www.jped.com.br
ORIGINAL
ARTICLE
The
Oxford
Classification
predictors
of
chronic
kidney
disease
in
pediatric
patients
with
IgA
nephropathy
夽
Rafaela
C.G.
Fabiano
a,
Stanley
A.
Araújo
b,
Eduardo
A.
Bambirra
b,
Eduardo
A.
Oliveira
c,
Ana
Cristina
Simões
e
Silva
c,d,∗,
Sérgio
V.B.
Pinheiro
caUniversidadeFederaldeMinasGerais(UFMG),HospitaldasClínicas,DivisãodeNefrologia,BeloHorizonte,MG,Brazil bUniversidadeFederaldeMinasGerais(UFMG),HospitaldasClínicas,DivisãodePatologiaRenal,BeloHorizonte,MG,Brazil cUniversidadeFederaldeMinasGerais(UFMG),FaculdadedeMedicina,UnidadedeNefrologiaPediátrica,BeloHorizonte,MG, Brazil
dUniversidadeFederaldeMinasGerais(UFMG),FaculdadedeMedicina,LaboratórioInterdisciplinardeInvestigac¸ãoMédica, BeloHorizonte,MG,Brazil
Received27June2016;accepted22September2016 Availableonline27January2017
KEYWORDS
IgAnephropathy; Glomerulonephritis; Chronickidney disease; Proteinuria;
OxfordClassification
Abstract
Objective: TheOxfordClassificationforImmunoglobulinAnephropathy(IgAN)identifies patho-logicalvariablesthatmaypredictthedeclineofrenalfunction.Thisstudyaimedtoevaluate theOxford ClassificationvariablesaspredictorsofrenaldysfunctioninacohortofBrazilian childrenandadolescentswithIgAN.
Methods: Atotalof54patientswithIgANbiopsiedfrom1982to2010wereassessed.Biopsies werere-evaluatedandclassifiedaccordingtotheOxford Classification.Multivariateanalysis oflaboratory andpathologicaldata wasperformed.The primaryoutcomeswere declineof baselineestimatedglomerularfiltrationrate(eGFR)greaterthanorequalto50%.
Results: Mean follow-upwas 7.6±5.0 years.Mean renal survival was 13.5±0.8 years and probability ofdecline≥50%inbaseline eGFRwas 8% atfiveyearsoffollow-up and15% at tenyears.Tenchildren (18.5%)hadadeclineofbaselineeGFR≥50%andfive(9.3%)evolved toend-stagerenaldisease.Kaplan---Meieranalysisshowedthatbaselineproteinuria, protein-uriaduringfollow-up,endocapillaryproliferation,andtubularatrophy/interstitialfibrosiswere associatedwiththeprimaryoutcome.MultivariateCoxanalysisshowedthatonlybaseline pro-teinuria(HR,1.73;95%CI,1.20---2.50,p=0.003)andendocapillaryhypercellularity(HR,37.18; 95% CI,3.85---358.94,p=0.002)were independentpredictorsofrenal dysfunction.No other pathologicalvariablewasassociatedwitheGFRdeclineinthemultivariateanalysis.
夽
Pleasecitethisarticleas:FabianoRC,AraújoSA,BambirraEA,OliveiraEA,SimõeseSilvaAC,PinheiroSV.TheOxfordClassification predictorsofchronickidneydiseaseinpediatricpatientswithIgAnephropathy.JPediatr(RioJ).2017;93:389---97.
∗Correspondingauthor.
E-mail:[email protected](A.C.SimõeseSilva). http://dx.doi.org/10.1016/j.jped.2016.09.003
Conclusion: ThisisthefirstcohortstudythatevaluatedthepredictiveroleoftheOxford Clas-sificationinpediatricpatientswithIgANfromSouthAmerica.Endocapillaryproliferationwas theuniquepathologicalfeaturethatindependentlypredictedrenaloutcome.
©2017SociedadeBrasileiradePediatria.PublishedbyElsevierEditoraLtda.Thisisanopen accessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/licenses/by-nc-nd/
4.0/).
PALAVRAS-CHAVE
NefropatiaporIgA; Glomerulonefrite; Doenc¸arenalcrônica; Proteinúria;
Classificac¸ãode Oxford
Preditoresdadoenc¸arenalcrônicasegundoaClassificac¸ãodeOxfordempacientes pediátricoscomnefropatiaporIgA
Resumo
Objetivo: AClassificac¸ãoOxfordparaaNefropatiaporImunoglobulinaA(IgAN)identificou var-iáveispatológicasderiscoparadisfunc¸ãorenal.Opresenteestudotevecomoobjetivoavaliaras variáveisdaClassificac¸ãodeOxfordcomopreditoresdedisfunc¸ãorenalemcrianc¸asBrasileiras comIgAN.
Métodos: Foramanalisados54pacientescomdiagnósticodeIgANentre1982-2010.Asbiópsias renaisforamreavaliadaspelaClassificac¸ãodeOxford.Foramrealizadasanálisesunie multi-variadadasvariáveisclínicasepatológicas.Odesfechoprimáriofoiquedadataxadefiltrac¸ão glomerular(TFG)≥50%dafiltrac¸ãobasal.
