w w w . r b o . o r g . b r
Original
Article
Risk
of
injury
to
vascular-nerve
bundle
after
calcaneal
fracture:
comparison
among
three
techniques
Pedro
José
Labronici
a,∗,
Vitor
Rodrigues
Reder
b,
Guilherme
Ferreira
de
Araujo
Marins
Filho
b,
Robinson
Esteves
Santos
Pires
c,
Hélio
Jorge
Alvachian
Fernandes
d,
Marcelo
Tomanik
Mercadante
eaUniversidadeFederalFluminense,Niterói,RJ,Brazil
b“Prof.Dr.DonatoD’Ângelo”OrthopedicsandTraumatologyService,HospitalSantaTeresa,Petrópolis,RJ,Brazil
cUniversidadeFederaldeMinasGerais,BeloHorizonte,MG,Brazil
dDepartmentofOrthopedicsandTraumatology,EscolaPaulistadeMedicina(EPM),UniversidadeFederaldeSãoPaulo(UNIFESP),
SãoPaulo,SP,Brazil
eSantaCasadeSãoPaulo,PavilhãoFernandinhoSimonsen,SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory: Received2May2015 Accepted15June2015
Availableonline16February2016
Keywords:
Calcaneus/injuries Orthopedicpins Bonescrews Operativesurgical procedures/methods
a
b
s
t
r
a
c
t
Objective:Toascertainwhetherthenumberofscrewsorpinsplacedinthecalcaneusmight increasetheriskofinjurywhenthreedifferenttechniquesfortreatingcalcanealfractures. Method:126radiographsofpatientswhosuffereddisplacedcalcanealfractureswere retro-spectivelyanalyzed.Threesurgicaltechniqueswereanalyzedonaninterobserverbasis:31 radiographsofpatientstreatedusingplatesthatwerenotspecificforthecalcaneus,48using specificplatesand47usinganexternalfixator.Theriskofinjurytotheanatomical struc-turesinrelationtoeachKirschnerwireorscrewwasdeterminedusingagradedsystemin accordancewiththeLichtclassification.Thetotalriskofinjurytotheanatomicalstructures throughplacementofmorethanonewire/screwwasquantifiedusingtheadditivelawof probabilitiesfortheproduct,forindependentevents.
Results:Allofthemodelspresentedhighexplanatorypowerfortheriskevaluated,sincethe coefficientofdeterminationvalues(R2)weregreaterthan98.6forallthemodels.Therefore,
thesetofvariablesstudiedexplainedmorethan98.6%ofthevariationsintherisksof injurytoarteries,veinsornervesandcanbeclassifiedasexcellentmodelsforprevention ofinjuries.
Conclusion:Theriskofinjurytoarteries,veinsornervesisnotdefinedbythetotalnumberof pins/screws.Theregionandthenumberofpins/screwsineachregiondefineanddetermine thebestdistributionoftherisk.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
∗
Correspondingauthor.
E-mail:[email protected](P.J.Labronici).
http://dx.doi.org/10.1016/j.rboe.2016.02.002
Risco
de
lesão
do
feixe
vasculonervoso
após
fratura
do
calcâneo:
comparac¸ão
entre
três
técnicas
Palavras-chave: Calcâneo/lesões Pinosortopédicos Parafusosósseos Procedimentoscirúrgicos operatórios/métodos
r
e
s
u
m
o
Objetivo: Verificarseonúmerodeparafusosoupinoscolocadosnocalcanharaumentariao riscodelesãoquandousamostrêstécnicasdiferentesparaotratamentodasfraturas. Método: Foramanalisadasretrospectivamente126radiografiasdepacientesquesofreram fraturadesviadadocalcanhar.Foramanalisadastrêstécnicascirúrgicassobaforma inter-observador:31radiografiasdepacientestratadoscomplacanãoespecíficaparaocalcanhar, 48complacaespecíficae47comfixadorexterno.Oriscodelesãodasestruturasanatômicas emrelac¸ãoacadafiodeKirschnerouparafusofoideterminadopelosistemadegraduac¸ão segundo aclassificac¸ãodeLicht. Aquantificac¸ão dorisco totalde lesãodasestruturas anatômicasnacolocac¸ãode maisdeum fio/parafusofoi calculadapela leiaditiva das probabilidadesdoprodutoparaeventosindependentes.
