REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
PublicaçãoOficialdaSociedadeBrasileiradeAnestesiologiawww.sba.com.br
SCIENTIFIC
ARTICLE
A
randomised
crossover
trial
comparing
the
Airtraq
®
NT,
McGrath
®
MAC
and
Macintosh
laryngoscopes
for
nasotracheal
intubation
of
simulated
easy
and
difficult
airways
in
a
manikin
Manuel
Ángel
Gómez-Ríos
a,∗,
Stephan
Pinegger
a,
María
de
Carrillo
Mantilla
a,
Lucia
Vizcaino
a,
Purísima
Barreto-Calvo
a,
Michael
J.
Paech
b,
David
Gómez-Ríos
a,
Beatriz
López-Calvi˜
no
aaDepartmentofAnaesthesiologyandPerioperativeMedicine,ComplejoHospitalarioUniversitariodeACoru˜na,ACoru˜na,Spain bPharmacology,PharmacyandAnaesthesiologyUnit,SchoolofMedicineandPharmacology,TheUniversityofWesternAustralia,
Perth,Australia
Received25August2014;accepted28October2014
Availableonline12May2015
KEYWORDS
Intubation; Laryngoscopes; Manikin; Randomised controlledtrial
Abstract
Objective: Severaldevicescanaidnasotrachealintubationwhenmanagingdifficultairways.
TheMcGrathMACandAirtraqNTwerecomparedwithaMacintoshlaryngoscopewhenstudying theperformanceofanaesthetistswithdifferentlevelsofexperience,inamanikinmodelof easyordifficultairwayscenarios.
Methods:Sixty-threeanaesthetistswererecruitedintoarandomisedtrialinwhicheach
per-formednasotrachealintubationwithalllaryngoscopes,inbothscenarios.Themainendpoint was intubationtime. Additional endpointsincluded laryngoscopic view,intubation success, numberofoptimisationmanoeuvres,audibledentalclicksandtheforceappliedtotheupper airway.
Results:IntubationtimewassignificantlyshorterusingtheMcGrathMACinbothscenariosand
usingtheAirtraqinthedifficultscenario,whencompared withtheMacintosh laryngoscope. Both devicesgave moreCormack andLehanegrade1or2views thantheMacintosh inthe difficultscenario(p<0.001).TheMcGrathMAChadthebestfirst-attemptsuccessrate(98.4% vs.96.8%and95.8%,p<0.001for theAirtraqNTandMacintoshlaryngoscopesrespectively). Thenumberofoptimisationmanoeuvres,audibledentalclicksandsubjectiveassessmentofthe degreeofforceappliedweresignificantlylowerforindirectlaryngoscopesversustheMacintosh laryngoscope(p<0.001).
∗Correspondingauthor.
E-mail:[email protected](M.Á.Gómez-Ríos). http://dx.doi.org/10.1016/j.bjane.2014.10.009
Conclusion:In a manikin, the Airtraqand the McGrath laryngoscopes appeared superior to theMacintoshlaryngoscopewhendealingwithsimulatedairwayscenarios.Bothdeviceswere associatedwithbetterviews,intubationtimesandratesofsuccess,especiallyinasimulated ‘‘difficult airway’’.Overallsatisfactionwas highestwiththe McGrath laryngoscope.Similar clinicalstudiesareneeded.
©2015SociedadeBrasileiradeAnestesiologia.PublishedbyElsevier EditoraLtda.Allrights reserved.
PALAVRAS-CHAVE
Intubac¸ão; Laringoscópios; Manequim;
Estudorandômicoe controlado
EstudocruzadoerandômicocomparandooslaringoscópiosAirtraq® NT,McGrath®
MACeMacintoshparaintubac¸ãonasotraquealemsimulac¸ãodeviaaéreafácile difícilemmanequim
Resumo
Objetivo:Váriosdispositivospodemajudaraintubac¸ãonasotraquealnomanejodeviaaérea
difícil.OslaringoscópiosMcGrathMACeAirtraqNTforamcomparadoscomumlaringoscópio Macintoshemestudododesempenhodeanestesistascomdiferentesníveisdeexperiência,em manequimcomcenáriodeviaaéreafáciloudifícil.
Métodos: Sessentaetrêsanestesistasforamrecrutadospara umestudorandômico, noqual
cadaumrealizouintubac¸ãonasotraquealcomtodososlaringoscópios,emambososcenários.O desfechoprimáriofoiotempodeintubac¸ão.Desfechosadicionaisincluíramvistalaringoscópica, sucesso naintubac¸ão,númerode manobrasdeotimizac¸ão,cliquesdentais audíveise forc¸a aplicadanasviasaéreassuperiores.
