www.jped.com.br
ORIGINAL
ARTICLE
Neonatal
screening:
9%
of
children
with
filter
paper
thyroid-stimulating
hormone
levels
between
5
and
10
IU/mL
have
congenital
hypothyroidism
夽
Flávia
C.
Christensen-Adad
∗,
Carolina
T.
Mendes-dos-Santos,
Maura
M.F.
Goto,
Letícia
E.
Sewaybricker,
Lília
F.R.
D’Souza-Li,
Gil
Guerra-Junior,
André
M.
Morcillo,
Sofia
Helena
V.
Lemos-Marini
UniversidadeEstadualdeCampinas(UNICAMP),FaculdadedeCiênciasMédicas,DepartamentodePediatria,Campinas,SP,Brazil
Received10October2016;accepted10January2017 Availableonline21July2017
KEYWORDS Congenital hypothyroidism; Neonatalscreening; Infant;
Newborn; Thyroiddiseases
Abstract
Objectives: Todeterminetheprevalenceofcongenitalhypothyroidisminchildrenwith filter-paperblood-spotTSH(b-TSH)between5and10IU/mLintheneonatalscreening.
Methods: Thiswasaretrospectivestudyincludingchildrenscreenedfrom2003to2010,with b-TSHlevelsbetween5and10IU/mL,whowerefollowed-upduringthefirsttwoyearsoflife whentherewasnoserumTSHnormalization.Thediagnosisofcongenitalhypothyroidismwas definedasserumTSH≥10IU/mLandstartoflevothyroxinetreatmentupto2yearsofage. Results: Ofthe380,741livebirths,3713(1.04%)hadfilterpaperTSHlevelsbetween5and 10IU/mLand,ofthese,339(9.13%)hadcongenitalhypothyroidism.Ofthese,76.11%ofthe caseswerediagnosedinthefirstthreemonthsoflifeand7.96%between1and2yearsofage. Conclusion: The study showed that9.13% ofthechildren with b-TSHlevelsbetween 5and 10IU/mLdevelopedhypothyroidismandthatinapproximatelyone-quarterofthem,the diag-nosiswasconfirmedonlyafterthethirdmonthoflife.Basedonthesefindings,theauthors suggesttheuseofa5IU/mLcutoffforb-TSHlevelsandlong-termfollow-upofinfantswhose serumTSHhasnotnormalizedtoruleoutcongenitalhypothyroidism.
©2017SociedadeBrasileiradePediatria.PublishedbyElsevierEditoraLtda.Thisisanopen accessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/licenses/by-nc-nd/ 4.0/).
夽
Pleasecitethisarticleas:Christensen-AdadFC,Mendes-dos-SantosCT,GotoMM,Sewaybricker LE,D’Souza-Li LF,Guerra-Junior G, etal.Neonatalscreening:9%ofchildrenwithfilterpaperthyroid-stimulatinghormonelevelsbetween5and10IU/mLhavecongenital
hypothyroidism.JPediatr(RioJ).2017;93:649---54.
∗Correspondingauthor.
E-mail:[email protected](F.C.Christensen-Adad).
http://dx.doi.org/10.1016/j.jped.2017.05.003
PALAVRAS-CHAVE Hipotireoidismo congênito; Triagemneonatal; Lactente;
Recém-nascido; Doenc¸asdaglândula tireoide
Triagemneonatal:9%dascrianc¸ascomTSHempapelfiltroentre5e10UI/mLtêm
hipotireoidismocongênito
Resumo
Objetivos: Determinar aprevalênciadehipotireoidismocongênitoemcrianc¸ascomTSHem papelfiltro(TSH-f)entre5e10UI/mLnatriagemneonatal.
Métodos: Estudoretrospectivoincluindocrianc¸astriadasde2003a2010,comTSH-fentre5 e 10UI/mL,que foram acompanhadas nosdois primeirosanos devida quandonão houve normalizac¸ãodoTSHsérico.OdiagnósticodehipotireoidismocongênitofoidefinidocomoTSH séricoigualousuperiora10UI/mLeiníciodetratamentocomlevotiroxinaatéosdoisanos deidade.
