www.jped.com.br
ORIGINAL
ARTICLE
Effects
of
a
psychological
intervention
on
the
quality
of
life
of
obese
adolescents
under
a
multidisciplinary
treatment
夽
Camila
R.M.
Freitas
a,
Thrudur
Gunnarsdottir
b,
Yara
L.
Fidelix
a,
Thiago
R.S.
Tenório
a,c,
Mara
C.
Lofrano-Prado
d,
James
O.
Hill
e,
Wagner
L.
Prado
f,∗aUniversidadedePernambuco,ProgramadePós-Graduac¸ãoemEducac¸ãodeFísica,Recife,PE,Brazil bUniversityofAkureyri,Akureyri,Iceland
cInstitutoFederaldeEducac¸ão,CiênciaeTecnologiadoSertãoPernambucano,SerraTalhada,PE,Brazil dUniversidadedeSãoPaulo,InstitutodePsicologia,SãoPaulo,SP,Brazil
eUniversityofColorado,AnschutzCenterforHealth&Wellness,Denver,UnitedStates
fUniversidadeFederaldeSãoPaulo(UNIFESP),DepartamentodeCiênciasdoMovimentoHumano,Santos,SP,Brazil
Received27January2016;accepted24May2016 Availableonline4November2016
KEYWORDS
Multidisciplinary intervention; Obeseadolescents; Psychological counseling
Abstract
Objective: Toinvestigatetheeffectsofmultidisciplinarytreatmentwithandwithout psycho-logicalcounselingonobeseadolescents’self-reportedqualityoflife.
Methods: Seventy-six obese adolescents (15.87±1.53 y) were allocated into psychological counseling group (PCG; n=36) or control group (CG; n=40) for 12 weeks.All participants receivedthesamesupervisedexercisetraining,nutritionalandclinicalcounseling.Participants inPCGalsoreceivedpsychologicalcounseling.QOLwasmeasuredbeforeandafter12weeks ofinterventionbyGenericQuestionnairefortheEvaluationofQualityofLife(SF-36).
Results: ThedropoutratewashigherinGC(22.5%)whencomparedwithPCG(0.0%)(p<0.001). After12weeks,participantsfromPCGpresentslowerbodyweight,relativefatmassandhigher freefatmass(p<0.001forall)comparedtoGC.QOLimprovedamongadolescentsfromboth groups(p<0.05),however,abetterQOLwasreportedfromthoseadolescentsenrolledinPCG.
夽
Pleasecitethisarticleas:FreitasCR,GunnarsdottirT,FidelixYL,TenórioTR,Lofrano-PradoMC,HillJO,etal.Effectsofapsychological interventiononthequalityoflifeofobeseadolescentsunderamultidisciplinarytreatment.JPediatr(RioJ).2017;93:185---91.
∗Correspondingauthor.
E-mail:[email protected](W.L.Prado).
http://dx.doi.org/10.1016/j.jped.2016.05.009
Conclusion: Theinclusionofapsychologicalcounselingcomponentinmultidisciplinary treat-mentforadolescentobesityappearstoprovidebenefitsobservedforimprovedQOLascompared withtreatmentwithoutpsychologicalcounseling.
©2016SociedadeBrasileiradePediatria.PublishedbyElsevierEditoraLtda.Thisisanopen accessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/licenses/by-nc-nd/ 4.0/).
PALAVRAS-CHAVE
Intervenc¸ão multidisciplinar; Adolescentesobesos; Aconselhamento psicológico
Efeitosdeumaintervenc¸ãopsicológicasobreaqualidadedevidadeadolescentes obesosemtratamentomultidisciplinar
Resumo
Objetivo: Parainvestigarosefeitosdotratamentomultidisciplinarcomesemaconselhamento psicológicovoltadoàqualidadedevidadeadolescentesobesos.