Resultados: Otempo deintubac¸ão foisignificativamentemenor comousodolaringoscópio
McGrathMACemambososcenáriosecomousodoAirtraqnocenáriodifícil,emcomparac¸ão comolaringoscópioMacintosh.Ambososdispositivosobtiverammaisgrau1ou2deCormack eLehane paravisualizac¸ãoqueo Macintoshem cenário difícil(p<0,001).OMcGrath MAC teve amelhor taxa desucesso na primeira tentativa (98,4% vs.96,8% e 95,8%, p <0,001, paraoslaringoscópiosAirtraqNTeMacintosh,respectivamente).Onúmerodemanobrasde otimizac¸ão,oscliquesdentaisaudíveiseaavaliac¸ãosubjetivadograudeforc¸aaplicadaforam significativamentemenoresparaoslaringoscópiosindiretosversusolaringoscópioMacintosh(p <0,001).
Conclusão:Em ummanequim, oslaringoscópiosAirtraqe McGrathpareceram superiores ao
laringoscópioMacintoshparalidarcomcenáriosdasviasaéreassimuladas.Ambososdispositivos foramassociadosamelhoresvisibilidades,temposdeintubac¸ãoetaxasdesucesso, especial-menteemsimulac¸ãode‘‘viaaéreadifícil’’.Asatisfac¸ãogeralfoimaiorcomolaringoscópio McGrath.Estudosclínicossimilaressãonecessários.
©2015SociedadeBrasileiradeAnestesiologia.PublicadoporElsevierEditoraLtda.Todosos direitosreservados.
Introduction
Airwaymanagementfororal andmaxillofacialsurgerycan beamajorchallenge.Thehighincidenceofdifficult intu-bationcomparedtowithinthegeneralpopulationisdueto congenitalvariationsorpathologyoftheoralandtheupper airwayanatomysecondarytoinfection,tumour,surgeryor radiotherapy.1,2 Nasotracheal intubation (NTI)is generally
needed to allow unrestricted surgical access and is usu-allyperformed using a Macintoshlaryngoscope and Magill forceps.Thisnecessitatesalignmentofthe oropharyngeal-laryngealaxesfor visualisation ofthe glottisandtracheal intubation3; and may fail or be poorly tolerated by an
awakepatientwitha‘difficultairway’,resultingin morbid-ityandevenmortality.4Useofafibreopticbronchoscopehas
beenrecommendedinthisscenario,butthisdeviceisoften unavailableandthetechniqueislessfamiliarandrequires additionalskillandtrainingtobeusedeffectively,5,6making
alternativesnecessary.
Advancesinopticandvideotechnologyhaveledto pro-ductionofnewintubationdevicessuchastheAirtraq® NT (ProdolMeditecS.A.,Vizcaya,Spain)andtheMcGrath®MAC (AircraftMedicalLtd,Edinburgh,UK).Adefining character-istic of these devices is that the glottic view is achieved indirectlyinsteadofbydirectline-of-sight,thusimproving theviewandreducingintubationtimecomparedwithdirect laryngoscopes.7Theefficacyandsafetyofthesedevicesfor
NTIhavereceivedlittleattention.
TrialcomparingtheAirtraq NT,McGrath MACandMacintoshlaryngoscopes 291
whenusedbyanaesthetistsofdifferentlevelsofexperience in direct laryngoscopy. The anaesthetists were unfamiliar withthese newdevices andparticipated in a randomised controlledmanikin study involving management of both a normal airwayand adifficult airway. We chose amanikin studybecausetheMcGrathMACisanewdevice,the perfor-manceofwhichhasnotbeenexaminedinatrialpublished inthepeer-reviewedliterature.
We hypothesisedthatthetimetocorrectendotracheal tube (ETT) placementthrough the nose would beshorter withthe Airtraq NT andMcGrath devices, comparedwith the Macintoshlaryngoscope. The primaryaim of the trial wastoassessthetimetosuccessfulintubationwhenusing thesedifferentdevices.
Methods
TheClinicalResearchEthicsCommitteeofGaliciaapproved thetrial (Ref: 2010/486),which adhered tothe standards of the International Conference on Harmonization Good Clinical Practice. The trial (NCT01311284) wasregistered at ClinicalTrials.gov before inclusion of participants. The participantswereeligibleiftheyweremembersof Depart-mentofAnaesthesiologyofUniversityHospitalComplexof ACoru˜na. Participation wasvoluntaryandall participants gavewritteninformedconsent.