Resultados: Oacompanhamentomédiofoi7,6±5,0anos.Asobrevidarenalmédiafoi13,5±0,8 anoseaprobabilidadedeatingirodesfechoprimáriofoi8%em5anose15%em10anosde seguimento.Dezcrianc¸as(18,5%)apresentaramquedanaTFGbasal≥50%e5(9,3%)evoluiu paradoenc¸arenalcrônicaterminal.AanálisedeKaplan---Meiermostrouqueaproteinúriabasal edeseguimento,aproliferac¸ãoendocapilareaatrofiatubular/fibroseintersticialforam asso-ciadascomodesfechoprimário.AanálisemultivariadadeCoxmostrouqueaproteinúriabasal (HR=1.73; IC95% 1.20-2.50,p=0.003)ea proliferac¸ãoendocapilar(HR=37.18;IC95% 3.85-358.94,p=0.002)forampreditoresindependentesdedisfunc¸ãorenal.Nenhumaoutravariável patológicafoiassociadacomdeclíniodaTFGnaanálisemultivariada.
Conclusão: EsteéoprimeiroestudobrasileiroqueavaliouaClassificac¸ãoOxfordemcrianc¸as comIgAN.A proliferac¸ãoendocapilarfoiaúnica característicapatológicacapazdepredizer independentementeodeclíniodafunc¸ãorenal.
©2017SociedadeBrasileiradePediatria.PublicadoporElsevierEditoraLtda.Este ´eumartigo OpenAccesssobumalicenc¸aCCBY-NC-ND(http://creativecommons.org/licenses/by-nc-nd/4.
0/).
Introduction
IgA nephropathy (IgAN) is one of the leading causes of glomerulonephritis worldwide. The predominant/co-dominantpresence of IgA1 in mesangial immune deposits is essential todiagnose IgAN.1 IgAN is characterized by a
highlyvariablecourse,extendingfromaverymilddisease2
toend-stagerenaldisease(ESRD).3Thediseaseusually
pro-gresses insidiously and the search for predictors of renal outcomemayenableindividualizeddecision-making,early patientcare,andappropriatetreatmentwithlessadverse effects.4---6
In this regard, the analysis of kidney tissue may also contributeadditionalprognosticinformation. In 2009,the International IgA Nephropathy Network developed the Oxford Classification, in which four histological variables with prognostic importance were identified as predictors of renal outcome in IgAN patients (MEST score): mesan-gial hypercellularity (M), endocapillary proliferation (E), segmental sclerosis or adhesion (S), and tubular atro-phy/interstitial fibrosis (T).7,8 The Oxford Classification
encompasses analysis of data from patients with a wide rangeof age.The predictive value ofeach specific lesion
onrenalsurvivalappearednottobedistinctbetween chil-drenandadultswithIgANintheOxfordClassificationstudy.9
Incontrast,previousstudieshadshownthatthehistological featuresofIgANinchildrenandadultsweredifferent.10---13
Compared with adults,children with IgAN showed signifi-cantlymoremesangialandendocapillaryproliferationand less chronic tubulointerstitial and vascular damage.10---13
OnlythreestudiesassessedtheperformanceoftheOxford Classificationexclusivelyinpediatricpatients.14---16Leetal.
reported that tubularatrophy/interstitial fibrosis was the onlyfeatureindependentlyassociatedwithrenaloutcomes in Chinese children with IgAN.15 In the Swedish study,
mesangial hypercellularity, endocapillary proliferation, or tubular atrophy/interstitial fibrosis were each associated withapoor outcome,but segmentalsclerosisor adhesion didnotreachstatisticalsignificance.14 TheJapanesestudy
showedthatonlymesangialhypercellularityscore,tubular atrophy,andcrescentsweresignificantpredictors ofrenal outcome.16 Hence, whether the classification system has
the predictive value of clinical, laboratory, and the four histologicalvariables ofthe OxfordClassification onrenal outcomeinacohortofBrazilianpediatricpatients.
Patients
and
methods
Patients
The records of 54 patients withbiopsy-proven IgAN were includedin theanalysisof thisretrospectivecohortstudy. Inclusion criteria were patients between 2 and 18 years ofagewithbiopsy-provenIgANwhowereadmittedtothe PediatricNephrology Unit(PNU), ClinicsHospital, Federal Universityof MinasGerais,Brazil, from1982 to2010, and hadat least nine monthsof follow-up. Diagnosticcriteria forIgANwerebasedonthefindingofdominant/codominant mesangialdepositionofIgAonimmunofluorescenceof kid-ney tissue.17 This PNU was established in 1969 and has
followed-up numerous children with IgAN according to a well-established protocol. Briefly, the protocol included investigation of disease etiology, assessment of clinical courseandlaboratoryalterations,andapplicationof treat-ment according to international guidelines.18 Pediatric
patientsadmittedtothePNUwithestimatedglomerular fil-tration rate (eGFR) below 60mL/min/1.73m2 or who had Henoch-Schönlein purpura, diabetes, or liver or systemic diseaseswereexcludedfromanalysis.
Ethicalaspects
The local ethics committee approved the study (CAAE 18196713.4.0000.5149). Informed consent was obtained fromallparentsorpersonslegallyresponsibleforpediatric patientswithIgAN.Theresearchprotocoldidnotinterfere withanymedicalrecommendationsorprescriptions.
Baselineandfollow-upcovariates
The date of renal biopsy was considered the base-line time point. The follow-up period was calculated as the time between renal biopsy and last outpatient visit, death, or 50% reduction of baseline eGFR. Varia-bles included in the analysis were: sex, ethnicity, age at baseline, eGFR, proteinuria, hypertension, weight-for-age Z-score, height-for-age Z-score, body mass index (BMI), and serum levels of creatinine. In order to avoid the overestimation of weight in patients with edema, only the dry weight was considered for the variables weight and BMI. Treatment was also evaluated accord-ing to medical prescription, regardless the duration of use.Renin-angiotensin system blockers(RASB)referred to prescription of angiotensin-converting enzyme inhibitors (ACEi) and/or angiotensin receptor blockers (ARB), and immunosuppressive drugs included corticosteroids and cyclophosphamide.
