRBSI were categorized into two subgroups depending on the infectioncontrol: (a) controlled, patients withcontrolled infection (n=20), defined as clinical and microbiological improvement,and(b)notcontrolled,patientswith uncon-trolledinfection (n=4), defined aspersistent bacteremia (the same pathogen responsible for the firstepisode was cultured 72h after catheter removal or 72h after initia-tionof the appropriate treatment), superinfection (CRBSI due to another pathogen during the therapy period), or deathrelatedtoCRBSI.16 Mortalitywasdefinedasrelated
toCRBSIifdeathoccurredwithinthefirst28daysofCRBSI suspicion.
Blood samples were assessed for routine hematology andbiochemistrypanels, aswell asfor PCT andCRP lev-els. PCT levels were determined using Brahms Kryptor® compactimmunoassayanalyzer(Thermofisher,Hennigsdorf, Germany) and RTA® Procalcitonin device (RTA, Kocaeli, Turkey) simultaneously. Both assays required a minimum of 80L serum, and tested positive if PCT levels were greater than 0.5ng/mL, according to the manufacturer’s instructions.Preferably,freshserumsampleswereusedfor measurements.However,ifsampleswerenot usedonthe sameday,theywerefrozenat−20◦C.
Statisticalanalysis
Data were analyzed using the SPSS version 19.0 (SPSS, Inc. --- Chicago, USA). Descriptive statistics were used to summarize the participants’ baseline characteristics, includingmeans, standard deviations (SDs), medians,and interquartilerangesforcontinuousvariablesandfrequency distributionsforcategoricalvariables.Tocomparethe base-line characteristics according totheoccurrence of CRBSI, the2testwasusedforcategoricalvariables.Thenormality
ofquantitativevariableswastestedbyKolmogorov---Smirnov test. For continuous variables, the independent-groups t
test was used for normally distributed variables or the
nonparametric Mann---Whitney U test, if the normality assumptionwasviolated.Theareaunderthereceiver oper-atingcharacteristic(ROC)curvewascalculatedtoevaluate the diagnostic and prognostic significance of the tested parameters.DatawereexpressedasareaunderROCcurves with95%confidenceintervals(CIs).TheYoudenindex (max-imum level of sensitivity+maximum level of specificity) wasused tofindthe optimal cut-off points.The sensitiv-ity,specificity,positivepredictivevalue(PPV),andnegative predictive value (NPV) were also calculated. The agree-ments of the PCT values between the two PCT devices weredeterminedbyCohen’scoefficient.In allanalyses,
two-tailedp-values<0.05wereregardedasstatistically sig-nificant.
Results
Characteristicsofthestudypopulation
ClinicalsuspicionofCRBSIwasnotedin62children.These subjects did not show an obvious alternative source for infection.Microbiological culture ofurine andchestX-ray werenegative.Thirteenchildrenwithinfectionotherthan CRBSIduringhospitalizationwereexcludedfromthestudy. Oftheremaining49patients,25(51%)wereprovenasnot suffering fromCRBSI (unprovenCRBSI) and24 (49%) were positiveforCRBSI(provenCRBSI).
The demographic and clinical characteristics of the patients are summarized in Table 1. During the study period, 49 patients (34.7% female, n=17; 65.3% male, n=32) from the 240 beds at the Pediatric Unit of Uni-versity Hospital, Ankara, Turkey, were enrolled, with a mean age of 72.8±66.9 months (range: 2---252 months). Nostatisticallysignificantdifferenceswerefoundregarding patients’age(p=0.24)andgender(p=0.14;Table1).The accompanying co-morbidities were as follows: 25 (52%) patients had non-oncologic diagnosis, including chronic diarrhea, cholestasis, renal failure, neurologic diseases requiring continuous total parenteral nutrition, while the remaining 24 (48%) patients had hematologic or onco-logicmalignancies/diseases,includingacutelymphoblastic leukemia,acutemyelogenousleukemia,orcentralnervous systemtumors(e.g.,ependymoma,primitive neuroectoder-maltumor;Table1).
Table1 Patients’demographicsandclinicalcharacteristics.