Trialprotocol
A randomisedcrossover trial wasperformed in the Train-ingTechnologyCenterofUniversityHospital ComplexofA Coru˜na.Sixty-threeanaesthetistswererecruited, compris-ing21residents(minimalexposuretoNTI,‘residentgroup’), 21consultants(anaesthetistsfamiliarwithaNTItechnique but who only performed it occasionally, ‘trained group’) and 21 expert consultants (whoperformed the technique regularly, ‘expert group’). Standardised instructions were providedabout each device,includinga demonstrationof theintubationmethodandverbalinformation. Theuseof optimisation manoeuvres tofacilitate intubation, such as readjustmentofheadposition,applicationofexternal laryn-gealforce,useofMagillforceps,useofastyletortheFrova airwayintubationcatheter(CookCriticalCare,Letchworth, United Kingdom), and the use of an assistant, were also demonstrated.Before thestudy,each anaesthetisttested thedifferentdevicesuntiltheyachievedsuccessful intuba-tionofthemanikin.
TheAirtraq®NTopticallaryngoscope,theMcGrath®MAC videolaryngoscopeandtheMacintoshlaryngoscope,size3, weretestedinthistrial(Fig.1).
All intubations were performed with a Portex Polar Preformed trachealtube (Smith Medical Internacional Ltd Hythe,Kent, UK;internaldiameter7.0mm) onastandard trainingmanikin(AirSimAdvance, Trucorp,Belfast, North-ernIreland). Eachsubjectperformed aNTI innormal and difficultairwaysusingthethreedevices.Thedifficultairway wasobtainedbytheinflationofthetongueofthemanikin with25mLofair,simulatinglimitedaccesstothe oropharyn-gealcavity.
Theorderofselectionofthedeviceandtheairway sce-nario at each attempt were randomised, based on a list
Figure1 TheAirtraq®NTopticallaryngoscope,theMacintosh
laryngoscopeandthenewMcGrath®MACVideolaryngoscope.
createdusingtheEpidatprogram,version3.1.Inaddition, theparticipants were blindedto level ofdifficulty of the airwayuntiltheirattempttointubation.
Atotalofthreeintubationattemptswereallowedwith each laryngoscope in each scenario. An unsuccessful NTI, removalofthedevicefromtheoralcavityduetoapoorview orNTItakingmorethan120swereconsideredafailed intu-bation.ThecorrectlocationoftheETTwascorroboratedby aninvestigatoratallintubationattempts.
The mainendpoint wasthetimetakentoachieve suc-cessfulNTI.Additionalendpointsincludedtimetoandgrade ofglotticview(CormackandLehanegrades1---4),incidence ofsuccessfulNTI,numberofattempts,numberof optimisa-tionmanoeuvresduringNTI,numberofaudibledentalclicks duetotouchingtheteeth,severityofforceappliedtothe upperairwayandtimetoventilationofthelungs.
Timeintervalsweremeasuredbythesameinvestigator, usinga stopwatch,for allintubations.Timingbeganwhen theblade of the intubation device was inserted between theteeth;interimtimes werewhen thevocal cordswere visualised,whentheETTwasinsertedintothetrachea;and timingfinishedatthefirstventilationofthelungs.Timeto viewthe glottiswaswhen theinvestigatorsawtheglottis onthe viewingdevice for theMcGrathMACandbyverbal notificationfromtheparticipantfortheAirtraqNTand Mac-intoshlaryngoscopes.The timetotrachealintubation was definedas the time frominsertion of the blade between theteeth untilthe ETT wasdeemed tobe correctly pos-itioned.Thetimetoinflationofthelungswasdefinedasthe timefrominsertionofthebladebetweentheteethtothe timewhentheETTwasconnectedtothemanualventilation device(LaerdalMedical,Stavanger,Norway)andsuccessful ventilationwasverifiedbytheinvestigator.