Histologicstudies
Renalbiopsywasperformedinall54children.Lessthan one-thirdofthecohort(29%)wasbiopsiedbefore1990.Biopsies
werere-examined by a single renalpathologist, who was blinded topatient outcome at the timeof scoring. Biop-sieswereanalyzedbasedon2gperiodicacidSchiff-stained
sections.Nospecimenshadlessthansixglomeruli. Biopsy specimens were classified and standardized according to the Oxford Classification,7,8 in which the
number of glomeruli was assessed and their mesangial hypercellularity (M) scored as ≤0.5 or >0.5, if more or less than half of the glomeruli showed hypercellularity, defined as four or more mesangial cells/mesangial area, endocapillaryproliferation(E,absentorpresent), segmen-tal glomerulosclerosis (S, absent or present), andtubular atrophy/interstitial fibrosis (T, 0=0---25%, 1=26---50%, and 2=>50%).Glomeruliwithcellularandfibrocellularcrescents andarterialintimalthickeningwerealsodetermined.
Definitions
Bloodpressure wasmeasured and evaluatedaccording to theFourthTaskForceonBloodPressure inChildren19 and
the95thpercentilewasusedasthecutoffpoint. Protein-uria was expressed in grams per day per 1.73m2. When 24-hurineproteinmeasurementswerenotavailable,urine protein-to-creatinine ratio (uP/Cr) was used to estimate 24-h urine protein excretion by adjusting the values for bodysurfacearea.16Absenceofproteinuriaormild
protein-uriawasconsideredwhenbelow1g/day/1.73m2or uP/Cr lowerthan1g/g.Moderateproteinuriawasdefinedasa non-nephroticproteinuriaofmorethan1g/day/1.73m2oruP/Cr between 1 and 3g/g. Severe or nephrotic range protein-uria wasconsidered whenabove3g/day/1.73m2 or when uP/Cr>3g/g.9,16 For each year of follow-up, the average
valueforallmeasurementsofproteinuriawasdetermined. The variable proteinuria during follow-up was the mean of all annual average values. Hematuria was diagnosed whenfive or more red blood cells were found in at least two urinary sediment exams. Weight-for-age and height-for-ageZ-scores were used toassess weight and stature. These measures were calculated using the public-domain softwareEpiInfo(version3.4.1).Sincecreatinine measure-mentsweremadebyJaffemethoduntilNovember2011in thisinstitution,glomerularfiltrationratewasestimatedby theconventional formula of Schwartz20 for data obtained
until this period. Accordingly, the value for the constant (K) was0.55for children under13 yearsoldand for ado-lescentgirls.Foradolescentboysatleast13yearsofage, the K value was 0.70. After November 2011, creatinine wasmeasured by IDMS (isotope dilution mass spectrome-try) traceable method. Therefore, the modified Schwartz formula21wasadoptedtoestimateGFRratherthanthe
con-ventionalSchwartzformula.
Outcome
Statisticalanalysis
Statisticalanalysiswasperformedusing(SPSSStatistics, ver-sion 19.0, IL, USA). Continuous variables were expressed as mean±SD. Categorical variables were described as percentages and analyzed using Pearson’s chi-squared test. Student’s t-test (normallydistributed variables) and Mann---WhitneyorKruskal---Wallis(nonparametricvariables) were used to compare continuous variables. Univariate analysisof continuous variables wasperformed usingCox regression, whereas categorical variables were analyzed using Kaplan---Meier and log-rank methods. Variables at baselineincluded in theunivariate analysiswere: gender, ethnicity,ageatbaseline,hypertension,andhistopathology features.Laboratory testsatbaseline werealsoincluded: eGFR,serumcreatinine,andproteinuria. TheCox propor-tionalhazardsmodelwasappliedtoidentifyvariablesthat wereindependentlyassociatedwithadecline≥50% from baseline eGFR. Only variables that were associated with theeventofinterestbyunivariateanalysis(p<0.25)were includedinthemultivariateCoxregression.Allreportedp -valueswere twosided.Values of p lower than 0.05were consideredstatisticallysignificant.Confidenceintervals(CI) included95%ofthepredictedvalues.