ProvenCRBSI(n=24) NotprovenCRBSI(n=25) p
Age[month;mean±SD(Min.---Max.)] 67.2±71.7(3.0---252.0) 78.2±63.1(2.0---245.0) 0.24a
Gender 0.14b
Female[n(%)] 11(45.8) 6(24)
Male[n(%)] 13(54.2) 19(76)
Primaryadmissiondiagnosis 0.39b
Hematological[n(%)] 12(50) 15(60)
Nephrological[n(%)] 4(16.7) 1(4.0)
Immunological[n(%)] 2(8.3) 2(8.0)
Gastroenterological[n(%)] 3(12.5) 1(4.0)
Other[n(%)] 3(12.5) 6(24.0)
WBCcount[103/
L;median(IQR)] 5.20(0.9---13.0) 1.7(0.8---5.4) 0.17c
Platelet[103/
L;median(IQR)] 118.0(43.0---237.2) 111.0(22.0---214.5) 0.83c
CRP[mg/dL;median(IQR)] 5.63(1.17---12.45) 2.10(0.73---8.5) 0.33c
PCT-Kryptor[ng/mL;median(IQR)] 1.77(0.30---4.96) 0.28(0.17---0.68) 0.03c,d
PCT-RTA[ng/mL;median(IQR)] 1.76(0.71---3.13) 0.57(0.26---1.00) 0.03c,d
Mortality[n(%)] 2(8.3) 0(0) N/A
WBC, whitebloodcell;CRP,C-reactive protein; PCT,procalcitonin;IQR,interquartile range;CRBSI, catheter-relatedbloodstream infection;N/A,notapplicable;SD,standarddeviation.
a Student’sttest. b Chi-squaredtest. c Mann---Whitneytest.
d Statisticallysignificantdifference.
organisms, which included S. epidermidis (n=1) and S. aureus(n=1).
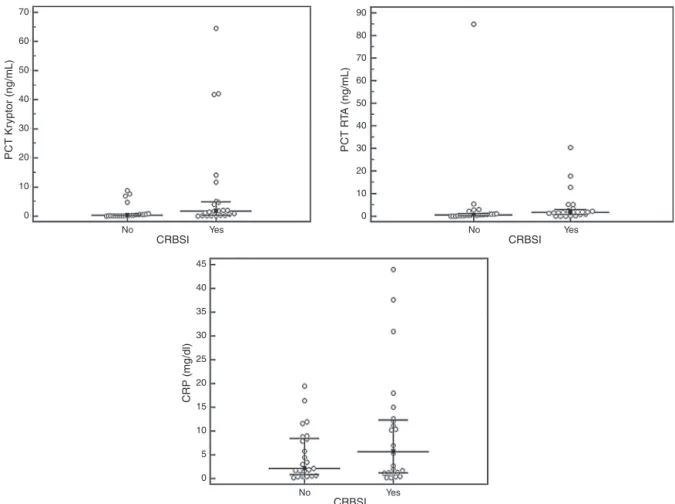
PCT-KryptorandPCT-RTAvaluesweresignificantlyhigher inpatientswithprovenCRBSIwhencomparedwiththosein patientswithunprovenCRBSI(p=0.03andp=0.03, respec-tively).CRBSIpatients did notshow asignificant increase inCRPvalues,ascomparedtonon-CRBSIpatients(p=0.33; Table1).ThedistributionofPCTandCRPvaluesaccordingto thepatientgroupisshowninFig.1.Amongthe24patients with CRBSI, CRP was significantly higher among patients withGram-negativebacterialinfection(12.30[5.65---32.57]) thanin thosewithGram-positivebacterialinfection (2.33 [0.40---9.15], p=0.01). PCT-Kryptor was also significantly higheramongpatientswithGram-negativebacterial infec-tion(4.40 [1.69---19.22]) than inthose withGram-positive bacterialinfections(0.32[0.08---2.10],p=0.02).Amongthe 24 patients withCRBSI, thosewithuncontrolled infection didnotshowsignificantincreasesinPCT-Kryptor,PCT-RTA, and CRP values, when compared with patients with con-trolled infection (p=0.91, 0.48, and 0.14, respectively). The agreement of the PCT values between PCT-Kryptor and PCT-RTA devices was considered as intermediate (:0.548).
The areas under the ROC curves for the diagnosis of CRBSIwere0.684(95%CI,0.526---0.843;p=0.03)forPCT-RTA (bestcutoff,1.18ng/mL)and0.683(95%CI,0.525---0.842; p=0.03)for PCT-Kryptor(bestcutoff, 0.86ng/mL;Fig.2). The areaundertheROC curvesfor the diagnosisof CRBSI was0.581(95%CI,0.417---0.745;p=0.33)forCRP.The sen-sitivity,specificity,PPV,NPV,andaccuracyofPCT-RTAwere 0.71,0.80,0.77,0.74,and0.75,respectively.The sensitiv-ity,specificity,PPV,NPV,andaccuracyofPCT-Kryptorwere 0.66,0.84,0.80,0.72,and0.75,respectively.