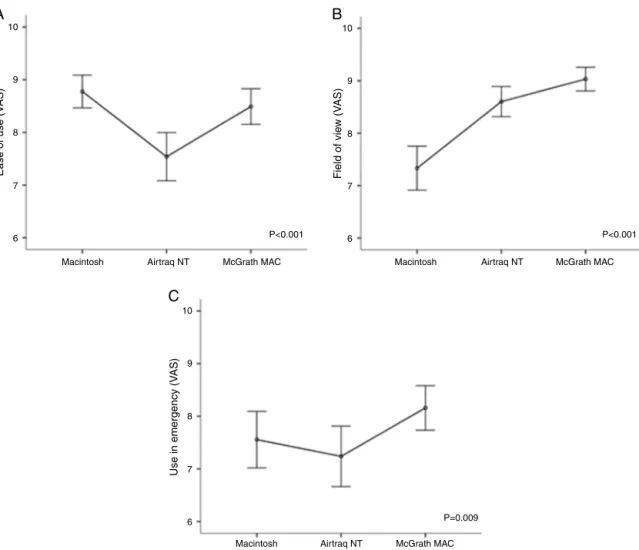
Thecountofaudibledentalclicksoundsofthemanikin (0,1,2or>2)wasmadeasanassessmentofpotential den-taltrauma.Aninvestigatorsubjectivelyassessedthedegree offorce(absent,slight,moderateorsevere)exertedduring eachintubation.Oncethestudywascompleted,each par-ticipantevaluatedtheclinicalutility ofeachlaryngoscope usingavisualanaloguescale(VAS)from0(extremelypoor) to10 (extremelyhigh) forcriteriaof easeof use,fieldof viewandpreferenceinanemergency.
Statisticalanalysis
Table1 Characteristicsandintubationexperienceofparticipants.Numericalvaluesrepresentmedian.
Residents Trained Experts
Number 21 21 21
Male:femaleratio 9:12 5:16 6:15
Experience(yr) 2.5±1.2 16.7±7.1 11.6±5.5
NumberofpreviousMacintoshNTI 2 15 All>50
NumberofpreviousAirtraq®NTNTI 0 0 0
NumberofpreviousMcGrath®MACNTI 0 0 0
Fromexperienceweconsideredthatthetimeexpectedfor NTIinamanikinwouldbe12---70s,dependingonthe oper-ator’s experience and the difficulty of the scenario. We reasoned that a reduction to 7s with one of the scopes was meaningful in a simulator study. Sixty-three partici-pantswouldprovide at least an 80%power todetect this difference, at a significance level of 0.05. The statistical analysiswasconductedusingSPSS20.0(SPSSInc.,Chicago, IL,USA).Thedatawereexpressedasmean±SDfor contin-uousordiscretevariablesandasfrequencyandpercentage forcategoricalvariables.Thenormaldistributionof quanti-tativevariableswasevaluatedbytheKolmogorov---Smirnov test.Thebetween-groupcomparisonswereperformedusing theMann---WhitneyU-testfornon-parametricvariablesand the independent Student t-test for parametric variables. The analysis of variance by Friedman and Kruskal---Wallis multiple-comparison tests were applied for comparison betweengroups. The Wilcoxontest wasusedforpost hoc comparisons.p-Valuesof<0.05wereconsideredstatistically significant.
Results
Participants’characteristics
Sixty-three anaesthesia providers --- 21 residents, 21 con-sultants and 21 experts --- were recruited (20 males, 43 females;meanage37years)andtherewerenodropouts.No participanthadpreviousexperiencewitheitherofthe indi-rectlaryngoscopestested.Theaverageexperienceindirect laryngoscopywasameanof10.2(SD7.8)years. Character-isticsoftheparticipantsarepresentedinTable1.
Easyairwayscenario
Thevaluesofthedifferentvariablesforbothscenariosare showninTable2.There wassignificant differencein time tointubation between the McGrath MAC, Airtraq NT and theMacintosh(p=0.002).Therewasnodifferencebetween theMacintoshandtheAirtraqNT,butintubationtimewas significantlyshorterwiththeMcGrath MACcomparedwith theAirtraqNT(p=0.001)andtheMacintoshlaryngoscopes (p=0.016).
Theresultsfortimetoviewthecordsandtimeto intu-bateinbothscenariosaregraphicallyrepresented(Fig.2). Therewerestatisticallysignificantdifferencesbetween the devices for several secondary endpoints (p<0.001). Thesewerethenumberofaudibledentalclicksounds,the
severityofforceappliedtotheupperairway,theCormack andLehanegradeofviewandthenumberofoptimisation manoeuvrestoaidNTI;thelatterwerereadjustmentofhead position(p<0.001),applicationofexternallaryngealforce (p=0.011)anduseofMagillforceps(p<0.001).These end-pointsweresignificantlyreducedinboththeMcGrathMAC andAirtraqNTgroupscomparedwiththeMacintoshgroup.A significantdifferencebetweendeviceswasobservedforthe timetakenfromvisualisationofthevocalcordstocorrect placementoftheETT(Fig.3A).
Therewerenosignificantdifferencesbetweengroupsfor the timetaken to viewthe vocal cords, the incidence of successfulETTplacementinthetracheaorthenumberof intubationattempts.