Resultados: Dos380.741nascidosvivostriados,3.713(1,04%)apresentaram TSH-fentre5e 10UI/mLe,destes,339(9,13%)tinhamhipotireoidismocongênito.Destes,76,11%doscasos foramdiagnosticadosnosprimeirostrêsmesesdevidae7,96%entreumedoisanosdeidade. Conclusão: Oestudomostraque 9,13%das crianc¸as comTSH-fentre5e 10UI/mL desen-volveramhipotireoidismoequeemcercadeum quartodelasodiagnósticosóseconfirmou apósoterceiromêsdevida.Combasenestesachados,sugere-seautilizac¸ãodopontodecorte deTSH-fde5UI/mLeoacompanhamentoemlongoprazodoslactentescujoTSHsériconão tenhasenormalizadoparadescartarohipotireoidismocongênito.
©2017SociedadeBrasileiradePediatria.PublicadoporElsevierEditoraLtda.Este ´eumartigo OpenAccesssobumalicenc¸aCCBY-NC-ND(http://creativecommons.org/licenses/by-nc-nd/4. 0/).
Introduction
Congenital hypothyroidism (CH), the most frequent con-genitalendocrinedisorder and oneof the main causes of preventableintellectualdisabilitywithearlydiagnosisand adequatetreatment,wasoneofthefirstdiseasesscreened inneonatalscreening(NS)programs.1---4
TheincidenceofCHbeforethecreationofNSprograms wasestimated at 1:6500,5 but soon after the start of NS programs,it increasedtoapproximately1:3000 to1:4000 live births (LB).6 In recent years, there has been a fur-therincreaseinCHincidenceinseveralpartsoftheworld, ranging from 1:1030 to 1:2679 LB.7---10 This fact is proba-blyassociatedwithan increasein thesurvival ofpreterm newborns,4,7 environmental11 andethnic factors,7 aswell asthereductioninthecutoffvaluesofthyroid-stimulating hormone (TSH) on filter-paper blood-spot (b-TSH) in NS programs.4,12
Initially, higher b-TSH cutoff values were adopted to avoid recalls and excessive costs, with the justification that mild forms of CH would have no consequences for the neurological development.4 However, some authors suggested that therewere insufficient studies to support thishypothesis,4 andthe European Consensus on Congen-ital Hypothyroidism of 2014 highlighted, as the primary objective of NS, the detection of all cases of primary CH.1
Inrecentyears,severalscreening serviceshavechosen tolowerthecutoffvalueofb-TSHtoreducethenumberof casesofundiagnosedCH.4,13---17
With this reduction, several programs reported an increase in the number of children diagnosed with CH throughNSprograms,4,13---17althoughtherehasalsobeenan increaseinthenumberofchildrenwithsuspectedCHand, therefore,ahigherrateofrecall.4,15,16,18
Since2001,theNeonatalScreeningProgramof Universi-dadeEstadualdeCampinas(UNICAMP)hasusedacutoffof 5IU/mLforb-TSHandhasperformedclinicaland labora-tory follow-upforat leastthefirsttwoyearsoflife ofall childrenwhoseserumTSHlevelsdonotnormalize.
Consideringthis context,the aim of thepresent study wastodeterminetheprevalenceofCHinchildrenwith b-TSHlevelsbetween5and10IU/mLintheNS.
Methods
Neonatalscreeningstrategyforcongenital hypothyroidism
UNICAMP’S Neonatal Screening ReferenceService (Servic¸o de Referência em Triagem Neonatal [SRTN]) is currently responsibleforneonatalscreening,diagnosis,and compre-hensivecareofchildrenintheVII(Campinas)andXIV(São João da Boa Vista) Regional Health Departments, regions thathaveapproximately5000LBpermonth.
Sinceitscreation,UNICAMP SRTN hasworked withthe sameteamforthetreatmentandfollow-upofthecases,and thelaboratoryandimaginginvestigationshavealwaysbeen performedattheservicesofUNICAMPhospitalcomplex.