Métodos: 76adolescentesobesos(15,87±1,53ano)foramalocadosemumgrupode aconsel-hamentopsicológicoe(GAP;n=36)ougrupodecontrole(GC;n=40)por12semanas.Todosos participantesreceberamomesmotreinamentofísicosupervisionadoeaconselhamento nutri-cionaleclínico.OsparticipantesnoGAPtambémreceberamaconselhamentopsicológico. A qualidadedevidafoiavaliadaantesedepoisdas12semanasdeintervenc¸ãopormeiodeum QuestionárioGenéricodeAvaliac¸ãodaQualidadedeVida(SF-36).
Resultados: OabandonodotratamentofoimaiornoGC(22,5%),emcomparac¸ãoaoGAP(0,0%) (p<0,001).Após12semanas,osparticipantesdoGAPapresentammenorpesocorporal,massa gordarelativaemaiormassalivredegordura(p<0,001paratodos)emcomparac¸ãoaoGC.A qualidadedevidamelhorouentreosadolescentesdeambososgrupos(p<0,05);contudo,uma melhorqualidadedevidafoirelatadapelosadolescentesincluídosnoGAP.
Conclusão: Ainclusãodeaconselhamentopsicológiconotratamentomultidisciplinardos ado-lescentesobesospareceproporcionarbenefíciosobservadosnamelhoriadaqualidadedevida, emcomparac¸ãoaotratamentosemaconselhamentopsicológico.
©2016SociedadeBrasileiradePediatria.PublicadoporElsevierEditoraLtda.Este ´eumartigo OpenAccesssobumalicenc¸aCCBY-NC-ND(http://creativecommons.org/licenses/by-nc-nd/4. 0/).
Introduction
Obesityanditsassociatedriskfactorshavebecomeamajor publichealthconcern.1---4Theworldwideprevalenceof over-weightamongchildrenandadolescents(aged5---17years)is estimatedat21.4%forgirlsand22.9%forboys.5InBrazil,the prevalenceofchildhoodandadolescentoverweight/obesity ranges from 4% to 37% in the different regions of the country.6
Studiesshowthatadolescenceobesityisassociatedwith an increased likelihood of depression, anxiety, and eat-ing disorders, which may affect quality of life (QOL).7---9 StudieshavedemonstratedlowerQOLinthephysical, psy-chosocial,emotional,andschoolfunctioningdomainsamong obesechildren andadolescentswhencomparedwiththeir normal weight peers10---12; a multidisciplinary behavioral treatment positively impacts QOL in this population.13 In fact, multidisciplinary behavioral interventions composed by regular physical activity, nutrition, and psychological counselinghavebeenwidelyacclaimedasthemosteffective approachfortreatingobesity.14,15Moreover,such interven-tionsappeartobemoreeffectivewithchildren/adolescents thanadults.16
Improvementsinweightandbodycompositionare com-monasaresultofamultidisciplinarybehavioraltreatment forobesity.10Improvementsinpsychologicalwell-beingand qualityof life are commonas well.8,9,17---19 Better psycho-logicaloutcomesmayresultfromchangesinweightstatus
andbodycompositionfollowinganincreaseinparticipants’ physicalactivitylevelsandimprovements ineating behav-ior. These psychological outcomes may also be directly related to a treatment including psychological counsel-ing;however,tothebestoftheauthors’knowledge,none of the previous researches were conducted to verify the contribution of psychological counseling onQOL in obese adolescentssubmitted toamultidisciplinary therapy. Psy-chologicalcounselingtargetsabroadvarietyoffactors,such asphysical, psychosocial,emotional, and school function-ing in the context of changing health-related behaviors. As such,psychological counseling per se could be affect-ingchangesinpsychologicaloutcomesandadolescents’QOL beyondtheeffectsobservedasaresultofchangesinweight statusorbodycomposition.Thus,themainpurposeofthis study wastoinvestigatethe effectsof amultidisciplinary treatmentforadolescentobesitywithandwithout psycho-logical counselingonparticipants’self-reported qualityof life.Secondaryoutcomesincludedtherapyadherence,and anthropometricandbodycompositionmeasures.