Difficultairwayscenario
A significant difference between the three intubation devices(p<0.001)wasdetectedfortheendpointsoftimeto viewthevocalcordsandintubationtime(Fig.2).However, there wasno significant differencebetween the McGrath MACandtheAirtraqNT(p=0.082).Nevertheless,thetime with both devices was significantly shorter than with the Macintosh(p=0.001andp<0.001respectively)(Fig.2).
The post hocanalysis for thetime tointubate demon-strated asignificantdifferencebetween theMcGrathMAC and the Airtraq NT when compared with the Macin-tosh (p<0.001) but nosignificant differencebetween the McGrathMACandtheAirtraqNT(p=0.125).
There wasa significant difference in time required to intubate associated with operator experience when using theMacintoshlaryngoscope(p=0.004).
TrialcomparingtheAirtraq NT,McGrath MACandMacintoshlaryngoscopes 293
Table2 Intubationsuccessratesandvariables.Valuesaremean±SDornumber(percentage)orpercentage.
Airwayscenario Easy Difficult
ML ANT McG ML ANT McG
SuccessNTI(n) 63(100) 61(96.8) 63(100) 58(92) 59(93.6) 62(98.4)
Times
Viewglottis(s) 15.1±7.5 15.4±10.0 13.1±6.5 30.6±12.0 22.9±14.8 18.1±9.7 Intubation(s) 31.3±14.2 34.7±19.2 25.4±14.4 51.7±17.2 41.0±21.7 37.4±21.8 Ventilation(s) 45.6±17.3 45.8±20.3 37.4±16.4 71.4±62.9 53.6±24.3 50.7±22.4
Manoeuvres
Head 76.2 38.1 49.2 90.3 51.6 53.2
BURP 19.0 3.2 9.5 61.3 8.1 14.5
Forceps 60.3 12.7 19.0 79.0 16.1 7.7
Stylet 0 0 3.2 1.6 3.2 1.6
Assistant 7.9 1.6 7.9 32.3 4.8 11.3
Dentalclicks(%)
0 44.4 73.0 76.2 9.5 61.9 60.3
1 38.1 19.0 20.6 46.0 33.3 38.1
2 14.3 7.9 3.2 30.2 1.6 1.6
>2 3.2 0 0 12.7 3.2 0
Pressureexertedonairway(%)
None 9.5 36.5 52.4 0 23.8 15.9
Minor 41.3 57.1 44.4 1.6 68.3 60.3
Moderate 46.0 6.3 3.2 17.5 4.8 22.2
Severe 3.2 0 0 81.0 3.2 1.6
Gradeofglotticview(%)
1 68.3 96.8 93.7 0 87.1 87.1
2 31.7 3.2 6.3 19.4 12.9 11.3
3 0 0 0 77.4 0 1.6
4 0 0 0 3.2 0 0
MLT=Macintosh,ANT=AirtraqNT,McG=McGrathMAC.NTI=nasotrachealintubation.BURP=backwards,upwards,right,pressure.Glottic viewbasedonCormackandLehaneclassification.
appearedtorequirelessforceontheupperairwaycompared withuseoftheMacintoshlaryngoscope(p<0.001).
In thedifficult airway scenario,both theMcGrath MAC andtheAirtraqNTweremorelikelytoprovideagrade1or2 viewthantheMacintosh(p<0.001),withalmostnoGrade3 or4views.Theposthocanalysisdemonstratedsignificantly betterviewsfromtheMcGrathMACthanfromtheAirtraqNT (p=0.013).Therewerenosignificantdifferencesbetween devicesfor thetimetakenfromvisualisation of thevocal cordstocorrectplacementoftheETT(Fig.3B).Therewere severalintubationfailureswiththeMacintosh(five)andthe AirtraqNT(four)andonewiththeMcGrathMAC.
The VAS score for ease of use of the Macintosh laryn-goscopewassignificantlyhigherthantheVASscoreof the AirtraqNTandMcGrathMACvideolaryngoscopes(p<0.001). Participantsratedtheindirectlaryngoscopeswell,astheir hypotheticallypreferredlaryngoscopeinanemergency set-ting,butposthocanalysisshowednosignificantdifferences betweengroups(Fig.4).
Discussion
Althoughmanystudieshavecomparedindirectversus con-ventionallaryngoscopy,8---10nonehavecomparedtheAirtraq
and McGrath MAC with the Macintosh laryngoscope for NTI. This study in a simulated manikin model, evaluat-ingtheperformanceofpractitionersexperiencedindirect laryngoscopybutinexperiencedwiththeseindirect laryngo-scopes,thetimetoNTI wassignificantlyshorterusingthe McGrathMACinthe easyanddifficult airwaysettingsand theAirtraqinthedifficultscenario.Indirectlaryngoscopes alsoofferedsuperiorviewsoftheglottisbeforeadditional optimisationstrategies.Secondaryendpointssuggestedthat theymight also reduce the risk of dentalinjury and high upperairwayforces.Theseadvantages weremostevident inthe‘limitedoropharyngealcavity’ordifficultscenario.