UNICAMP SRTN uses the cutoff value for b-TSH of 5IU/mL in a dried whole-blood sample on filter paper,
equivalentto11IU/mLinserum,andtheanalysesare
per-formed by time-resolved fluorometry (AutoDELFIA---Perkin ElmerLifeSciences,MA,USA).
UNICAMPSRTNusesthefollowingprotocolforthe diag-nosisandtreatmentofCH:childrenwithb-TSH>5IU/mL
or≤0.01IU/mLarecalledinforserumTSHandfree
forage,butlowerthan10IU/mL,aremonitoredthrough
clinical andlaboratory examinationsin UNICAMP SRTNfor thefirsttwoyearsoflifeoruntiltestnormalization.
Those with serum TSH ≥10IU/mL are referred for
follow-up at the Congenital Hypothyroidism Outpatient Clinicof Hospital deClínicas of UNICAMP, where theyare evaluated individually; and those who persist with TSH >10IU/mLorhaveT4Llevels<0.9ng/dLarediagnosedas
having CHand start treatment withsodium levothyroxine (L-T4).
Serum TSH and T4L collections are performed accord-ing to the technical standards of the Clinical Pathology LaboratoryofUNICAMP;theanalysesareperformedby elec-trochemiluminescence,usingTSHandT4Lreferencevalues of0.41---4.5IU/mLand0.9---1.8ng/dL,respectively.
Studydesign
A retrospective study wascarried out using the UNICAMP SRTNdatabase toobtain thenumberof LB screenedfrom April 2003toSeptember 2009.Childrenwithb-TSHvalues between5and10IU/mL insamplescollectedinthefirst
monthoflifewereselected.
PrimaryCHwasconsideredwhenthechildhadserumTSH ≥10IU/mL at anytimeduring thefirsttwoyearsof life,
regardless of T4L concentration, and received treatment withL-T4.
The followinginformationwasobtainedfromthe medi-cal filesof children withCH and b-TSH levelsbetween 5 and 10IU/mL: b-TSH value; age at NS collection;
gen-der; initial, confirmatory TSH and T4L levels, as well as levels at the start of treatment; and age at the start of treatment.
The following definitionsof serumTSH andT4L values were considered for the study: initial test (the first test collectedafterb-TSH);confirmatorytest(thefirsttestfor whichserumTSHwas≥10IU/mLforeachchild);andtest
at the start of treatment (thelast test collectedprior to medicationintroduction).
Statisticalanalysis
DatawereprocessedusingthesoftwareSPSS,(SPSSInc. ver-sion16.0,Chicago,IL,USA).The resultsofthequalitative variablesareshownasabsoluteandrelativefrequencies.
For theTSH andT4L measurements, the median, min-imum, and maximum values, range (total range), and interquartilerange(IQR)weredetermined.Whenassessing TSH concentrations, the use of medians was chosen to avoid upper limit problems (>100IU/mL) for some
results.
Theresultsofthequantitativevariableswereexpressed asmean±standarddeviationormedian(IQR).
TheprevalenceofCHwasdeterminedbasedonthedata ofthestudygroupwiththerespective95%confidence inter-val(CI).TheMann---Whitneytest wasusedforcomparisons inrelationtogender.Ap-value<0.05wasconsidered signif-icantinallanalyses.
Screened (n=380,741)
Positive screening TSH in filter paper > 5 μIU/mL
(n=3,961)
TSH in filter paper > 5 and < 10 μIU/mL (n=3,713)
Congenital hypothyroidism
(n=339) Screening after 30 days
(n=5)
TSH in filter paper ≥ 10 μIU/mL (n=248)
Figure1 Flowchartofthescreeningforcongenital hypothy-roidismfromApril2003toSeptember2009.
Ethicalaspects
ThisprojectwasapprovedbytheResearchEthicsCommittee ofFaculdadedeCiênciasMédicasofUNICAMP.
Results
IntheperiodfromApril 2003toSeptember2009,380,741 LB were screened for CH throughUNICAMP SRTN. A total of3,961newbornswereenrolledtocomplementthe inves-tigation,resultingin a recall frequency of 1.04% (95%CI: 1.01---1.07). Ofthese, 248 (6.26%) had b-TSH≥10IU/mL
and 3,713 (93.74%) had b-TSH between 5 and 10IU/mL
(Fig.1).Usingthecutoffvalueof10IU/mL,therecallrate wouldhavebeen0.07%(95%CI:0.06---0.08).