Discussion
Current methods for the diagnosis of CRBSIs are time-consuming and rely on culture techniques that require 24---48h to confirm the diagnosis. Therefore, parameters thataccuratelydistinguishCRBSIfromnon-CRBSIatanearly stageareimportant.17Inthepresentstudy,PCTwas
consid-eredagooddiagnosticmarkerwhencomparedwithWBCand CRP.PCTcandistinguishpatientswithCRBSIfrompatients withBSIfromothersources.Additionally,onthedayof clin-icalsuspicionoftheinfection,acutoffpointof0.86ng/mL ofPCT wasshowntodistinguishpatientswithandwithout CRBSI.The specificity ofthe test was0.84 anda positive resultinanypatientmaybeusedasaparametertoremove centrallinesimmediately.TheRTA-PCTassayshowed mod-erate concordance with the established Kryptor method, withanoptimalcutoffof1.18ng/mL.Therefore,this tech-niquecanbeconsideredasausefultoolinvariousmedical settings,although it requires further evaluation in larger studies.
Thepresentfindingsareinagreementwithsomeofthe recentreportsthatassessedthediagnosticvalueofPCTfor earlydetectionofdifferentinfectionsintheintensivecare unit(ICU).16,18,19ThediagnosticvalueofPCTinCRBSIswas
alsoevaluatedinadifferentcohort,andthepresentfindings areconsistentwiththosereports.16,17However,theauthors
inthosereportsdidnotspecificallyevaluateCRBSIin chil-dren,andaproportionoftheirpatientshadsufferedseptic episodes.
Biomarkers of inflammation, such as the WBC count and CRP levels, can also be evaluated to diagnose CRB-SIs, although their specificity is lower.20 Several studies
70 90
80
70
60
50
40
30
20
10
0 60
50
40
30
20
10
No Yes No Yes
No Yes
CRBSI
CRBSI CRBSI
PCT Kr
yptor (ng/mL)
PCT R
T
A (ng/mL)
CRP (mg/dl)
0
45
40
35
30
25
20
15
10
5
0
Figure1 Distributionofprocalcitonin(PCT)andC-reactiveprotein(CRP)accordingtothestudygroups.CRBSI,catheter-related bloodstreaminfection.
of bacterial infections, especially sepsis.14,21---23
Addition-ally,Theodorou etal.16 have reportedthat thediagnostic
accuracy of PCT in patients with CRBSIs is significantly higherwhencomparedwithWBCandCRP.Consistentwith
1.0
0.8
0.6
0.4
0.2
0.0
0.0 0.2 0.4 0.6
PCT_Kryptor PCT_RTA Reference line
1-specificity ROC Curve
Sensitivity
0.8 1.0
Figure2 Receiveroperatingcharacteristiccurvesfor procal-citonin(PCT)andC-reactiveprotein(CRP)forthedetectionof centralvenouscatheter-relatedbloodstreaminfection(CRBSI).
this report, we have not observed significant differences in the CRP levels between patients with and without CRBSI.
Inorderofprevalence,thefourgroupsofmicrobesthat mostcommonly causeCRBSIassociatedwithpercutaneous insertion arecoagulase-negative staphylococci, S. aureus,
Candidaspecies, and entericGram-negative bacilli.1
Con-sistentwiththatreport,1 thedominantcausativeagentof
CRBSIinthepresentstudywascoagulase-negative staphylo-cocci.However,contrarytothepresentfindings,Theodorou et al.16 have reported that Gram-negative bacteria were
predominantlyrecoveredfrompatientswithprovenCRBSI, andtheirpatients werecriticallyillwithprolonged inten-sive care unit stay. Consistent with the findings by Chen etal.,17 thepresent findingsalsounderlinedthatthePCT
concentrationsandCRPlevelswerehigheramongpatients with Gram-negative bacteremia than among those with Gram-positive bacterial infections. Dandona et al.24 and
Linscheid et al.25 have described that serum PCT levels
Several ICU cases can be empirically managed with-out immediate catheter withdrawal. On many occasions, watchfulwaiting is a prudentapproach.26 Some CRBSIsin
hemodynamically stable patients can be handled in situ byusingantibiotics,andfrequently,bacteremiais cleared andthe catheteris sterilized.8,27 In 20of the 24patients
