RevBrasAnestesiol.2016;66(6):654---656
REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
PublicaçãoOficialdaSociedadeBrasileiradeAnestesiologiawww.sba.com.br
CLINICAL
INFORMATION
Spinal
injection
of
local
anesthetic
during
cervical
facet
joint
injection
Juan
A.
Ramos
UniversidadedeCarabobo,DepartamentodeAnestesiología,Valencia,Venezuela
Received21February2014;accepted28April2014 Availableonline2June2014
KEYWORDS
Injections; Intra-articular;
Zygapophysealjoint;
Painmanagement
Abstract
Introduction:Facetjointpainisacommonsourceofnon-radicularbackpainworldwide. Non-surgicalinterventionalmodalitiesremainthemainstayinthetreatmentoffacetogenicback painandcomprisethesecondmostcommonlyperformedinterventionalpainproceduresinthe USA.
Case:A 36 year-old man with chronic cervical pain secondary to C6---C7 facet arthrosis radiographically,underwent diagnosticlocalanesthetic bilateral facetjoint injectionunder fluoroscopic guidance. The left sidewas injected uneventfully; however, 1---2min following injectionoftherightsidethepatientcomplainedofunwellnessandbecameveryanxious.He referredparesthesiasofthebilateral upperextremities,chestandupperabdomen.Physical examinationshowedsensorydeficitsroughlyfromC5toT7withoutmotordeficits; resuscita-tionmeasureswerenotwarranted.Thedeficitswerecompletelyresolvedby35---40mininthe recoveryarea.
Discussion: Facet joint injections are a common and safe method of treating back pain secondaryto facetarthropathy.Despiteexcellent safetyprofiles,rare andsometimes, life-threatening complications can occur. Our case hypothesizes intrathecal injection of local anesthetic during facet joint injection. Few reports have described similar situations. We hypothesizeamechanismofentry throughthefacetjoint,given theproximity ofthe liga-mentumflavum,andtheintrathecalspacetotheanterioraspectofthefacetjoint.Thisreport reinforcestheneedforresuscitationandairwaymanagementequipmenttobereadilyavailable whereinterventionalproceduresareperformed,aswellastheneedforadequateproficiency inairwaymanagementandresuscitationtechniquesinPainMedicinetraining.
©2014SociedadeBrasileiradeAnestesiologia.PublishedbyElsevierEditoraLtda.Thisisan openaccessarticleundertheCCBY-NC-NDlicense( http://creativecommons.org/licenses/by-nc-nd/4.0/).
E-mail:[email protected]
http://dx.doi.org/10.1016/j.bjane.2014.04.004
Spinalinjectionoflocalanestheticduringcervicalfacetjointinjection 655
PALAVRAS-CHAVE
Injec¸ões; Intra-articular;
Articulac¸ões
zigoapofisárias;
Controledador
Injec¸ãoespinhaldeanestésicolocalduranteinjec¸ãoemfacetasarticularescervicais
Resumo
Introduc¸ão: Adornasarticulac¸õesfacetáriaséumafontemundialmentecomumdedoresnas costas não radiculares.As modalidades de intervenc¸ões não cirúrgicas continuam sendoos pilaresnotratamentodadorsalgiafacetáriaeocupamosegundolugarentreosprocedimentos maiscomumentefeitosnosEUAparaomanejodador.
Relatodecaso: Pacientedosexo masculino,36anos, comdorcervicalcrônicasecundária à artrosefacetáriaemC6-C7(confirmadaporradiografia),submetidoaexamediagnóstico bilat-eraldasfacetascominjec¸ãodeanestésicolocalsoborientac¸ãofluoroscópica.Oladoesquerdo foi injetadosem intercorrências;porém,um-doisminutos apósainjec¸ão dolado direito, o pacientequeixou-sedemal-estareficoumuitoansioso.Mencionouparestesianosbrac¸os,no tóraxenoabdomesuperior.Oexamefísicoreveloudéficitssensoriaisde,aproximadamente, C5aT7,semdéficitmotor;medidasdereanimac¸ãonãoeramjustificáveis.Osdéficitsforam completamenteresolvidosem35-40minutosnaáreaderecuperac¸ão.