Afterclinicalandlaboratoryfollow-upofthe3713 chil-drenwithb-TSHlevelsbetween5and10IU/mL,339(206 malesand133females)werediagnosedwithCHandstarted hormonereplacementtherapywithL-T4,whichcorresponds toaCHprevalenceof9.13%(95%CI:8.2---10.1;Fig.1).
Themeanandmedianagesatb-TSHcollectionwere5±4 daysoflifeand3(4)daysoflife,respectively,andatthe ini-tialserumcollection,24±14daysoflifeand20(13)daysof life.Theconfirmatoryexaminationwascollectedatamean ageof77±121daysoflifeandamedianof28(48)daysof life.
AsshowninTable1,despiteborderlinevaluesofb-TSHin theNS(5.01---9.90UI/mL),TSHvaluesatbaselineshoweda largevariationinthestudiedgroup(3.02to>100IU/mL). The initial TSH of 113 children was <10IU/mL, with a median of 7.00 (2.75) IU/mL. Confirmatory TSH in this grouprangedfrom10.00to>100.00IU/mL,withamedian of 11.50 (2.14) IU/mL. The remaining 226 cases had an initial TSH≥10IU/mL, of which 190 initiated treatment immediately; the remaining 36 patients, all with initial TSH<30IU/mLandnormalorhighT4Llevels,were main-tainedwithoutmedication atthefirstmoment, withlater introduction of hormonal replacement due to the persis-tenceofTSHelevation.
Table1 TSHainneonatalscreeningandinitial,confirmatory,andafterstartoftreatmentexams.
n Median IQR Minimum Maximum
Screening 339 6.37 1.78 5.01 9.90
Initial 339 11.50 7.23 3.02 >100.00
Confirmatory 339 12.89 5.06 10.00 >100.00
Treatment 339 13.12 5.30 8.06 >100.00
n,numberofcases;IQR,interquartilerange.
a
IU/mL.
Table2 T4Laintheinitial,confirmatory,andafterstartoftreatmentexams.
n Median IQR Minimum Maximum
Initial 338 1.36 0.34 0.21 2.39
Confirmatory 338 1.30 0.35 0.12 2.35
Treatment 338 1.30 0.34 0.12 2.12
n,numberofcases;IQR,interquartilerange.
ang/dL.
(18.58%)ofthechildrenhadTSHlevels>20IU/mL atthe
startofthetreatment.
No differences were observed in relation to gen-der regarding the values of b-TSH (p=0.073) and initial (p=0.777)andconfirmatory(p=0.376)TSHlevels,aswell aslevelsatthestartoftreatment(p=0.843).
It is noteworthythat 15 of the339 children presented T4Llevelsbelow thereference valuesin the first evalua-tion,with14ofthem showingTSHvalues>15IU/mLand
onlyone,withaTSHvalueof6.06IU/mLatthefirst
col-lection,showedelevationofTSHlevelsabove10IU/mLin
subsequentcollections.Regardingthelastlaboratory eval-uationperformedpriortothestartoftreatment,17ofthe 339hadT4Llevelsbelowthereferencevalue,whereasTSH rangedfrom10IU/mL to>100IU/mL; in13 ofthese17
patients,thevalueswere>20IU/mL(Table2).
No differences were observed regarding gender in the initial(p=0.318)andconfirmatory(p=0.706)T4Lvalues,as wellasinvaluesatthestartoftreatment(p=0.542).