Results
Clinicalandpathologicalcharacteristics
Atotalof 54patients (31boys)withIgAN wereanalyzed. The majority were classified as white (51.9%). The mean agewas9.7±3.3years.Atthetimeofrenalbiopsy,mean eGFR was 143±49.7mL/min/1.73m2. The mean baseline
proteinuriawas0.97±1.93g/dayper1.73m2.Fourpatients
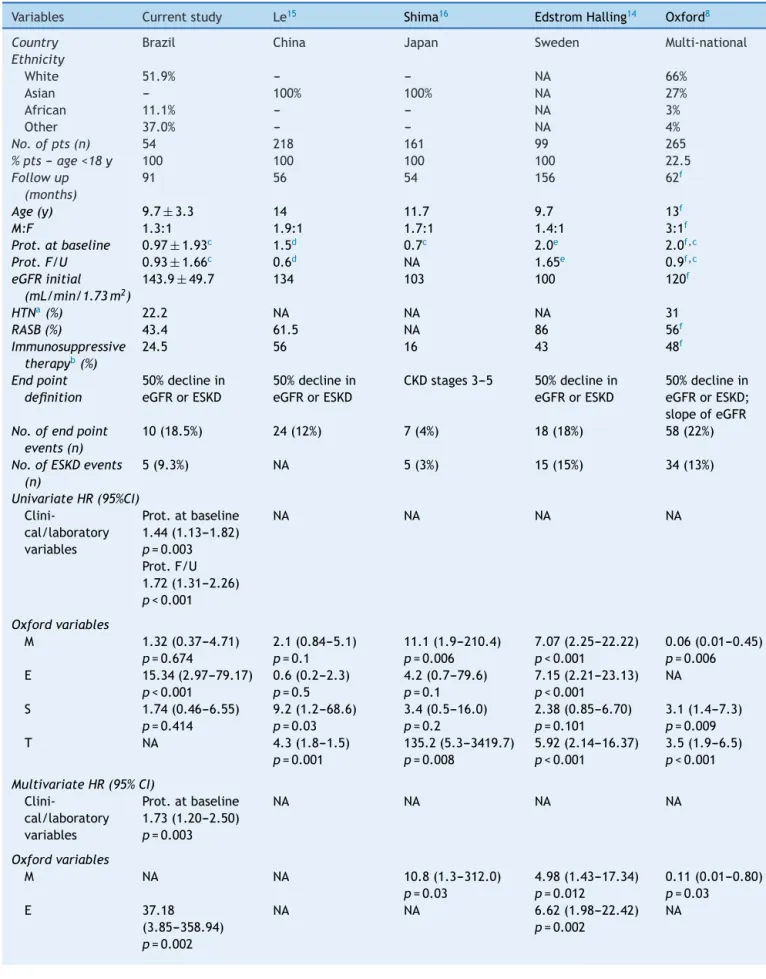
(7.4%)hadbaselineproteinuriainthenephroticrangeand sixpatients (11.1%)presented withmoderateproteinuria. Twelvepatients (22.2%)hadarterialhypertension orwere receiving antihypertensive therapy at the time of renal biopsy.Table1summarizesclinicalanddemographicdataat thetimeofrenalbiopsy.Thesefindingswerealsocompared withfourotherpediatriccohortstudies.
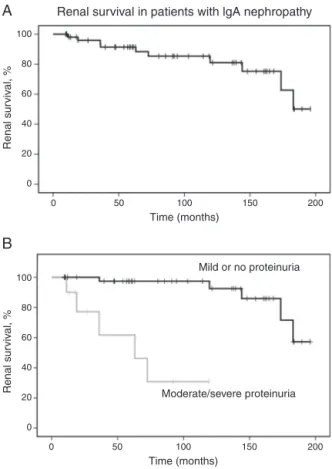
The mean follow-up time was 90±60 months. Of all patients,ten(18.5%)developed50%declineinrenal func-tion,withmeanendpointeGFRof70±43mL/min/1.73m2. Fivepatients(9.3%)developedESRDin109±85months. Sur-vivalanalysisestimatedthattheprobabilityof50%decline in renal function was 8% at five years and 15% at ten years. Laboratory evaluation at last visit revealed mean eGFRof143.9±49.7mL/min/1.73m2 forpatientswhodid notachievetheprimaryoutcome.Renalsurvivalanalysisis showninFig.1.
Pathologicalanalysisshowedameanof23glomeruliper biopsy.Therewere18patientswithmesangialproliferation (M1),fivepatientswithendocapillaryproliferation(E1),13 patientswithsegmentalsclerosis/adhesionlesion(S1),and onlytwopatientswithtubulointerstitialfibrosis,moderate in one(T1) and severe in theother (T2).Due tothe low frequencyoftubulointerstitialfibrosis,T1andT2were com-binedforthefollowinganalysis.Thefrequencyofcrescents wasalsolow(7.4%)andvascularlesionswerefoundinjust
100
80
60
40
20
0
0 50 100
Renal survival in patients with lgA nephropathy
A
B
Time (months)
Renal sur
viv
al, %
150 200
100
80
60
40
20
0
0 50 100
Time (months)
Moderate/severe proteinuria Mild or no proteinuria
Renal sur
viv
al, %
150 200
Figure 1 Renal survival in patients with IgA nephropathy.
(A)Kaplan---Meiercurvesshowtheprobabilityofrenalsurvival (declineofbaselineeGFR≥50%)forpatientswithIgA nephropa-thy(n=54).(B)Kaplan---Meiercurvesshowthelowerprobability of renal survival for patients with moderate to severe pro-teinuria (n=10) as compared with patients with mild or no proteinuria(n=44).eGFR,estimatedglomerularfiltrationrate.
onecase. Vascularlesionswere notincluded in statistical analysis.
Associationsbetweenpathologicallesions,baseline clinicalfeatures,andtreatment
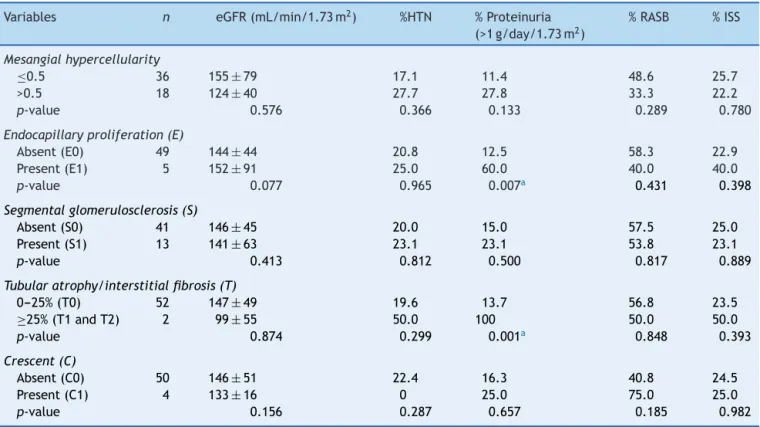
Possibleassociationsbetweenclinicalfindings,therapeutic approach, and renal histology of the patients are shown in Table 2. None of the lesions were significantly asso-ciated with eGFR or hypertension at the time of biopsy. Endocapillaryproliferationandtubularatrophy/interstitial fibrosis(≥25%)wereassociatedwithmoderate/severe pro-teinuria atbaseline.Mesangialhypercellularity,segmental glomerulosclerosis,andextracapillaryhypercellularitywere notassociatedwithanyoftheclinicalfeatures.The thera-peuticapproachwithRASBandimmunosuppressorswasnot significantlyassociatedwithpathologicalvariables.