with CRBSI in the present study, bacteremia was cleared and the catheter wassterilized with accurate antimicro-bials,withoutremoval.Thisresultwasespeciallyimportant for children,consideringthe underlyingreasons,including malignancies,inthepresentstudy.However,Gram-negative bacteriawererecoveredfromtwoofthedeceasedchildren. When the patientswere considered ascontrolledand not controlledfor infectioninthepresentstudy,althoughPCT orWBCandCRPwerenotthediscriminatingbiomarkers,the PCTresults mayhaveprovidedtheearliestopportunityto removeacatheterwhileawaitingthebloodcultureresults. Some limitations of the present study should also be noted here. First, the sample population was relatively smaller and heterogeneous regarding the underlying dis-easeconditions.Therefore,thepresent resultsneed tobe confirmedinalargerandmorehomogeneouspool.A con-trol groupwas not designedin this study, but rathertwo groups including proven CRBSI and unproven CRBSI from thepopulationof childrenwithcentrallineswere catego-rizedat theendofthestudyperiodtocreatethedesired groups.Conversely,acontrolpopulationwithbloodstream infectionfrom children without centrallines thatare not catheterrelated mayallow for abetter understanding of other catheter-related blood stream infections. However, thepresentresultsareveryimportant,duetothescarcity ofstudiesonearlyCRBSIdiagnosisinchildren.Inaddition, patients whohadany other infectionwere excluded, and thewithdrawalof potentialconfoundersmayincrease the strengthof thepresentfindingsabout biomarkersas diag-nosticandmonitoringtools.Second,itwasnotpossibleto performthesequentialanalysisoftheinfectiousbiomarkers tounderstandthelongitudinalchangesinthePCT concen-trationandoptimaltimingofthePCTforprognosticvalue, duetofinancialconstraints.
In conclusion, PCT may be a useful rapid diagnos-tic biomarker for suspected CRBSI in children. The new automated rapidquantitativeassay,thePCT-RTA(Kocaeli, Turkey), has some benefits such as small size, easy implantability in a laboratory, and ease of interpretation of the results for the measurement of PCT values. This assay, with a sensitivity and specificity of 71% and 80%, respectively, is an immunochromatographic test for the quantitativedetectionofPCT,andiseasytouseunder emer-gencyconditions.
Funding
ThestudywaspartiallysupportedbyTheCompanyofDialab TibbiUrunlerveOzelSaglik.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgments
The authorswould like tothankSevilay Karahan (Depart-ment of Biostatistics, Hacettepe University Faculty of Medicine,Ankara,Turkey)forthestatisticalanalyses.
References
1.MermelLA,AllonM,BouzaE,CravenDE,FlynnP,O’GradyNP, etal.Clinicalpracticeguidelinesforthediagnosisand manage-mentofintravascularcatheter-relatedinfection:2009Update bytheInfectiousDiseasesSocietyofAmerica.ClinInfectDis. 2009;49:1---45.
2.Romanelli RM, Anchieta LM, Mourão MV, Campos FA, Loy-ola FC, Mourão PH, et al. Risk factors and lethality of laboratory-confirmed bloodstream infection caused by non-skin contaminant pathogens in neonates. J Pediatr (Rio J). 2013;89:189---96.
3.RaadI,HannaH,MakiD.Intravascularcatheter-related infec-tions: advances in diagnosis, prevention, and management. LancetInfectDis.2007;7:645---57.
4.MunsonEL,DiekemaDJ,BeekmannSE,ChapinKC,DoernGV. Detection and treatment of bloodstream infection: labora-toryreportingandantimicrobialmanagement.JClinMicrobiol. 2003;41:495---7.
5.KhatibR,SaeedS,SharmaM,RiedererK,FakihMG,Johnson LB. Impact of initial antibiotic choice and delayed appro-priate treatment on the outcome of Staphylococcus aureus bacteremia.EurJClinMicrobiolInfectDis.2006;25:181---5. 6.PearsonML.Guidelineforpreventionofintravascular
device-relatedinfections.HospitalInfectionControlPracticesAdvisory Committee.InfectControlHospEpidemiol.1996;17:438---73. 7.CapdevilaJA. Catheter-relatedinfection:anupdateon
diag-nosis, treatment, and prevention. Int J Infect Dis. 1998;2: 230---6.
8.BouzaE,AlvaradoN,AlcaláL,PérezMJ,RincónC,Mu˜nozP. Arandomizedand prospectivestudyof3 procedures forthe diagnosis of catheter-related bloodstream infection without catheterwithdrawal.ClinInfectDis.2007;44:820---6.