Methods
Sample
407 adolescents registered
Baseline assessements
Motivation interview
Psychological counseling group (PCG) (n=36) Control group (CG) (n=40)
12 weeks - evaluations
36 adolescents 27 adolescents - 335 excluded, didn’t fulfill inclusion criteria
Figure1 Flowofparticipantsthroughthestudyprocess.
media(newspaper,radio,andtelevision)intheurbanarea of Recife, Brazil. The study was approved by the Ethics CommitteeoftheUniversity ofPernambuco(No.154/09); parentsorguardianssignedan informedconsent,and par-ticipantssignedanassentform.Theinclusioncriteriawere: agerange13---18years;pubertalstage:Tanner3---420,21; obe-sity:BMI>95thpercentile22;andnopre-existingconditions that would restrict participation in an exercise program. Additionalexclusioncriteriaincluded pregnancy,presence of hypertensionand/or anothermetaboliccondition (such asdiabetestypeIIdiabetesandhyperlipidemia),anduseof weightlossmedications.
Studyprotocol
A total of 407 adolescents were screened for the study. Duringthefirstlaboratoryvisit,potentialparticipantswere instructedtoself-assessandreporttheirperceivedpubertal stage;heightandweightwasmeasured.Atthesecondvisit, an individual, semi-structured interview containing eight questionswasconductedby apsychologist. The interview assessedmotivesforseekingweightlosstreatmentand bar-rierstolosingweight.Duringathirdvisit,theadolescents underwentamedicalscreeningandrestingECG’swere per-formed.Threehundredthirty-twoadolescentsdidnotmeet inclusioncriteriabasedonthescreeningresults.Atotalof 76obeseadolescents(27boysand49girls)whometall inclu-sioncriteriawereenrolledinthestudy.Followingbaseline
testing,participantswereallocatedintoeither psycholog-icalcounseling group (PCG; n=36) or control group (CG; n=40)for12weeksofamultidisciplinaryinterventionthat includedsupervisedexercisetrainingsessions,nutritional, andclinicalcounseling(Fig.1).ParticipantsenrolledinPCG alsoreceivedpsychologicalcounseling.Fig.1presentsthe flowofparticipantsthroughthestudyprocess.
Multidisciplinarytreatment
Clinicalcounseling
Medical follow-up was performed once a month by an endocrinologist. This included a physical examination to monitorclinicalparametersandtofacilitateoverall compli-ancewiththestudy.
Nutritioneducation
Supervisedaerobicexercisetraining
The adolescentsunderwent an exercise program adminis-teredona treadmillandsupervisedbyphysical educators threetimesperweek(36sessionstotal).Theintensityofthe exercisetraining(50---60% of themaximum oxygen uptake [VO2max]) was individualized, based on each adolescents’ ventilatorythreshold1 (VT1)obtained froman incremen-taltest ona treadmillwithafixed inclinationof1%.23 All exercisesessionshadasetcaloricexpenditureat350kcal (1050kcalweek−1)anddurationwasdeterminedas:
Exercisesessiontime(min)
=350kcal/(VO2ontargetintensity×1MET)
Psychologicalcounseling
Psychologicalcounselingwasconductedfor onehoureach weekinsmallgroups(approximatelynineadolescents)bya clinicalpsychologist. Alongwiththepsychological motiva-tionforcompliance,themesrelatedtobodyimage,eating disorders (symptoms and consequences), the relationship between food and feelings, family and social problems, mood,anxiety,anddepressionwereincluded.
Measurements
Allparticipantsunderwentthe sameassessment protocol, atthebeginningandattheendofthe12-weektreatment. Assessmentswereperformed duringa similartimeof day toavoidcircadianinfluence.Thesameevaluatorconducted theassessmentsforbothcohorts.
Pubertalmaturation
Each participantwas givendrawings of the five stages of breast, genital, and pubic hair development. They were instructedtolookatthedrawings,readtheaccompanying descriptions,think about their ownphysical development andappearanceincomparisontothedrawings,andpickthe onethatmostcloselyresembledtheirownstageofphysical maturity.