ThereducedintubationtimefoundintheMcGrathMAC groupcorroborates a preliminary clinical study that com-paredtheMacintoshwiththeMcGrathseries5.11 However,
theresultsobtainedinpreviousstudiesfor oralintubation withthe McGrath series 5 contrast withour findings.12---14
Thisdifferencemay reflectthe factthat thecurrent ver-sionoftheMcGrathincorporatesaMacintoshblade,15which
might have modified user characteristics compared with otherdeviceswithblades witha morepronounced curva-ture.
Macintosh Airtraq NT McGrath MAC P=0.300 0
20 40 60 80 100
A
Time to vie
w the v
ocal cords (s)
Macintosh Airtraq NT McGrath MAC P=0.002 0
20 40 60 80 100
Intubation time (s)
Intubation time (s)
Macintosh Airtraq NT McGrath MAC Macintosh Airtraq NT McGrath MAC
P<0.001 0 P<0.001
20 40 60 80 100
0 20 40 60 80 100
Time to vie
w the v
ocal cords (s)
B
C
D
Figure2 Boxplotsdepictingthetimetoviewthevocalcordsandthetimetointubateineasy(AandB)anddifficult(CandD) airwaysimulations.
were longer and more attempts were required to intu-batewhen comparedwiththeMcGrath MAC. By contrast, thespeedoforalintubationwiththestandardAirtraqwas fasterthanother devices.16,17 Thismaybebecauseofthe
side-channel that guides the ETT through the glottis.7,18
TheAirtraqNTlacksan ETTchannel,preservingthe angu-lated blade, but consequently the view with the Airtraq
NT does not necessarily correspond with the path fol-lowed by the ETT, making it more difficult to pass the tracheal tube. Extra manoeuvres may be necessary and thefourintubationfailuresweobservedoccurredbecause participants had difficulty placing the ETT into the glot-tis. This is considered a general limitation of indirect laryngoscopes.19
Macintosh Airtraq NT McGrath MaC
P=0.018 P=0.510
McGrath MaC Macintosh Airtraq NT
–20 0 20 40 60 80 100
–20 0 20 40 60 80 100
A
B
∆
t (S) ∆
t (S)
TrialcomparingtheAirtraq NT,McGrath MACandMacintoshlaryngoscopes 295
A
B
C
10
9
8
7
6
10
9
8
7
6 10
9
8
7
6
Airtraq NT McGrath MAC Macintosh
Airtraq NT McGrath MAC Macintosh
Airtraq NT McGrath MAC Macintosh
Field of vie
w (V
AS)
Ease of use (V
AS)
Use in emergency (V
AS)
P<0.001
P=0.009 P<0.001
Figure4 Graphsrepresentingthevisualanaloguescale(VAS)scoreofparticipants’subjectiveevaluationsofthedevices.
DuringNTI,incontrastwithoralintubation,the intuba-tion timedepends less upon the time required toexpose theglottisandmoreonthetimeneededtoadvancetheETT fromthenasopharynxtowardstheglottis.20Thetimetaken
fromvisualisationofthevocalcordstoinsertionoftheETT was shorter withthe McGrath MAC than withthe Airtraq NTandMacintoshlaryngoscopeinbothscenarios,probably becausefeweroptimisationmanoeuvreswererequired.
AirtraqNTandMcGrathMACappearedtoreduceforces and the risk of dental trauma compared with the Macin-tosh,whichisconsistentwithpreviousstudiesusingindirect laryngoscopes.21---24Inconventionallaryngoscopy,significant
forceisrequiredtoaligntheglottis,pharyngeal,and laryn-gealaxes,25 butthisisnotrequiredwhenusinganindirect
laryngoscope.7,19Theliteraturedoesnotdescribedentalor
upperairwayinjuryduetothesedevices.