Survivalanalysis
Table1 Clinicalvariablesatthetimeofinitialbiopsyandtheendpointoffollow-up.Comparisonofcurrentdatawithother pediatriccohortstudies.
Variables Currentstudy Le15 Shima16 EdstromHalling14 Oxford8
Country Brazil China Japan Sweden Multi-national
Ethnicity
White 51.9% --- --- NA 66%
Asian --- 100% 100% NA 27%
African 11.1% --- --- NA 3%
Other 37.0% --- --- NA 4%
No.ofpts(n) 54 218 161 99 265
%pts--- age<18y 100 100 100 100 22.5
Followup (months)
91 56 54 156 62f
Age(y) 9.7± 3.3 14 11.7 9.7 13f
M:F 1.3:1 1.9:1 1.7:1 1.4:1 3:1f
Prot.atbaseline 0.97± 1.93c 1.5d 0.7c 2.0e 2.0f,c
Prot.F/U 0.93±1.66c 0.6d NA 1.65e 0.9f,c
eGFRinitial (mL/min/1.73m2)
143.9± 49.7 134 103 100 120f
HTNa(%) 22.2 NA NA NA 31
RASB(%) 43.4 61.5 NA 86 56f
Immunosuppressive therapyb(%)
24.5 56 16 43 48f
Endpoint definition
50%declinein eGFRorESKD
50%declinein eGFRorESKD
CKDstages3---5 50%declinein eGFRorESKD
50%declinein eGFRorESKD; slopeofeGFR No.ofendpoint
events(n)
10(18.5%) 24(12%) 7(4%) 18(18%) 58(22%)
No.ofESKDevents (n)
5(9.3%) NA 5(3%) 15(15%) 34(13%)
UnivariateHR(95%CI)
Clini-cal/laboratory variables
Prot.atbaseline 1.44(1.13---1.82) p=0.003 Prot.F/U 1.72(1.31---2.26) p<0.001
NA NA NA NA
Oxfordvariables
M 1.32(0.37---4.71)
p=0.674
2.1(0.84---5.1) p=0.1
11.1(1.9---210.4) p=0.006
7.07(2.25---22.22) p<0.001
0.06(0.01---0.45) p=0.006
E 15.34(2.97---79.17)
p<0.001
0.6(0.2---2.3) p=0.5
4.2(0.7---79.6) p=0.1
7.15(2.21---23.13) p<0.001
NA
S 1.74(0.46---6.55)
p=0.414
9.2(1.2---68.6) p=0.03
3.4(0.5---16.0) p=0.2
2.38(0.85---6.70) p=0.101
3.1(1.4---7.3) p=0.009
T NA 4.3(1.8---1.5)
p=0.001
135.2(5.3---3419.7) p=0.008
5.92(2.14---16.37) p<0.001
3.5(1.9---6.5) p<0.001 MultivariateHR(95%CI)
Clini-cal/laboratory variables
Prot.atbaseline 1.73(1.20---2.50) p=0.003
NA NA NA NA
Oxfordvariables
M NA NA 10.8(1.3---312.0)
p=0.03
4.98(1.43---17.34) p=0.012
0.11(0.01---0.80) p=0.03
E 37.18
(3.85---358.94) p=0.002
NA NA 6.62(1.98---22.42)
p=0.002
Table1 (Continued)
Variables Currentstudy Le15 Shima16 EdstromHalling14 Oxford8
S NA NA NA NA NA
T NA 2.9(1.0---7.9)
p=0.04
91.7(3.3---2676.4)
p=0.01
4.22(1.48---12.03)
p=0.007
5.0(2.3---11.1)
p<0.001
CI,confidenceinterval;CKD,chronickidneydisease;E,endocapillaryhypercellularity;eGFR,estimatedglomerularfiltrationrate;ESKD, endstagekidneydisease;F/U,follow-up;HR,Hazardratio;HTN,hypertension;M,mesangialhypercellularity;M:F,male:female;NA, notavailable;prot,proteinuria;pts,patients;RASB,renin---angiotensin-systemblockade;S,segmentalglomerulosclerosis;T,tubular atrophy/interstitialfibrosis.
aEitherpresenceofhypertensionoruseofantihypertensivemedicationsatinitialevaluation. b Eithersteroidsorotherimmunosuppressivemedicine.
c Proteinuriaexpressedasgofprotein/day/1.73m2. d Proteinuriaexpressedasgofprotein/day.
e Albuminuriaexpressedasmgofalbumin/mgofcreatinine. f Datarestrictedtochildren.
Table2 Associationbetweenpathologicalandclinicalvariablesatthetimeofrenalbiopsy.