Resultados: Todososmodelosapresentaramumaltopoderdeexplicac¸ãodoriscoavaliado, umavezqueosvaloresdocoeficientededeterminac¸ãoR2 sãomaioresdoque98,6para
todososmodelos.Portanto,oconjuntodevariáveisestudadoexplicamaisde98,6%das variac¸õesdosriscosdelesãodasartérias,veiasoudosnervosepodemserclassificados comoexcelentesmodelosparaprevenc¸ãodelesões.
Conclusão: Oriscodelesãodasartérias,veiasoudosnervosnãoédefinidopelototalde pinos/parafusos.A regiãoeaquantidadedepinos/parafusosem cadaregiãodefineme determinammelhoradistribuic¸ãodorisco.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Fracturesofthecalcaneusaccountfor60%ofthefractures ofthetarsus.1,2Althoughcalcanealfracturesaccountforonly 1–2%ofallfracturesinallpartsoftheskeleton,theyarestill amajorchallengefororthopedists.2–6Inyoungpatients,they arefrequentlycausedbyhigh-energytrauma.Approximately 75%ofthesefracturesareintra-articular.4,7,8Calcaneal frac-turespresentahighrateofunsatisfactoryresults,withgreat morbidityforthepatients.
The ideal treatment for intra-articular fractures of the calcaneus remains a matter of controversy, despite the advancesin imaging diagnostics and surgical techniques.9 Several surgical techniques for treating displaced intra-articularfractures exist, andthese include:open reduction withinternalfixation,5,9minimallyinvasivetechniques,10 per-cutaneous techniques,11 percutaneous calcaneoplasty4 and externalfixation.12Independentofthetechniqueused, vari-ousanatomicalstructuresinthemedialregionoftheheelmay beatriskofiatrogenicinjuriescausedbythetipsofscrews, drillbits,externalfixatorpinsorKirschnerwires.13–15
Theobjectiveofthisstudywastoinvestigatewhetherthe numberofscrewsorpinsplacedintheheelwouldincreasethe riskofinjury,inusingthreedifferenttechniquesfortreating calcanealfractures.
Material
Aretrospectiveanalysiswasconductedon126radiographs on patients who suffered displaced fractures of the heel
in 2013and 2014.Cases offractures withoutdisplacement andfracturestreatedconservatively,andpatientsforwhom no postoperative radiographic control was available, were excluded.Threesurgicaltechniqueswereanalyzedin inter-observerform:31radiographsfrompatientswhoweretreated usingaplatethatwasnotspecificforthecalcaneus,48witha specificplateand47withanexternalfixator.Thesepatients weretreatedatfourinstitutions.
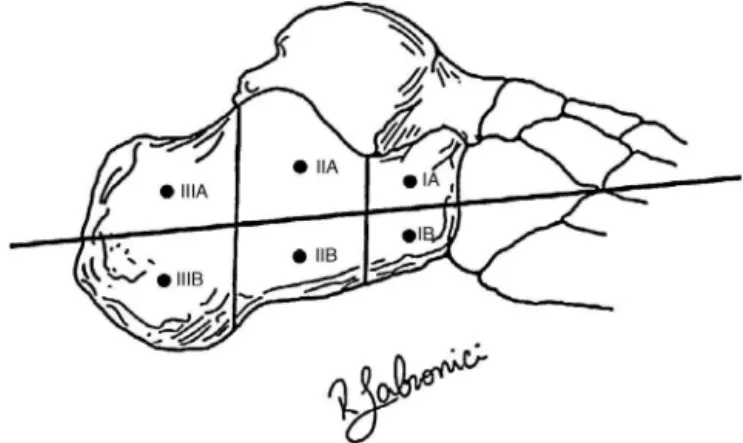
Tocalculatetheriskofinjurytonerves,arteriesandveins, theheelsweredividedintosixdifferentzones,asillustratedin
Fig.1.ZonesIAandIBwerelocatedintheanteriortuberosity ofthecalcaneus,fromthecalcaneocuboidjointlinetoalinein theregionofGisane’sangle.ZonesIIAandIIBwerelocatedin theregionofthecalcanealbody,fromthelineofGisane’sangle
Table1–Likelihoodofinjurytoarteries,veins,nerves andtendonsaccordingtothezoneoftheheel.