Anthropometryandbodycomposition
Participantswereweighedbarefootandwearinglight cloth-ingonaFilizolascale(model160/300,Brazil)tothenearest 0.1kg. Stature was measured to nearest 0.5cm using a wall-mountedstadiometer (Filizolascale, model 160/300, Brazil).Bodymassindex(BMI)wascalculatedin kgm−2.22 Triceps, subscapular,andmedial calfskinfoldswere mea-sured in triplicate with a caliper (Lange, CA, USA) with constantpressure(10gmm−2)andresolutionof1mm,onthe
righthemisphere;themeanvaluewasused.Body composi-tionwasestimatedbygender-specificequations.24
Generic Questionnairefor the Evaluation of Quality of Life:‘MedicalOutcomesStudySF-36’.
The SF-36, translated into Portuguese and validated for the Brazilian population,25 was used to assess the adolescents’ quality of life (QOL). The instrument is multidimensional. It consists of 36 items, and is intended to generically evaluate QOL. The question-nairehaseightmulti-item subscales:physicalfunctioning, role-physical, pain, general health perception, vitality, social functioning, role-emotional, mental health, plus a
one-itemmeasureofself-evaluatedchangeinhealthstatus overthepastyear.
Statisticalprocedures
AllanalyseswereperformedusingthesoftwareStatistica® 7.0 for Windows®. Normality was verified by the Shapiro---Wilktestanddatawerepresentedasmeans±SD; differences in outcomes between times (baseline and 12 weeks)andgroupswereanalyzedusingtwo-wayANOVAwith aDuncanposthoctest.Duetobaselinedifferencesbetween groupsfor%FM,physicalfunctioning,generalhealth percep-tion,and meanof dimensionsof QOL,additional analyses were performed with ANCOVA,where thebaseline values wereincludedascovariates.Thesignificancelevelwasset atp<0.05.
Results
Ofthe76adolescentswhoparticipatedinthestudy,100% fromPGC(n=36)and67.5%fromGC(n=27)completedthe 12-week of multidisciplinary therapy (p<0.001). At base-line,differencesinheightandrelativefatmass(%FM)were observedbetweengroups(p<0.05forboth).
Multidisciplinarytherapy waseffective in reducing BMI (PCG=2.6%andCG=0.5%;F1,61=37.05;p<0.001),fatmass (PCG=24% and CG=10.3%; F1,59= 12.78; p<0.001) and to increase FFM (PCG=21.2% and CG=13.5%; F1,60= 55.34; p<0.001).At theend of12 weeks,participantsfromPCG presentedlowerbodyweight(2.3%,F1,61=7.03;p<0.001), %FM (PCG=13.7%, F1,59=12.78; p<0.001) and higher FFM (PCG=7.7%, F1,60=55.34; p<0.001) when compared GC (Table1).
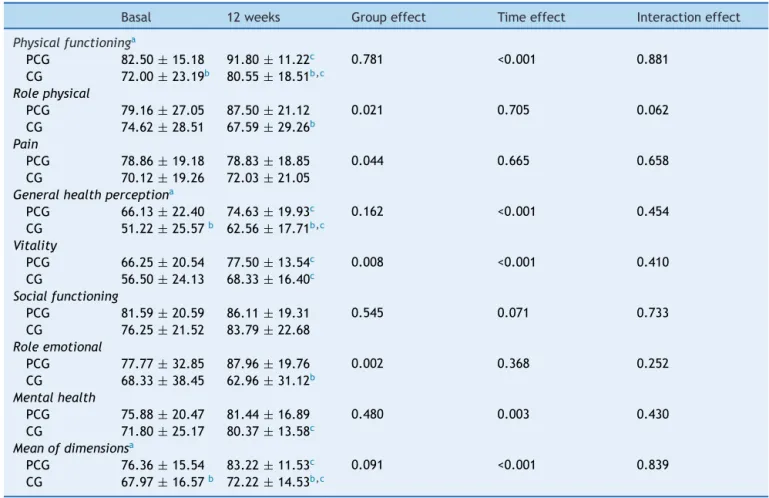
As shown in Table 2, adolescents from both PCG and CGpresentedanoverallimprovementonthedimensionsof QOL, suchasphysical functioning,general health percep-tion,vitality,andmeanofdimensions.However,highvalues ofself-reportedQOLwereobservedinadolescentsenrolled inthePGC.