FamiliaritywiththeMacintoshlaryngoscope forroutine trachealintubationcouldhaveintroducedbiasinthisstudy. However,therewasnorelationshipbetweentheexperience of the operator and the time taken for NTI with indirect laryngoscopes.This corroborates previous trialsindicating thatnovelopticalandvideolaryngoscopesareeasytouse andhaveasimilarlearningcurveforbothresidentandstaff anaesthetists.14,18,26
The resultsof thisstudyindicatethatindirect laryngo-scopesmaybeadvantageousinthemanagementofdifficult
airway secondary to reduced oropharyngeal space (pres-enceoftumour,infectionormuscleflapafterreconstructive surgery).Few publications have addressed this topic,27---29
althoughtworecentclinicalstudiessuggestthattheAirtraq NTmaybemoreusefulthantheMacintosh.20,30 Thisstudy
differsinseveralpointsandprovidesadditionalinformation. Ourstudyhas severallimitations. Themajorlimitation is that we used a manikin instead of patients. An airway simulatordoesnotreproduceclinicalintubatingconditions exactly,withreal-lifedifferencesincludingtheappearance ofhumidifiedgas,secretions or blood,which addto diffi-culty. However manikin studies allow well-controlled and reproducible conditions, especially for untested medical devices.This avoidsharmtopatientsand maintainsstrict standardisationof study conditionscompared tothe vari-abilityofdifferingpatientairwayanatomy.Inaddition,we onlyusedone approachtoadifficult airway scenarioand other scenarios may resultin alternative performance by thedevice.Nevertheless,recentclinicalstudiessupportthe mainfindingsin thissimulationmodel.11,20,30 Inastudy of
havebeen underpowered.The ‘‘airwayforce’’estimation wasasubjectiveopinionthatdidnotinvolveameasurement systemandmaynotbevalidwithrespectto reproducibil-ity.Finally,thereareanumberofothervideolaryngoscopes available,soour studyonly contributestogeneral under-standinginthisarea.
In conclusion, in this manikin study, the Airtraq and the McGrath laryngoscopes appeared more useful than the conventional Macintoshlaryngoscope undersimulated conditions.Bothdeviceswereassociatedwithshorter intu-bationtimesandfewerattempts andgreater satisfaction, possiblybecauseofthebetterviewwhichappearedtoresult fromfeweradditionalmanoeuvrestoimprovetheview.The clinicalrelevanceisunknownuntilsimilarcomparative clin-icalstudieshave beenconductedtoestablishthebenefits andthedisadvantagesofthesedevicesduringnasotracheal intubation.
Funding
Thisworkwassupportedbydepartmentalandinstitutional fundsonly.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgements
WethankallthemembersoftheDepartmentof Anaesthe-sia and Critical Care of University Hospital Complex of A Coru˜nafortheirparticipationinthestudy,andthemember ofTrainingTechnology Centerfortheir pricelesslogistical support.
References
1.AyusoMA,SalaX,LuisM,etal.Predictingdifficultorotracheal intubationinpharyngo-laryngealdisease:preliminaryresultsof acompositeindex.CanJAnaesth.2003;50:81---5.
2.Mayhew JF. Airway management for oral and maxillofacial surgery.IntAnesthesiolClin.2003;41:57---65.
3.HallCE,ShuttLE.Nasotrachealintubationforheadandneck surgery.Anaesthesia.2003;58:249---56.
4.Gómez-Ríos MA, Serradilla LN. Use of the Airtraq® optical
laryngoscope for nasotracheal intubation in predicted dif-ficult airway management in oral surgery. Can J Anaesth. 2010;57:1136---7.
5.KristensenMS,MøllerJ.Airwaymanagementbehaviour, expe-rience and knowledge among Danish anaesthesiologists ---room for improvement. Acta Anaesthesiol Scand. 2001;45: 1181---5.
6.MasonRA. Learningfibreopticintubation:fundamental prob-lems.Anaesthesia.1992;47:729---31.
7.Niforopoulou P, Pantazopoulos I, Demestiha T, et al. Video-laryngoscopes in the adult airway management: a topical review of the literature. Acta Anaesthesiol Scand. 2010;54: 1050---61.
8.MaassenR,LeeR,HermansB,etal.Acomparisonofthree vide-olaryngoscopes:theMacintoshlaryngoscopebladereduces,but doesnotreplace,routinestyletuseforintubationinmorbidly obesepatients.AnesthAnalg.2009;109:1560---5.
9.EnomotoY,AsaiT,AraiT,etal.Pentax-AWS,anew videolaryn-goscope,ismoreeffectivethantheMacintoshlaryngoscopefor trachealintubationinpatientswithrestrictedneckmovements: a randomized comparative study. Br J Anaesth. 2008;100: 544---8.
10.McElwainJ,MalikMA,HarteBH,etal.ComparisonoftheC-MAC videolaryngoscopewiththeMacintoshGlidescope,andAirtraq laryngoscopes ineasyand difficultlaryngoscopy scenarios in manikins.Anaesthesia.2010;65:483---9.