Variables n eGFR(mL/min/1.73m2) %HTN %Proteinuria
(>1g/day/1.73m2)
%RASB %ISS
Mesangialhypercellularity
≤0.5 36 155±79 17.1 11.4 48.6 25.7
>0.5 18 124±40 27.7 27.8 33.3 22.2
p-value 0.576 0.366 0.133 0.289 0.780
Endocapillaryproliferation(E)
Absent(E0) 49 144±44 20.8 12.5 58.3 22.9
Present(E1) 5 152±91 25.0 60.0 40.0 40.0
p-value 0.077 0.965 0.007a 0.431 0.398
Segmentalglomerulosclerosis(S)
Absent(S0) 41 146±45 20.0 15.0 57.5 25.0
Present(S1) 13 141± 63 23.1 23.1 53.8 23.1
p-value 0.413 0.812 0.500 0.817 0.889
Tubularatrophy/interstitialfibrosis(T)
0---25%(T0) 52 147±49 19.6 13.7 56.8 23.5
≥25%(T1andT2) 2 99± 55 50.0 100 50.0 50.0
p-value 0.874 0.299 0.001a 0.848 0.393
Crescent(C)
Absent(C0) 50 146± 51 22.4 16.3 40.8 24.5
Present(C1) 4 133±16 0 25.0 75.0 25.0
p-value 0.156 0.287 0.657 0.185 0.982
eGFR,estimatedglomerularfiltrationrate;HTN,hypertension;RASB,renin-angiotensin-systemblockade;ISS,immunosuppressive ther-apy.
Valuesareexpressedasmean±SDforeGFRandasproportionforHTN,proteinuria,RASB,andISS. ap<0.05.
variables of the Oxford Classification, Kaplan---Meier revealed that endocapillary hypercellularity (chi-squared 18.52; p<0.001, log-rank [Mantel---Cox]), and tubular atrophy/interstitial fibrosis (chi-squared 62.96; p<0.001, log-rank[Mantel---Cox])wereassociatedwithrenalsurvival. Mesangial hypercellularity (chi-squared 0.18; p=0.673, log-rank[Mantel---Cox]),segmentalglomerulosclerosis (chi-squared 0.68; p=0.409, log-rank [Mantel---Cox]), and extracapillaryhypercellularity(chi-squared1.11;p=0.292, log-rank [Mantel---Cox]) were not associated with primary outcome.Fig.2showsrenalsurvivalbyKaplan---Meier anal-ysisaccordingtotheOxfordClassification.
100
80
60
40
20
0
0 50 100
Mesangial hypercellularity
Renal survival in patients with lgA nephropathy according
to the Oxford Classification
A
Time (months)
M1 M0
E0
E1
T1/T2
T0 S0
S1
Renal sur
viv
al, %
150 200
100
80
60
40
20
0
0 50 100
Endocapillary proliferation
B
Time (months)
Renal sur
viv
al, %
150 200
100
80
60
40
20
0
0 50 100
Segmental glomerulosclerosis
C
Time (months)
Renal sur
viv
al, %
150 200
100
80
60
40
20
0
0 50 100
Tubular atrophy/interstitial fibrosis
D
Time (months)
Renal sur
viv
al, %
150 200
Figure2 RenalsurvivalofpatientswithIgAnephropathyaccordingtotheOxfordClassification.(A)Kaplan---Meiercurvesshow
thesameprobabilityofrenalsurvival(declineofbaselineeGFR≥50%)forpatientswithmesangialhypercellularityM1(n=18)and withoutmesangialhypercellularityM0(n=36).(B)Kaplan---Meiercurvesshowthelowerprobabilityofrenalsurvivalforpatientswith endocapillaryproliferationE1(n=5)ascomparedwithpatientswithoutendocapillaryproliferationE0(n=49).(C)Kaplan---Meier curvesshowthesameprobabilityofrenalsurvivalforpatientswithsegmentalglomerulosclerosisS1(n=13)andwithout segmen-talglomerulosclerosisS0(n=41).(D)Kaplan---Meiercurvesshowthelowerprobabilityofrenalsurvivalforpatientswithtubular atrophy/interstitialfibrosis≥25%T1orT2(n=2)ascomparedwithpatientswithtubularatrophy/interstitialfibrosisequalorlower than25%T0(n=52).eGFR,estimatedglomerularfiltrationrate.
diagnosis,butsignificancewasnotfoundduetosmall num-berofpatients withtubulointerstitialfibrosis(n=2).Also, mesangial hypercellularity (HR 1.32; 95% CI, 0.37---4.71,
p=0.674),segmental glomerulosclerosis(HR1.74;95% CI, 0.46---6.55,p=0.414)andextracapillaryhypercellularity(HR 0.04; 95%CI, 0.00---416.77, p=0.497) werenot associated with primary outcome. No other variable was associated withprimaryoutcome.
Baseline variables associated with the renal survival were proteinuria at the time of first renal biopsy and endocapillary hypercellularity. In multivariate Cox analy-sis,afteradjustmentbyCoxregressionmodel,proteinuria atbaseline(HR,1.73;95%CI,1.20---2.50,coefficient 0.55;
p=0.003)andendocapillaryhypercellularity(HR,37.18;95% CI, 3.85---358.94, coefficient 3.62; p=0.002) remained as independentpredictorsofthedeclineofbaselineeGFRof atleast50%.