Discussion
The data from the present study provided evidence that including psychological counseling in a multidisciplinary treatment is more effective for improving QOL when comparedwithatreatmentthatdoesnotincludeit. Further-more,psychologicalcounselingmayreducedropoutrate.
Thediscussionsof topicssuchassocialacceptanceand self-motivation may have encouraged adolescents to fur-thermodifytheirlifestyle,makingthemmoreawareofthe importanceofphysicalactivityandnutrition,10,11,26---29 lead-ingtopositivechangesonbodycomposition,asobservedin thepresentstudy,whichhasbeenidentifiedasaprotective factoragainstdiseasedevelopment(e.g.,hypertension, dia-betes, dyslipidemia,andcardiovascular problems)1,2,4,26---29 andassuchmayalsoimprovetheQOLofindividuals.30
Table1 Effectsofmultidisciplinarytherapywithandwithoutpsychologicalcounselingonanthropometryandbodycomposition inobeseadolescents.
Baseline 12weeks Groupeffect Timeeffect Interactioneffect
BM(kg)
PCG 91.26±11.22 89.16±11.98b 0.022 0.001 0.010
CG 95.87±10.33 96.72±10.98c
BMI(kg−1m2)
PCG 34.48±3.88 33.61±3.92b 0.505 <0.001 0.222
CG 34.55±3.36 34.40±3.73b
FFM(kg)
PCG 44.14±7.50 53.51±8.72b <0.015 <0.001 0.029
CG 42.03±5.20 47.73±4.56b,c
FMa
PCG 51.61±8.39 39.23±8.46b <0.001 <0.001 0.002
CG 56.04±5.89 50.28±4.76b,c
BM,bodymass;BMI,bodymassindex;FFM,fatfreemass;%FM,relativefatmass;PCG,psychologicalcounselinggroup;CG,control group.
p≤0.05.
a ANCOVA. b vs.basal. c vs.PCG.
Table2 Effectsofmultidisciplinarytherapywithandwithoutpsychologicalcounselingonqualityoflifeinobeseadolescents.
Basal 12weeks Groupeffect Timeeffect Interactioneffect
Physicalfunctioninga
PCG 82.50±15.18 91.80±11.22c 0.781 <0.001 0.881
CG 72.00±23.19b 80.55±18.51b,c
Rolephysical
PCG 79.16±27.05 87.50±21.12 0.021 0.705 0.062
CG 74.62±28.51 67.59±29.26b
Pain
PCG 78.86±19.18 78.83±18.85 0.044 0.665 0.658
CG 70.12±19.26 72.03±21.05
Generalhealthperceptiona
PCG 66.13±22.40 74.63±19.93c 0.162 <0.001 0.454
CG 51.22±25.57b 62.56±17.71b,c
Vitality
PCG 66.25±20.54 77.50±13.54c 0.008 <0.001 0.410
CG 56.50±24.13 68.33±16.40c
Socialfunctioning
PCG 81.59±20.59 86.11±19.31 0.545 0.071 0.733
CG 76.25±21.52 83.79±22.68
Roleemotional
PCG 77.77±32.85 87.96±19.76 0.002 0.368 0.252
CG 68.33±38.45 62.96±31.12b
Mentalhealth
PCG 75.88±20.47 81.44±16.89 0.480 0.003 0.430
CG 71.80±25.17 80.37±13.58c
Meanofdimensionsa
PCG 76.36±15.54 83.22±11.53c 0.091 <0.001 0.839
CG 67.97±16.57b 72.22±14.53b,c
PCG,PsychologicalCounselingGroup;CG,ControlGroup. p≤0.05.
studiesshould considerthe reasonsfor earlydropout and factorscontributingtotreatmentcompletion.