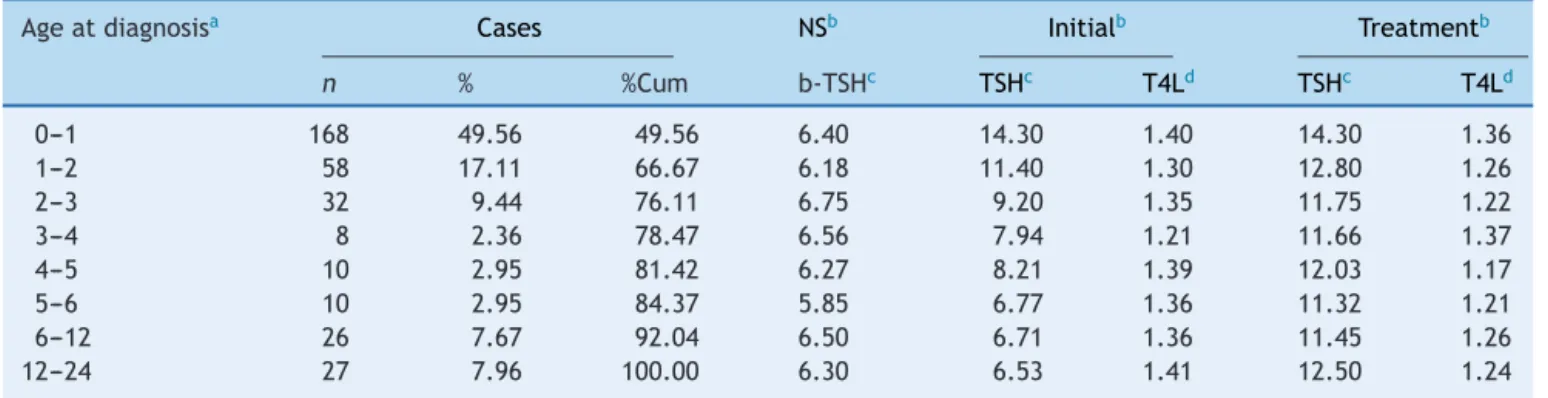
Diagnosiswasconfirmedbetween2and695daysoflife, witha mean of 94±143 days of life and a median of 32 (68),and76.11%ofthechildrenwithCHhadthediagnosis confirmedbeforetheageofthreemonths.However,23.89% ofthe cases thatwould later receive thediagnosis ofCH hadTSHvaluesabovetheupperlimitofnormal,but with noindicationoftreatment,andremainedonfollow-upwith periodic measurementsof TSH and T4L,being defined as having hypothyroidism between 3 and 24 months of age. AmongthesechildrenwithCH,7.96%hadadiagnosis con-firmedbetween1and2yearsofage(Table3).
Discussion
Thisisastudywithasignificantsample,basedonthe expe-rienceofaservice,amongfewinBrazil,14,19,20whichusesa lowerb-TSHcutoffvaluethanmostNSprograms.
The use of alower b-TSHcutoffvalue inthe analyzed sampleresulted in a14.8-foldincrease inthe recallrate, which would be of 0.07% using the cutoff of 10IU/mL,
whereas it was1.04% witha cutoff of 5IU/mL. Another SRTN from Brazil showed a similar recall rate of 1.08%, usingacutoffvalueof4.5IU/mL,14whileKoradaetal.,13 using acutoff value of6mIU/L, reporteda recall rate of 0.23%. Thesedatasuggest that thereis nodirect associa-tionbetweenthecutoffvaluesusedinNSforCHandrecall rates,asconcludedbyLoeber21 intheanalysisof37 Euro-peancountries’NSin2004.
The use of lower cutoff points, with a consequent increaseinthenumberofrecalledchildren,leadstohigher costswithNS,inadditiontogeneratinganxietyforparents andrelativesofhealthychildren.18Duringthestudyperiod, children with b-TSH between 5 and 10IU/mL were sub-mittedtoatleastonevenousbloodcollectiontoevaluate thyroidfunctionand,afterfollow-up,approximately90%of themweredefinedasfalse-positivecases.
However, during the evaluation of these six years of NS with an b-TSHcutoff value of 5IU/mL, 339 children whowouldnothave been detectedwithacutoffpoint of 10IU/mLwerediagnosedwithCH.