Discussion
This study investigated possible predictive factors asso-ciated with decline of eGFR in pediatric patients with
IgAN. The main findings were related to the prognos-ticrole of proteinuria and of endocapillary proliferation. Therefore,childrenwhohadadeclineof50%ineGFR pre-sentedhigher levelsof proteinuriaat baseline andduring follow-up. On the other hand, patients with mild or no proteinuria had better renalsurvival compared with chil-drenwithmoderate/severeproteinuria.Thesefindingsare consistent with recent results showing a good prognosis for patients with mild proteinuria.22---24 Among
As shown in Table 1, only three studies adopting the OxfordClassificationwerepreviouslypublishedexclusively with pediatric patients.14---16 Compared with Chinese,15
Swiss,14 and original Oxford8 cohorts, the present
sam-pleis verysimilar.As expected,highproportionsofmales and of white children (51.9%) among IgAN patients were observed.Althoughtherearecleargeographicalandethnic differences,IgANis morecommon inAsianandCaucasian children.12Itshouldbepointedoutthatallofthepatients
had a baseline eGFR above 60mL/min/1.73m2. In addi-tion, they presented less severe baseline proteinuria. In comparisontotheOxfordcohort,fewerpatientsexhibited nephrotic range proteinuria at baseline (7.4%). Further-more, the number of patients with no medication during followup(RASBorimmunosuppressivetherapy)seemedto be higher in the present cohort. Accordingly, only eight patientsreceivedcorticosteroids,andonewasalsotreated withcyclophosphamide. These findings may indicate that thiscohortincluded mildercases ofIgAN thanthe Oxford study.In agreement, the lowerincidence of primary out-comeinthiscohort(18.5%vs.22%intheOxfordstudy)might beexplainedat least inpart by theoccurrence ofmilder casesofIgAN.
In regard to histological variables in exclusively pedi-atricstudies, EdströmHallingetal.found that segmental glomerulosclerosis(S)wasnotassociatedwiththe progres-sion of IgAN in the Swiss cohort of 99 children.14 Shima
etal. examined 161 children in Japan and reported that only mesangial hypercellularity (M) and interstitial fibro-sis/tubular atrophy (T) are prognostic markers in that population.16 In China, the analysis of a 218 children
revealedthatonly Tremains asaprognosticmarkerafter multivariate analysis.15 Two other large adult cohorts of
IgANalsoincludedpediatricpatients.22,23Herzenbergetal.
evaluated187 NorthAmerican patients including45 chil-dren and observed that each histological variable has the same predictive value found in Oxford original stud-ies, except M, which behaves as a weaker predictor.22
More recently, theEuropean study VALIGA retrospectively analyzed 1147 European patients, including 174 children. Segmentalglomerulosclerosis(S),mesangial hypercellular-ity (M), tubular atrophy/interstitial fibrosis (T), but not endocapillary proliferation (E), were identified as predic-tors of renal outcome in this cohort.23 More recently, a
retrospective study from Great Britain showed that pro-teinuria, endocapillary proliferation (E1 versus E0), and interstitial fibrosis/tubular atrophy (T2 versus T0) were ableto predict ESRD in a cohort of 147 adults withIgAN receivingnoimmunosuppression.25 Similarly,proteinuriaat
baselineandendocapillaryproliferationinrenaltissue pre-dicted renal function deterioration in the present study. Ontheotherhand,theOxfordClassificationstudyshowed no significance of E as a predictor of renal survival in children.9 Endocapillary proliferation probably interacted
with immunosuppressive therapy in IgAN patients.9 The
samewasobservedintheVALIGAstudy.23 Inametanalysis
withIgANcohorts,Ewasnotrelatedtotheoutcomeeither.3
Itshouldbepointedoutthatrecentstudieshaveshoweda benefitofimmunosuppressivetherapyonglomerular endo-capillaryproliferation inpatients withIgAN.22 Shen etal.
reportedthatendocapillaryproliferationcouldbereversed byimmunosuppressivetherapyinpatientswithIgAN.26 The
reversaloftheselesionsmayexplainthelackofcorrelation of these lesions with clinical outcomes.26 Although
endo-capillary proliferation is nota uniform predictor of renal dysfunctionintheOxfordvalidationstudieswithchildren, the present study showed that this variable may predict renaldysfunctioninIgANchildrenwithlessseveredisease andlowlevelsofimmunosuppression.
It is noteworthy that the present study evaluated, for thefirsttime,theperformanceofOxfordClassificationina cohortofpediatricpatientsfromSouthAmerica.However, thisstudydidnotaimtovalidatetheOxfordClassificationin SouthAmericanchildrenwithIgA.Rather,theobjectivewas todescriberiskfactorsassociatedwiththedeclineofrenal functionin Brazilianpediatric patientswithIgAN.In addi-tion,thelimitationsofthisstudymustberecognized.First, theretrospectivedesignmadedifficultthecontroloverthe variables measured. Second, the small sample size might contributetothelackofpredictive valueforsome patho-logicalvariables.Third,itwasnotpossibletosystematically analyze some time-dependent variables, including hyper-tension.However,somefeaturesofthisstudymayincrease thestrengthofthesefindings,includingthelargesetofdata collectedovermany yearsandlong-term follow-upbythe sameteamwithawell-establishedclinicalprotocol,aswell asthecarefulre-evaluationofallrenalbiopsiesbyasingle expertpathologistblindedtoclinicaldataandoutcome.
In conclusion, endocapillary proliferation in renal tis-sue was the single pathological variable independently associated with renal outcome in this Brazilian pedi-atric IgAN cohort. Proteinuria at baseline was also of prognostic relevance. However, the low prevalence of other histopathological lesions --- particularly segmental glomerulosclerosis,interstitialfibrosis/tubularatrophy,and extracapillaryhypercellularity---hamperedtheappraisalof theirvalue.Althoughtheresultscertainlyrequire confirma-tion by other South Americanpediatric IgANcohorts, the adoptionoftheOxfordClassificationmayenablethe com-parisonofpathologicalvariablesbetweendifferentstudies.
Funding
Fundac¸ãodeAmparoàPesquisadoEstadodeMinasGerais, Brazil (FAPEMIG), Conselho Nacional de Desenvolvimento CientíficoeTecnológico,Brazil(CNPq),andCoordenac¸ãode Aperfeic¸oamentodePessoaldeNívelSuperior(CAPES).
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgements
References
1.Wyatt RJ, Julian BA. IgA nephropathy. N Engl J Med. 2013;368:2402---14.