Discussão: Aaplicac¸ãodeinjec¸õesnasarticulac¸õesfacetáriaséummétodocomumeseguro detrataradornascostassecundáriaàartropatiafacetária.Apesardosexcelentesperfisde seguranc¸a,complicac¸õesrarase,àsvezes,comriscodemortepodemocorrer.Nossocasorelata ainjec¸ãointratecaldeanestésicolocalduranteinjec¸ãonasfacetasarticulares.Poucosrelatos descreveram situac¸ões semelhantes. Levantamos a hipótese de um mecanismo de entrada atravésdafacetaarticular,porcausadaproximidadedoligamentoamareloedoespac¸o intrate-calcomoaspectoanteriordafacetaarticular.Esserelatoreforc¸aanecessidadedereanimac¸ão edeequipamentospara omanejodasviasaéreasestarem prontamentedisponíveisquando procedimentosintervencionistassãofeitos,bemcomoanecessidadedeestabelecerodomínio doconhecimentonomanejodasviasaéreasedastécnicasdereanimac¸ãoetreinamentoem medicinadador.
©2014SociedadeBrasileiradeAnestesiologia.PublicadoporElsevierEditoraLtda.Este ´eum artigo OpenAccess sobumalicenc¸aCCBY-NC-ND( http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Chronicbackpainisacommonandseriousprobleminthe modernworld,withupto84percentofadultssufferingfrom itatsomepointintheirlives.1
Facetjoint(FJ)pain,painwhicharisesfromarthrosisof thezygapophysealjointsinthespine,isacommonsourceof non-radicularbackpain,withanestimatedpointprevalence ashighas15---40%inthelumbar spine2 and45---55%in the
neck.3
Despite controversial evidence supporting its efficacy,4
non-surgical interventional modalities to treat these dis-orders (i.e.FJ injections, MedianBrach Blocks(MBB) and RadiofrequencyAblations(RFA)oftheMBB)stillremainthe mainstay in the treatment of facetogenic back pain5 and
comprise the second mostcommonly performed interven-tionalpainproceduresin USA.6 Wepresent an uncommon
complication of these common procedures, a case of intrathecallocalanestheticinjectionduringFJinjection.
Case
An otherwise healthy 36-year-old man with a history of chronic cervical back pain of 10 months duration, sta-tus post-anterior cervical spinal fusion, withC6---C7 facet
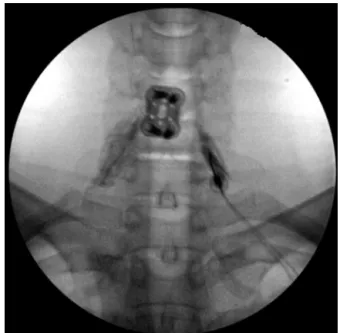
arthrosisradiographically,underwentdiagnosticlocal anes-thetic bilateral FJ injection. The patient was positioned prone,andunder fluoroscopythe C6---C7 FJ waslocalized andmarked,followedbychlorhexidinesterilefield prepa-rationanddraping.A22-gaugespinalneedlewasinserted percutaneouslyanddirectedunderfluoroscopyuntil inser-tionthroughthejointcapsulewasfeltasadropintothejoint space.Thiswasconfirmedwithinjectionof0.5mLof iodine-basedcontrastmediawithsatisfactoryarthrograms(Fig.1), followedbynegativeaspirationandsubsequentinjectionof 1mL of 0.5% Bupivacaine onthe left and 0.75mL onthe rightasallowedbycomplianceofthejointspace.Theleft sidewasinjecteduneventfully;however,1---2minfollowing injectionoftherightside,thepatientcomplainedof unwell-nessandbecamevery anxious.He wasturnedsupineand wasadministeredoxygenbynasalcannula.Vitalsignsand oxygensaturationremainedunremarkablewiththe excep-tionofmildtachycardiaandtachypnea;basicintubationand resuscitationequipmentweremadereadilyavailable. The patientreferredparestheticsensations(pinsandneedles)to thebilateralupperextremities,chestandupperabdomen. Onphysicalexaminationthereweresensorydeficitsto tem-perature sensation in the areas referred by the patient, roughlyfromC5toT7withoutmotordeficits.