OtherNSprogramsalsodetectedadditionalcasesofCH withalowercutoffvalue,asobservedinthestudybyBarone etal.,14inwhich63%ofthe475identifiedcasesofCHhad b-TSHbetween4.5and9.5mIU/L,andinthestudybyKorada etal.,13whichconfirmedtwocasesofCHamongthe67 full-term infants withb-TSHbetween 6and 10mIU/L. One of theSRTNsinthestateofSãoPaulo,whichreducedthe cut-offvalueforb-TSHbetween2005and2008,alsodetected sixcasesofCHamong1181childrenwithinitialb-TSH lev-els between 5 and 10IU/mL.20 Recently, Jones et al.17 observed,amongthe304 diagnosedCHcases,26 children withb-TSHbetween8and10mIU/L.
Therefore, in this study, as well as in others,4,13---17 it hasbeendemonstratedthatchildrenwithCHmightnotbe detectedwiththehighercutoffpointsthatareusuallyused, andtheseadditionaldiagnosedcasesjustify,inthepresent authors’opinionandinthatofotherauthors,thereduction inthecutoffvalueofb-TSH.4,13
Table3 Thyroidfunctionaccordingtoagerangeatdiagnosis.
Ageatdiagnosisa Cases NSb Initialb Treatmentb
n % %Cum b-TSHc TSHc T4Ld TSHc T4Ld
0---1 168 49.56 49.56 6.40 14.30 1.40 14.30 1.36
1---2 58 17.11 66.67 6.18 11.40 1.30 12.80 1.26
2---3 32 9.44 76.11 6.75 9.20 1.35 11.75 1.22
3---4 8 2.36 78.47 6.56 7.94 1.21 11.66 1.37
4---5 10 2.95 81.42 6.27 8.21 1.39 12.03 1.17
5---6 10 2.95 84.37 5.85 6.77 1.36 11.32 1.21
6---12 26 7.67 92.04 6.50 6.71 1.36 11.45 1.26
12---24 27 7.96 100.00 6.30 6.53 1.41 12.50 1.24
n,numberofcases;NS,neonatalscreening;%Cum,cumulativerelativefrequency.
a Months.
b Valuespresentedasmedian. c
IU/mL.
d ng/dL.
belowthereferencevalue,forwhomimmediatetreatment isrecommended.1
It is not yet clear in the literature whether patients with mild elevations in TSH levels are at risk for cogni-tiveimpairment.4,5,8,22 Ithasbeensuggestedthatcasesof neurologicaldisordersthatresultindecreased school per-formance are related to mild forms of CH, not detected by NS due to elevated b-TSH cutoff values.4,23 A recent study showed thatchildren with b-TSHbetween the 75th and99.95thpercentilesaremorelikelytohavepoorschool performance, when comparedto those withb-TSH below the 75th percentile.24 Thus, many have argued that until thereisevidenceofabsenceofriskofintellectual disabil-itywithouttheuseofL-T4,thetreatmentofthesecasesis preferable.4,25
Althoughmostof thegroupwasdiagnosedwithCHand started treatment early, many children who remained on follow-upduetonon-normalizationofTSHvaluesdeveloped hypothyroidismbetween3monthsand2yearsofage.
Onefactorpossiblyinvolvedinthelateconfirmationof CH is breastfeeding, sincebreast milk may be an exoge-nous source of T4, sometimes evenmasking clinical signs of CH.26,27 There is a chance that, given the usual rec-ommendation of exclusive breastfeeding until the sixth month,somechildrenwithmildCHmayhaveshownamore marked elevation in TSH levels after weaningor reduced breastfeeding. Anotherpossibility is that theyare due to thyroid hormone synthesis defect that often take some time for hypothyroidism to be established, as previously reported.28
Inbrief,theresultsofthisstudydemonstratedthatthe use of the b-TSHcutoff value of 5IU/mL in NS allowed thedetectionofadditionalCHcasesandmanyofthese chil-drenonlyhadthediagnosisconfirmedlater.Consideringthat among the different countries and even within the same countrythereis nohomogeneity in diagnosticand follow-upcriteria, morestudies are needed toprovide evidence for an ideal cutoffvalue for b-TSHand toestablish more specific diagnosticandtreatment protocols.1,4,29 Basedon the findingsof thepresent study, theauthors suggest the useofacutoffvalueof5IU/mLandlong-termfollow-up forthesechildren,aimingtodetectallCHcases.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgements
Topatientsandtheirfamilieswhowerepartofthestudy.To theemployeesoftheOutpatientClinicofPediatricsof Hos-pitaldas ClínicasdaUNICAMPandthe NeonatalScreening ReferenceServiceof UNICAMP, especiallytobiologist Car-menSílviaGabetta,HeadoftheLaboratoryoftheNeonatal ScreeningReferenceServiceofUNICAMP.