11.BamgbadeOA,OnaolapoMH,ZuokumorPA.Nasotracheal intu-bation withthe McGrathvideolaryngoscope in patientswith difficultairway.EurJAnaesthesiol.2011;28:673---4.
12.NgI,HillAL, WilliamsDL,etal.Randomizedcontrolledtrial comparing the McGrath videolaryngoscope with the C-MAC videolaryngoscopeinintubatingadultpatientswithpotential difficultairways.BrJAnaesth.2012;109:439---43.
13.RayDC,BillingtonC,KearnsPK,etal.AcomparisonofMcGrath andMacintoshlaryngoscopesinnoviceusers:amanikinstudy. Anaesthesia.2009;64:1207---10.
14.Savoldelli GL, Schiffer E, Abegg C, et al. Comparison of the Glidescope, the McGrath, the Airtraq and the Macin-toshlaryngoscopesinsimulateddifficultairways*.Anaesthesia. 2008;63:1358---64.
15.HyugaS,SekiguchiT,IshidaT,etal.Successfultracheal intuba-tionwiththeMcGrath(®)MACvideolaryngoscopeafterfailure
withthePentax-AWSTMinapatientwithcervicalspine
immo-bilization.CanJAnaesth.2012;59:1154---5.
16.Lu Y, Jiang H, Zhu YS. Airtraq laryngoscope versus con-ventional Macintosh laryngoscope: a systematic review and meta-analysis.Anaesthesia.2011;66:1160---7.
17.McElwain J,LaffeyJG. Comparison oftheC-MAC® Airtraq®,
and Macintoshlaryngoscopes in patientsundergoingtracheal intubation withcervical spineimmobilization. Br J Anaesth. 2011;107:258---64.
18.Savoldelli GL,SchifferE,Abegg C,et al. Learningcurves of theGlidescope,theMcGrathandtheAirtraqlaryngoscopes:a manikinstudy.EurJAnaesthesiol.2009;26:554---8.
19.Pott LM, Murray WB. Review of video laryngoscopy and rigid fiberoptic laryngoscopy. Curr Opin Anaesthesiol. 2008;21:750---8.
20.StMontG,BieslerI,PförtnerR,etal.Easyanddifficultnasal intubation---arandomisedcomparisonofMacintoshvsAirtraq®
laryngoscopes.Anaesthesia.2012;67:132---8.
21.Malik MA, Hassett P, Carney J, et al. A comparison of the Glidescope Pentax AWS, and Macintosh laryngoscopes when used bynovice personnel: a manikin study. Can J Anaesth. 2009;56:802---11.
22.LiuL, Tanigawa K, Kusunoki S,et al. Tracheal intubation of a difficultairway using Airway ScopeAirtraq, and Macintosh laryngoscope:a comparativemanikin studyofinexperienced personnel.AnesthAnalg.2010;110:1049---55.
23.CarassitiM,ZanzonicoR,CecchiniS,etal.Forceandpressure distributionusingMacintosh andGlideScope laryngoscopes in normal and difficultairways:a manikin study.Br JAnaesth. 2012;108:146---51.
24.Maharaj CH, Higgins BD, Harte BH, et al. Evaluation of intubation using the Airtraq or Macintosh laryngoscope by anaesthetistsineasyandsimulateddifficultlaryngoscopy---a manikinstudy.Anaesthesia.2006;61:469---77.
25.El-Orbany M, Woehlck H, Salem MR. Head and neck position for direct laryngoscopy. Anesth Analg. 2011;113: 103---9.
26.Maharaj CH, Costello JF, Higgins BD, et al. Learning and performanceoftrachealintubationbynovicepersonnel:a com-parisonoftheAirtraqandMacintoshlaryngoscope.Anaesthesia. 2006;61:671---7.
TrialcomparingtheAirtraq NT,McGrath MACandMacintoshlaryngoscopes 297
Videolaryngoscope,the Boedeker Bougieendotracheal intro-ducer,andtheBoedekercurvedforceps.StudHealthTechnol Inform.2012;173:310---2.
28.Jones PM, Armstrong KP, Armstrong PM, et al. A com-parison of glidescope videolaryngoscopy to direct laryn-goscopyfor nasotrachealintubation.AnesthAnalg.2008;107: 144---8.
29.SuzukiA, OnoderaY, MitamuraSM,etal. Comparisonofthe Pentax-AWSAirwayScopewiththeMacintoshlaryngoscopefor nasotracheal intubation:a randomized, prospective study.J ClinAnesth.2012;24:561---5.