Zoneoftheheel Pointofcomparison
Artery Vein Nerve Tendon
IA 0.434 0.434 0.132 0.0
IB 0.208 0.208 0.132 0.0
IIA 0.151 0.170 0.113 0.0
IIB 0.038 0.038 0.038 0.0
IIIA 0.075 0.075 0.057 0.0
IIIB 0.019 0.019 0.019 0.0
Source:datafromthehospitalservicefiles.
totheendoftheposteriortuberosityofthetalus.ZonesIIIA
andIIIBwerelocatedintheregionoftheposteriortuberosity
ofthecalcaneus.
AccordingtoLabronicietal.,15theprobabilityofinjuriesto
thearteries,veins,nervesandtendonsinthesixzonesstudied wasbasedontheclassificationofLichtetal.16forhighrisk,as showninTable1.Thisstudydemonstratedthat,forexample, thelikelihoodofarteryinjuryuponcrossingthemedialcortex inzoneIAwas0.434or43.4%.
Generalizing,thetotallikelihoodofinjuryofan anatom-icalpoint,inplacingnwiresorscrews,isthesumofallthe individualprobabilities(onebyone)minustheprobabilitiesof thetwo-by-twocombinations,plustheprobabilitiesofallthe three-by-threecombinations,minustheprobabilitiesofallthe four-by-fourcombinations,plusthesumofallthefive-by-five combinations,andsoon,untilthen-by-ncombinationsare reached.
Pr(Fi)−
Pr(Fi∩Fj)+Pr(Fi∩Fj∩Fk)−
Pr(Fi∩Fj∩Fk∩Fl)+
Pr(Fi∩Fj∩Fk∩Fl∩Fm)
−Pr(F1∩F2∩F3∩F4∩F5∩F6)
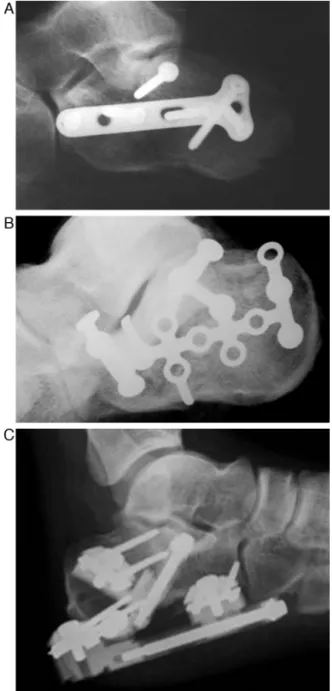
Thiswasthemathematicalformulathatwasdetermined forcalculatingtherisk.Itwastransformedintoacomputer programandthenwasanalyzedbythreeresearchers indepen-dently,inordertomeasurethethreetechniquesused(Fig.2).