9.Schuetz P, Mueller B, Trampuz A. Procalcitonin and other biomarkersfortheassessmentofdiseaseseverityandguidance oftreatmentinbacterialinfections.AdvSepsis.2008;6:82---9. 10.KimKE,HanJY.Evaluationoftheclinicalperformance ofan
automatedprocalcitonin assayforthequantitativedetection ofbloodstreaminfection.KoreanJLabMed.2010;30:153---9. 11.SimonL,GauvinF,AmreDK,Saint-LouisP,LacroixJ.Serum
pro-calcitoninandC-reactiveproteinlevelsasmarkersofbacterial infection: asystematicreviewand meta-analysis.ClinInfect Dis.2004;39:206---17.
12.von Lilienfeld-Toal M, Dietrich MP, Glasmacher A, Lehmann L, Breig P, Hahn C, et al. Markers of bacteremia in febrile neutropenicpatientswithhematologicalmalignancies: procal-citoninandIL-6aremorereliablethanC-reactiveprotein.Eur JClinMicrobiolInfectDis.2004;23:539---44.
13.Christ-CrainM,Jaccard-StolzD,BingisserR,GencayMM,Huber PR,TammM,etal.Effectofprocalcitonin-guidedtreatmenton antibioticuseandoutcomeinlowerrespiratorytractinfections: cluster-randomised, single-blindedinterventiontrial. Lancet. 2004;363:600---7.
14.AssicotM,GendrelD,CarsinH,RaymondJ,GuilbaudJ,Bohuon C.Highserumprocalcitoninconcentrationsinpatientswith sep-sisandinfection.Lancet.1993;341:515---8.
16.TheodorouVP,PapaioannouVE,TripsianisGA,PanopoulouMK, ChristophoridisEK,KouliatsisGA,etal.Procalcitoninand pro-calcitoninkineticsfordiagnosisandprognosisofintravascular catheter-related bloodstreaminfectionsin selectedcritically illpatients:aprospectiveobservationalstudy.BMCInfectDis. 2012;12:247.
17.ChenJ,WangY,ShenZ,ZhuZ,SongY,HanR.Earlydiagnostic valueofplasmaPCTandBGassayforCRBSIafterOLT.Transplant Proc.2011;43:1777---9.
18.Charles PE,KusE,AhoS,PrinS,DoiseJM,OlssonNO,etal. Serum procalcitonin for the early recognition of nosocomial infectioninthecriticallyillpatients:apreliminaryreport.BMC InfectDis.2009;9:49.
19.TsangarisI,PlachourasD,KavathaD,GourgoulisGM,TsantesA, KopteridesP,etal.Diagnosticandprognosticvalueof procal-citoninamongfebrilecriticallyillpatientswithprolongedICU stay.BMCInfectDis.2009;9:213.
20.NakajimaA,YazawaJ,SugikiD,MizuguchiM,SagaraH,Fujisiro M,et al.Clinicalutilityofprocalcitonin asa markerof sep-sis:apotentialpredictorofcausativepathogens.InternMed. 2014;53:1497---503.
21.Giamarellos-Bourboulis EJ, Grecka P, Poulakou G, Anargyrou K, Katsilambros N, Giamarellou H. Assessment of procal-citonin as a diagnostic marker of underlying infection in
patients with febrile neutropenia. Clin Infect Dis. 2001;32: 1718---25.
22.PetrikkosGL,ChristofilopoulouSA, TentolourisNK,Charvalos EA,KosmidisCJ,DaikosGL.Valueofmeasuringserum procal-citonin,C-reactiveprotein,andmannanantigenstodistinguish fungalfrombacterialinfections.EurJClinMicrobiolInfectDis. 2005;24:272---5.
23.LoonenAJ,deJagerCP,TosseramsJ,KustersR,HilbinkM,Wever PC,etal.Biomarkersandmolecularanalysistoimprove blood-streaminfectiondiagnosticsinanemergencycareunit.PLOS ONE.2014;9:e87315.
24.DandonaP,NixD,WilsonMF,AljadaA,LoveJ,AssicotM,etal. Procalcitoninincreaseafterendotoxininjectioninnormal sub-jects.JClinEndocrinolMetab.1994;79:1605---8.
25.LinscheidP,SeboekD,NylenES,LangerI,SchlatterM,Becker KL,etal. InvitroandinvivocalcitoninI geneexpression in parenchymalcells:a novelproductofhumanadiposetissue. Endocrinology.2003;144:5578---84.
26.RijndersBJ,PeetermansWE,VerwaestC,WilmerA,Van Wijn-gaerdenE.Watchfulwaitingversusimmediatecatheterremoval inICU patientswithsuspected catheter-related infection: a randomizedtrial.IntensiveCareMed.2004;30:1073---80. 27.BestulMB,VandenbusscheHL.Antibioticlocktechnique:review