Although it is known that engaging in regular physical exerciseimproves QOL,7,9,27 recentstudieshavesuggested thatthe additionof a behavioral component anda nutri-tionalinterventionprovidesthemostchangesinQOLamong obeseindividuals.3,10,12,13Inthosestudies,overweight ado-lescents reported lower QOL when compared with their normalweightpeers.This wasobservednot onlyontheir totalscore,butalsoonthephysical, social,psychosocial, andschooldomainsasassessedbythePedsQL4.0, suggest-ing that lowerQOL affects adolescents ona daily basis.8 Obeseindividuals aremore vulnerabletosocial injustices (e.g.,bullying,discriminationinschool,socialisolation)and arelikelytofaceprejudice,whichmayresultinpoorerQOL. Behavioral interventionsthat aim to promote lifestyle changes (increasing physical activity and improving diet quality)areidentifiedaseffectiveforimprovingQOL,among both adolescentsand adults. It is noteworthy that, while comparing the groups of this study, those who received psychological counseling reported a higher QOL on some domains(physicalfunctioning,rolephysical,generalhealth perception, mean of dimensions). The results from the presentstudyareconsistentwithotherstudiesthat demon-stratedthatobesity treatmentshouldfocusonchangesin lifestyleandbeconductedby amultidisciplinary team.7---9 However,todate, thiswasthefirststudy toevaluatethe effectofaddingpsychologicalcounselinginsucha multidis-ciplinaryintervention.
Alimitationofthisstudy wastheuseof agenericQOL questionnaire,which maybelesssensitive than aspecific questionnaire. Another limitation is the fact that, of the participantswhostartedout inCG,only 67.5%completed theintervention,whichreducedthegeneralizabilityofthe conclusions drawn from this study. However, the dropout rateobserved in thisstudy wasnot anyhigher than what isexpectedininterventionstudies.
Inconclusion,multidisciplinarytreatmentimproves qual-ity of life among obese adolescents; the outcomes are improvedwhenpsychologicalcounselingisincluded. More-over,theinclusionofapsychologicalcounselingcomponent may reduce the dropout ratio commonly observed in the obesitytreatmentinadolescents.
Funding
All phases of this study were supported by the Con-selhoNacionaldeDesenvolvimentoCientíficoeTecnológico (CNPQ).DatacollectionwasperformedattheUniversityof Pernambuco.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgements
All phases of this study were supported by the Con-selhoNacionaldeDesenvolvimentoCientíficoeTecnológico
[CNPQ). Data collection was performed by the Grupo de EstudosemNutric¸ãoeExercício(GENE).
References
1.SinhaA,KlingS.Areviewofadolescentobesity:prevalence, etiology,andtreatment.ObesSurg.2009;19:113---20.
2.HillsAP,AndersenLB,ByrneNM.Physicalactivityandobesityin children.BrJSportsMed.2011;45:866---70.
3.Pulgarón ER. Childhood obesity: a review of increased risk for physical and psychological comorbidities. ClinTher. 2013;35:A18---32.
4.SparlingPB,FranklinBA,Hill JO.Energybalance:thekey to aunifiedmessageondietand physicalactivity.JCardiopulm RehabilPrev.2013;33:12---5.
5.Pérez Rodrigo C. Current mapping of obesity. Nutr Hosp. 2013;28:21---31.
6.SouzaCO,SilvaRC.Factorsassociatedwithexcessweightin Brazilianchildrenandadolescents:review.JBrazilianSocFood Nutr.2009;34:201---16.
7.Burgi´c-Radmanovi´cM,Gavri´cZ,Strki´cD.Eatingbehavior disor-dersoffemaleadolescents.PsychiatrDanub.2009;21:297---301. 8.KunkelN,OliveiraWF,PeresMA.Overweightandhealth-related qualityoflifeinadolescentsofFlorianópolis,SouthernBrazil. RevSaudePubl.2009;43:226---35.
9.PoetaLS,DuarteMdeF,GiulianoIde C.Health-related qual-ity of life of obese children. Rev Assoc Med Bras (1992). 2010;56:168---72.
10.Dalle Grave R, Calugi S, Centis E, El Ghoch M, Marchesini G. Cognitive-behavioral strategies to increase the adher-ence to exercise in the management of obesity. J Obes. 2011;2011:348293.
11.JacobJJ,IsaacR.Behavioraltherapyformanagementof obe-sity.IndianJEndocrinolMetab.2012;16:28---32.