Statistical
methodology
The data gathered were analyzed through multiple linear regression inthe SPSSsoftware (StatisticalPackageforthe SocialSciences),version22.0.Multiplelinearregression anal-ysisisatechniqueforconfirmingdependence.Itsaimisto examinethebehaviorofadependentvariable,measuredasa functionofotherexplanatoryvariables.Theobjectiveofthis study wastoevaluatethe relationship betweenthe riskof injurytoanartery,veinornerveandthenumberofscrewsor pinsplacedineachregionofthecalcaneus(A1,A2,A3,B1,B2 orB3).IfAiisthenumberofscrewsorpinsplacedinregionA,
index‘i’,andBiisthenumberofscrewsorpinsplacedinregion
B,index‘i’,thegenerallinearregressionmodelthatexplains therelationshipbetweentheriskofinjuringanartery,veinor
Fig.2–(A)Radiographofacalcanealfracturetreatedusing anonspecificplate;(B)radiographwithspecificplate;and (C)radiographwithexternalfixator.
nerveandthenumberofscrewsplacedineachregionisgiven by:
Risk=a1A1+a2A2+a3A3+b1B1+b2B2+b3B3+u, (1)
whereriskisthedependentvariable;aiandbiaretheangular
coefficientsofeachrespectivevariableAiandB;anduisthe
errortermorresidualdifferencebetweentherealriskandthe valuepredictedbythemodel.Thiserrorrepresentsthe vari-ablesthatwerenotincludedinthemodelandmayhavesome powerforexplainingtherisk.
wasevaluatedusingStudent’sttestandthesignificanceofthe modelwasevaluatedusingtheANOVAFtest.The assump-tionsofthemodel(i.e.normaldistributionoftheindependent variable,absenceofheteroscedasticityandabsenceof mul-ticollinearity)wereanalyzedusingtheKolmogorov–Smirnov test,GlejsertestandVIFandtolerancestatistics,respectively. Giventhatthe risks ofinjuringanartery, vein ornerve areindependent,alinearregressionmodelwasproposedfor eachoftherisks,foreachtypeofprocedureanalyzed: place-mentofnonspecificplates,platesspecificforthecalcaneus andexternalfixators.Inthis manner,nineregression mod-elswereobtained.Inadditiontotheanalysisonthemultiple linearregressionmodel,asimpleregressionmodelbetween theriskandthetotalnumberofpins(T)placedwasanalyzed, givenby:
Risk=aT+e, (2)
whereaistheangularcoefficientofthevariable tobe esti-matedandeistheerrorterm.
Despite the recommendation to use beta regression for the risk variable, since this is a variable of limited inter-val [0,1], simplelinear regression was chosenbecause this had the advantagesthat the results could be easily inter-preted,the samplesizeensured non-violationofnormality forthevariablesandnoneofthemodelsproposedviolatedthe assumptionsofthemultiplelinearregressionmodel(absence of heteroscedasticity and absence of multicollinearity). In addition,themodelswereevaluatedbymeansofbeta regres-sion, which confirmed the significance ofall the variables proposed,inallthemodels.
Results
Table2demonstratesthep-valuesoftheKolmogorov–Smirnov
test. This test was used to assess whether each of the
Table2–p-ValuesoftheKolmogorov–Smirnovtestfor thevariablesofriskofinjurytoarteries,veinsornerves, inthethreeproceduresinvolved,i.e.placementof nonspecificplates,platesthatarespecificforthe calcaneusandexternalfixators.
Procedure Riskofinjury
toarteries
Riskofinjury toveins
Riskofinjury tonerves
Non-specific plates
0.103 0.108 0.595
Platesspecificfor calcaneus
0.134 0.116 0.195
Externalfixators 0.070 0.062 0.639
dependentrisk variablespresentednormaldistribution,for
each typeofprocedure analyzed:placement ofnonspecific
plates,platesspecificforthecalcaneusandexternalfixators.
Itwasobservedthatnoneofthep-valuesgreaterthan5%led
torejectionofthenullhypothesisofnormality,whichwasthe
desiredsituation.
Inadditiontothetestfornormaldistribution,theGlejser
test and the VIF and tolerance statistics alsoprovided the
assurancethatheteroscedasticityandmulticollinearitywere
absentfromallthemodelsproposed.