656 J.A.Ramos
Figure1 Fluoroscopic arthrogramof bilateral C6---C7 facet joints.
completelyresolvedby35---40minintherecoveryarea.No residualdeficitswerenotedandthepatientwasdischarged.
Discussion
FJinjectionsareacommonandsafemethodoftreating non-radicularbackpaininpatientswithfindingssuggestingfacet arthropathy.5 Despite excellent safety profiles, rare and
sometimes, life-threatening complications can occur. Our casedescribeswhatwehypothesizetobeintrathecal injec-tionof localanestheticduringaFJ injection.Few reports havedescribedsimilarsituationswithmorepronounced neu-rologic and hemodynamic effects,7,8 concomitantly these
occurredafterinjectionofspinalanesthetic(10mg approx-imately)dosesofBupivacaineintrathecally.Wehypothesize amechanismofentrythroughtheFJ,giventheproximityof theligamentumflavum,andconsequentially,theintrathecal spacetotheanterioraspectofFJcapsule.9Theminuscule
doseof Bupivacaine(between2.5 and5mg)injectedmay accountforthelack ofsympathectomyandshortduration
of the symptoms. Another hypothesis would be subdural, ratherthanintrathecalspreadofthelocalanesthetic; how-ever, it is felt that the volume injected is insufficient to accountforsuchwidespreaddeficits.
This report reinforces the need for resuscitation equipment, including supplemental oxygen, intravenous accessories,intubationandmonitoring equipment,aswell as vasoactive medications to be readily available in any facilitywhereinterventionalproceduresareperformed,but mostly,itemphasizestheneedforadequateproficiencyin airway management and resuscitation techniques in Pain Medicinetraining,especiallyinphysicianswithout anesthe-siabackground.
Conflicts
of
interest
Theauthordeclaresnoconflictsofinterest.
References
1.CassidyJD,CarrollLJ,CoteP.TheSaskatchewanhealthandback painsurvey.Theprevalenceoflowbackpainandrelated disabil-ityinSaskatchewanadults.Spine.1998;23:1860---6.
2.BeresfordZM,KendallRW,WillickSE.Lumbarfacetsyndromes. PainPract.2010;10:113---23.
3.vanEerdM,PatijnJ,LatasterA, etal.5.Cervicalfacetpain. PainPract.2010;10:113---23.
4.ChouR, LoeserJD,OwensDK,et al.Interventionaltherapies, surgery,andinterdisciplinary rehabilitationforlowback pain: anevidence-basedclinicalpracticeguidelinefromtheAmerican PainSociety.Spine.2009;34:1066---77.
5.FalcoFJ,ManchikantiL,DattaS,etal.Anupdateofthe effec-tiveness oftherapeutic lumbarfacet joint interventions.Pain Physician.2012;15:E909---53.
6.ManchikantiL.Thegrowthofinterventionalpainmanagement inthenewmillennium:acriticalanalysisofutilizationinthe medicarepopulation.PainPhysician.2004;7:465---82.
7.Goldstone JC, Pennant JH. Spinal anaesthesia following facet joint injection. A report of two cases. Anaesthesia. 1987;42:754---6.
8.MarksR,SempleAJ.Spinalanaesthesiaafterfacetjoint injec-tion.Anaesthesia.1988;43:65---6.