12.PorteladeSantana ML,daCostaRibeiroJuniorH,MoraGiral M,RaichRM.Epidemiologyandriskfactorsofeatingdisorderin adolescence:areview.NutrHosp.2012;27:391---401.
13.Lofrano-PradoMC,AntunesHK,doPradoWL,dePianoA,Caranti DA,TockL,etal.QualityoflifeinBrazilianobeseadolescents: effectsofalong-termmultidisciplinarylifestyletherapy.Health QualLifeOutcomes.2009;7:61.
14.FreitasCR,Lofrano-PradoMC,GomesPP,AlmeidaNC,Ferreira MN,PradoWL.Efeitodaintervenc¸ãomultidisciplinar sobrea insatisfac¸ãodaimagemcorporalemadolescentesobesos.Rev BrasAtivFisSaude.2012;17:449---56.
15.Curioni CC, Lourenc¸o PM. Long-term weight loss after diet and exercise: a systematic review. Int J Obes (Lond). 2005;29:1168---74.
16.SnethenJA,BroomeME,CashinSE.Effectiveweight lossfor overweightchildren:ameta-analysisofinterventionstudies.J PediatrNurs.2006;21:45---56.
17.GunnarsdottirT,NjardvikU,OlafsdottirAS,CraigheadL, Bjar-nasonR.Childhoodobesityandco-morbidproblems:effectsof Epstein’s family-basedbehaviouraltreatmentinan Icelandic sample.JEvalClinPract.2012;18:465---72.
18.HoM,GarnettSP,BaurL,BurrowsT,StewartL,NeveM,etal. Effectivenessoflifestyleinterventionsinchildobesity: system-aticreviewwithmeta-analysis.Pediatrics.2012;130:e1647---71. 19.ZabelinaDL,EricksonAL,KolotkinRL,CrosbyRD.Theeffectof ageonweight-relatedqualityoflifeinoverweightandobese individuals.Obesity(SilverSpring).2009;17:1410---3.
20.Marshall WA, Tanner JM. Variations in pattern of pubertal changesingirls.ArchDisChild.1969;44:291---303.
22.Cole TJ, Bellizzi MC, Flegal KM, Dietz WH. Establishing a standarddefinitionforchildoverweightandobesityworldwide: internationalsurvey.BMJ.2000;320:1240---3.
23.PorszaszJ,CasaburiR,SomfayA,WoodhouseLJ,WhippBJ.A treadmillrampprotocolusingsimultaneouschangesinspeed andgrade.MedSciSportsExerc.2003;35:1596---603.
24.SlaughterMH,LohmanTG, BoileauRA, HorswillCA,Stillman RJ, Van Loan MD, et al. Skinfold equations for estimation of body fatness in children and youth. Hum Biol. 1988;60: 709---23.
25.CiconelliRM.Traduc¸ãoparaoportuguêsevalidac¸ãodo ques-tionáriogenéricodeavaliac¸ãodequalidadedevida‘‘medical outcomes study 36-item short-form health survey (SF-36)’’. [Thesis].SãoPaulo,Brazil:UNIFESPEscolaPaulistadeMedicina; 1997.
26.Al-Hazzaa HM, Abahussain NA, Al-Sobayel HI, Qahwaji DM, MusaigerAO.Physicalactivity,sedentarybehaviorsanddietary
habits among Saudi adolescentsrelative to age, gender and region.IntJBehavNutrPhysAct.2011;8:140.
27.Teixeira PJ, Silva MN, Coutinho SR, Palmeira AL, Mata J, Vieira PN, et al. Mediators of weight loss and weight loss maintenance inmiddle-agedwomen.Obesity (SilverSpring). 2010;18:725---35.
28.Bianchini JA,da Silva DF,Nardo CC,Carolino ID, Hernandes F, Nardo NJr. Multidisciplinary therapy reduces risk factors for metabolic syndrome inobese adolescents. EurJPediatr. 2013;172:215---21.
29.Fortes LS, Morgado FF, Ferreira ME. Factors associated with inappropriate eating behavior in adolescent students. Rev PsiquiatrClín.2013;40:59---64.