Table3demonstratestheestimatesforthecoefficientsof
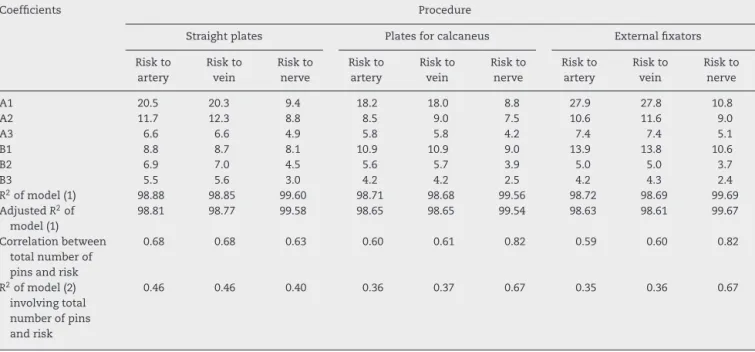
eachproposedmodel,describedasdefinedinEq.(1).Forthe nine modelsproposed,theoverall statisticalsignificanceof themodelwasconfirmed(p-valueoftheANOVAFtest<0.001), alongwiththesignificanceofallofthevariables(numbersof pinsandscrewsineacharea),separately(p-valueofStudent’st test<0.001).Allthemodelspresentedhighexplanatorypower fortheriskevaluated,giventhatthevaluesofthecoefficient ofdeterminationR2weregreaterthan98.6forallthemodels.
Therefore, thevariablesstudiedexplainedmorethan 98.6% ofthevariationoftherisksofinjurytothearteries,veinsor nerves,andcanbeclassifiedasexcellentmodelsforinjury pre-vention.Incomparingtheadjustedvaluesforthecoefficient
Table3–Estimatesofthecoefficientsofthelinearregressionmodelsandcoefficientofdeterminationofthemodel(R2).
Coefficients Procedure
Straightplates Platesforcalcaneus Externalfixators
Riskto artery Riskto vein Riskto nerve Riskto artery Riskto vein Riskto nerve Riskto artery Riskto vein Riskto nerve
A1 20.5 20.3 9.4 18.2 18.0 8.8 27.9 27.8 10.8
A2 11.7 12.3 8.8 8.5 9.0 7.5 10.6 11.6 9.0
A3 6.6 6.6 4.9 5.8 5.8 4.2 7.4 7.4 5.1
B1 8.8 8.7 8.1 10.9 10.9 9.0 13.9 13.8 10.6
B2 6.9 7.0 4.5 5.6 5.7 3.9 5.0 5.0 3.7
B3 5.5 5.6 3.0 4.2 4.2 2.5 4.2 4.3 2.4
R2ofmodel(1) 98.88 98.85 99.60 98.71 98.68 99.56 98.72 98.69 99.69
AdjustedR2of
model(1)
98.81 98.77 99.58 98.65 98.65 99.54 98.63 98.61 99.67
Correlationbetween totalnumberof pinsandrisk
0.68 0.68 0.63 0.60 0.61 0.82 0.59 0.60 0.82
R2ofmodel(2)
involvingtotal numberofpins andrisk
ofdeterminationR2,itwasobservedthatthemodelsfor
pre-dictingtheriskofnerveinjurywerebest,sincetheyexplained approximately100%oftherisk.
On the last two lines of Table 3, the correlation and coefficients ofdetermination R2 of the model proposed by
Eq. (2) are also analyzed. In this, the risk is only consid-eredasafunctionofthetotalnumber ofpins andscrews. It was observed that the models thus proposed presented lowexplanatorypowerfortherisk.Thus,thesemodelshave notbeen displayed. The riskofinjury to arteries,veins or nerveswasnotdefinedbythetotalnumberofpinsorscrews. Theregionandthenumberofpinsorscrewsineachregion explainedanddeterminedthedistributionofriskbetter.