2.Gutiérrez E, Zamora I, Ballarín JA, Arce Y, Jiménez S, QueredaC,etal.Long-termoutcomesofIgAnephropathy pre-sentingwith minimal or no proteinuria. J Am Soc Nephrol. 2012;23:1753---60.
3.LvJ, Shi S, Xu D, Zhang H, Troyanov S, Cattran DC, et al. Evaluation of the Oxford Classification of IgA nephropathy: a systematic review and meta-analysis. Am J Kidney Dis. 2013;62:891---9.
4.Tangri N, Stevens LA, Griffith J, Tighiouart H, Djurdjev O, NaimarkD,etal.Apredictivemodelforprogressionofchronic kidneydiseasetokidneyfailure.JAMA.2011;305:1553---9. 5.TaalMW,BrennerBM.Renalriskscores:progressandprospects.
KidneyInt.2008;73:1216---9.
6.TaalMW,BrennerBM.Predictinginitiationandprogressionof chronickidneydisease:developingrenalriskscores.KidneyInt. 2006;70:1694---705.
7.WorkingGroupoftheInternationalIgANephropathy Network andtheRenal PathologySociety,RobertsIS, CookHT, Troya-novS,AlpersCE,AmoreA,etal.TheOxfordClassificationof IgAnephropathy:pathologydefinitions,correlations,and repro-ducibility.KidneyInt.2009;76:546---56.
8.WorkingGroupoftheInternationalIgANephropathy Network andtheRenalPathologySociety,CattranDC,CoppoR,CookHT, FeehallyJ,Roberts IS,etal.TheOxfordClassificationofIgA nephropathy:rationale, clinicopathological correlations, and classification.KidneyInt.2009;76:534---45.
9.WorkingGroupoftheInternationalIgANephropathy Network andtheRenalPathologySociety,CoppoR,TroyanovS,CamillaR, HoggRJ,CattranDC,etal.TheOxfordIgAnephropathy clinico-pathologicalclassificationisvalidforchildrenaswellasadults. KidneyInt.2010;77:921---7.
10.MinaSN,MurphyWM.IgAnephropathy.Acomparativestudyof theclinicopathologicfeaturesinchildrenandadults.AmJClin Pathol.1985;83:669---75.
11.Okada K, Funai M, Kawakami K, Kagami S, Yano I, Kuroda Y. IgA nephropathy inJapanese childrenand adults: a com-parativestudyofclinicopathologicalfeatures.AmJNephrol. 1990;10:191---7.
12.IkezumiY,SuzukiT,ImaiN,UenoM,NaritaI,KawachiH,etal. Histologicaldifferencesinnew-onsetIgAnephropathybetween childrenandadults.NephrolDialTranspl.2006;21:3466---74. 13.HaasM,RahmanMH,CohnRA,Fathallah-ShaykhS,AnsariA,
Bar-toshSM.IgAnephropathyinchildrenandadults:comparisonof
histologicfeaturesandclinicaloutcomes.NephrolDialTranspl. 2008;23:2537---45.
14.EdströmHallingS,SöderbergMP,BergUB.Predictorsof out-comeinpaediatricIgAnephropathywithregardtoclinicaland histopathologicalvariables(OxfordClassification).NephrolDial Transpl.2012;27:715---22.
15.LeW,ZengCH,LiuZ,LiuD,YangQ,LinRX,etal.Validation ofthe OxfordClassification ofIgA nephropathy for pediatric patientsfromChina.BMCNephrol.2012;13:158.
16.Shima Y, Nakanishi K, Hama T, Mukaiyama H, Togawa H, Hashimura Y, et al. Validity of the Oxford Classification of IgA nephropathy in children. Pediatr Nephrol. 2012;27: 783---92.
17.GallaJH.IgAnephropathy.KidneyInt.1995;47:377---87. 18.HoggRJ.IdiopathicimmunoglobulinAnephropathyinchildren
andadolescents.PediatrNephrol.2010;25:823---9.
19.NationalHighBloodPressureEducationProgramWorkingGroup on High Blood Pressure in Children and Adolescents. The fourth reportonthediagnosis,evaluation, and treatmentof high bloodpressure in childrenand adolescents. Pediatrics. 2004;114:555---76.
20.Schwartz GJ, Brion LP,Spitzer A. The use of plasma creat-inine concentrationfor estimating glomerular filtration rate in infants, children, and adolescents. Pediatr Clin N Am. 1987;34:571---90.
21.SchwartzGJ,Mu˜nozA,SchneiderMF,MakRH,KaskelF,Warady BA,etal.NewequationstoestimateGFRinchildrenwithCKD. JAmSocNephrol.2009;20:629---37.
22.Herzenberg AM, Fogo AB, Reich HN, Troyanov S, Bavbek N, MassatAE,etal.ValidationoftheOxfordClassificationofIgA nephropathy.KidneyInt.2011;80:310---7.
23.CoppoR,TroyanovS,BellurS,CattranD,CookHT,FeehallyJ, etal.ValidationoftheOxfordClassificationofIgAnephropathy incohortswithdifferentpresentationsandtreatments.Kidney Int.2014;86:828---36.
24.HigaA,ShimaY,HamaT,SatoM,MukaiyamaH,TogawaH,etal. Long-termoutcomeofchildhoodIgAnephropathywithminimal proteinuria.PediatrNephrol.2015;30:2121---7.
25.ChakeraA,MacEwenC,BellurSS,ChompukLO,LunnD,Roberts IS. Prognostic value of endocapillary hypercellularity in IgA nephropathypatientswithnoimmunosuppression.JNephrol. 2016;29:367---75.