Discussion
Foreachprocedure(nonspecificplates,platesspecificforthe calcaneusand externalfixators), this study usedstatistical multiplelinearregressionmodelsthatefficiently estimated theriskofinjurytoarteries,veinsandnervesfromthe num-berofpinsorscrewsthateachprocedureineachregionwould use.Tojudgewhichprocedureisleastinvasive,thenumberof pinsorscrewstobeplacedineachprocedureineachregion needstobeplannedandtheexpectedvaluefortherespective riskshouldbecalculatedfrom theequationsobtained.The coefficientsthusestimatedshowedthatthepinsandscrews intheregionA1weretheonesthatcontributedmosttoward increasingtheriskofinjurytothearteries,veinsornerves. PinsorscrewsintheregionsA2andB1alsocontributedtoward therisksofinjury.
Meticulousknowledgeoftheanatomyofthehindfootis animportantprerequisiteforplanningforplacementofpins orforopenreductionandinternalfixationofheelfractures. Structurescontainedwithinthetarsaltunnel,whichareclose tothemedialregionofthecalcaneus,arevulnerabletoinjury causedbypins,drillbitsorscrewsthatpenetratethemedial cortexofthecalcaneus.15Albertetal.17dividedthecalcaneus intothreezones.ZoneIstartsatthecalcaneocuboidjointand
extendsposteriorly asfar asGisane’scritical angle;zoneII
startsatGisane’sangleandextendsposteriorlytoincludeall oftheposteriorfacet;andzoneIIIencompassestheposterior
tuberosity.Theriskofinjurytothestructuresofthemedial regionwascalculatedforeachlocationintowhichpinswere insertedinthelateralregion.Theyconcludedthatpinsplaced inthesubchondralboneoftheposteriorfacetoranteriorto Gisane’scriticalanglemightincreasetheriskofinjurytothe medialstructuresofthecalcaneus.Labronicietal.15 demon-stratedthat divisioninto sixzones wasmorereproducible, withtheirrespectiverisksofinjurytotheanatomical struc-tures.Theriskofinjurycanbequantifiedthroughthelawof additionofprobabilities,andthisallowsbetterplanningwith regardtothesitesoflowerriskforpinplacement.However,it isimportanttoemphasizethedifficultyinvolvedinpredicting thelikelihoodofneurovascularinjurycausedbyanatomical variationsthatareencounteredinthetarsalcanal,with sub-divisionofthetibialnerveintoitsmedialplantar,lateraland medialcalcanealbranches.
Some authors18–21 observed that the injuries most fre-quentlyaffectingcutaneousnerves weretothesuralnerve
laterallyandthetibialnerveposteromedially.Theseinjuries usuallyresultinhypoesthesiaandaretreatedconservatively, exceptifaneuromadevelops,whichshouldthenbetreated surgically.
Conclusion
Throughcomparingtheriskestimatesobtained,surgeonscan evaluatewhichprocedurewouldbesafest,soastoavoidthe riskofinjurytoarteries,veinsornerves.
Thecoefficientsestimatedthroughthisstudyshowedthat pins and screws inthe region A1were the onesthat con-tributed most toward increasing the risk of injury to the arteries,veinsornerves.PinsorscrewsintheregionsA2and B1alsocontributedtowardtheriskofinjury.
Theriskofinjurytothearteries,veinsandnervesisnot definedbythetotalnumberofpinsandscrews.Theregion andthenumberofpinsandscrewsineachregionexplainand determinethedistributionoftherisk.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.RodríguezSR,Gardu ˜noRB,RaygozaCO.Surgicaltreatmentof
calcanealfractureswithaspecialtitaniumAOplate.Acta
OrtopMex.2004;18Suppl1:S34–8.
2.MedeirosCML,HenaoJES,RohenkohlC,HirataLM,Baruffi
NA,KleinJuniorA,etal.Avaliac¸ãofuncionaldasfraturas
intra-articularesdocalcâneotratadascirurgicamente.Rev
BrasOrtop.2008;43(11/12):482–9.
3.BanerjeeR,NickischF,EasleyME,DiGiovanniC.Footinjuries.
In:BrownerBD,JupiterJB,LevineAM,editors.Skeletal
trauma.4thed.Philadelphia:Saunders;2009.p.2585–748.
4.BiggiF,DiFabioS,D’AntimoC,IsoniF,SalfiC,TrevisaniS.
Percutaneouscalcaneoplastyindisplacedintraarticular
calcanealfractures.JOrthopTraumatol.2013;14(4):307–10.
5.FrankMA,BerberianW,LiporaceF.Calcanealfractures:
surgicalexposureandfixationtechniqueupdate.CurrOrthop
Pract.2011;22(1):4–11.
6.EneR,PopescuD,PanaitescuC,CircotaG,CirstoiuM,Cirstoiu
C.Lowcomplicationsafterminimallyinvasivefixationof
calcaneusfracture.JMedLife.2013;6(1):80–3.
7.JulianoP,NguyenHV.Fracturesofthecalcaneus.OrthopClin
NorthAm.2001;32(1):35–41.
8.LutterLD,MizelMS,PfefferGB.Orthopaedicknowledge
update.Footandankle.Rosemont,IL:AmericanAcademyof
OrthopaedicSurgeons;1994.
9.AgrenPH,WretenbergP,Sayed-NoorAS.Operativeversus
nonoperativetreatmentofdisplacedintra-articularcalcaneal
fractures:aprospective,randomized,controlledmulticenter
trial.JBoneJointSurgAm.2013;95(15):1351–7.
10.CaoL,WengW,SongS,MaoN,LiH,CaiY,etal.Surgical
treatmentofcalcanealfracturesofsanderstypeIIandIIIbya
minimallyinvasivetechniqueusingalockingplate.JFoot
AnkleSurg.2015;54(1):76–81.
11.BrigidoSA,GalliMM,BleazeyST,ProtzmanNM.Modular
stemfixed-bearingtotalanklereplacement:prospective
resultsof23consecutivecaseswith3-yearfollow-up.JFoot
12.DaytonP,FeilmeierM,HensleyNL.Techniqueforminimally
invasivereductionofcalcanealfracturesusingsmallbilateral
externalfixation.JFootAnkleSurg.2014;53(3):376–82.
13.MekhailAO,EbraheimNA,HeckBE,YeastingRA.Anatomic
considerationsforsafeplacementofcalcanealpins.Clin
OrthopRelatRes.1996;(332):254–9.
14.SantiMD,BotteMJ.Externalfixationofthecalcaneusand
talus:ananatomicalstudyforsafepininsertion.JOrthop
Trauma.1996;10(7):487–91.
15.LabroniciPJ,PereiraDN,PilarPHVM,FrancoJS,SerraMD,
CohenJC,etal.Localizac¸ãoseguranacolocac¸ãodospinos
percutâneosnocalcâneo.RevBrasOrtop.2012;47(4):455–9.
16.LichtNJ,RoweDE,RossLM.Pitfallsofpediclescrewfixation
inthesacrum.Acadavermodel.Spine(Phila,Pa,1976).
1992;17(8):892–6.
17.AlbertMJ,WaggonerSM,SmithJW.Internalfixationof
calcaneusfractures:ananatomicalstudyofstructuresatrisk.
JOrthopTrauma.1995;9(2):107–12.
18.HarveyEJ,GrujicL,EarlyJS,BenirschkeSK,SangeorzanBJ.
MorbidityassociatedwithORIFofintra-articularcalcaneus
fracturesusingalateralapproach.FootAnkleInt.
2001;22(11):868–73.
19.PaleyD,HallH.Intra-articularfracturesofthecalcaneus.
Acriticalanalysisofresultsandprognosticfactors.JBone
JointSurgAm.1993;75(3):342–54.
20.SandersR.Displacedintra-articularfracturesofthe
calcaneus.JBoneJointSurgAm.2000;82(2):225–50.
21.RammeltS,ZwippH.Calcaneusfractures:facts,controversies