References
1.Léger J, Olivieri A, DonaldsonM, Torresani T, Krude H, van VlietG, etal. EuropeanSocietyforPaediatricEndocrinology consensus guidelines on screening, diagnosis, and manage-mentofcongenitalhypothyroidism. JClinEndocrinol Metab. 2014;99:363---84.
2.RoseSR,BrownRS,FoleyT,KaplowitzPB,KayeCI,Sundararajan S,etal.Updateofnewbornscreeningandtherapyforcongenital hypothyroidism.Pediatrics.2006;117:2290---303.
3.MacielLM,KimuraET,NogueiraCR,MazetoGM,MagalhãesPK, NascimentoML,etal.Congenitalhypothyroidism: recommen-dationsoftheThyroidDepartmentoftheBrazilianSocietyof Endocrinologyand Metabolism. Arq BrasEndocrinol Metabol. 2013;57:184---92.
4.Corbetta C, Weber G, Cortinovis F, Calebiro D, Passoni A, Vigone MC, et al. A 7-year experience withlow blood TSH cutoff levels for neonatal screening reveals an unsuspected frequencyofcongenitalhypothyroidism(CH).ClinEndocrinol (Oxf).2009;71:739---45.
5.Grosse SD, Van Vliet G. Prevention of intellectual disability throughscreeningforcongenitalhypothyroidism:howmuchand atwhatlevel?ArchDisChild.2011;96:374---9.
6.FisherDA,DussaultJH,FoleyTP,KleinAH,LaFranchiS,Larsen PR, et al. Screening for congenital hypothyroidism: results of screening one million North American infants. J Pediatr. 1979;94:700---5.
8.DeladoëyJ,RuelJ,GiguèreY,VanVlietG.Istheincidenceof congenitalhypothyroidism reallyincreasing? A20-year retro-spectivepopulation-based studyinQuébec.JClinEndocrinol Metab.2011;96:2422---9.
9.Mitchell ML, Hsu HW, Sahai I, Group MPEW. The increased incidence of congenital hypothyroidism: fact or fancy? Clin Endocrinol(Oxf).2011;75:806---10.
10.BotlerJ,Camacho LA, CruzMM. Phenylketonuria,congenital hypothyroidismandhaemoglobinopathies:publichealthissues foraBraziliannewbornscreeningprogram.CadSaudePublica. 2012;28:1623---31.
11.MeddaE,OlivieriA,StaziMA,GrandolfoME,FazziniC,Baserga M,etal.Riskfactorsforcongenitalhypothyroidism:resultsof apopulationcase-controlstudy(1997---2003).EurJEndocrinol. 2005;153:765---73.
12.FordG,LaFranchiSH.Screeningforcongenitalhypothyroidism: aworldwideviewofstrategies.BestPractResClinEndocrinol Metab.2014;28:175---87.
13.KoradaSM,PearceM,WardPlattMP,AvisE,TurnerS,WastellH, etal.Difficultiesinselectinganappropriateneonatalthyroid stimulatinghormone(TSH)screeningthreshold.ArchDisChild. 2010;95:169---73.
14.BaroneB,LopesCL,TyszlerLS,doAmaralVB,ZarurRH,Paiva VN,etal.EvaluationofTSHcutoffvalueinblood-spotsamples inneonatalscreeningforthediagnosisofcongenital hypothy-roidismintheProgramaPrimeirosPassos---IEDE/RJ.ArqBras EndocrinolMetabol.2013;57:57---61.
15.MengreliC,Kanaka-GantenbeinC,GirginoudisP,MagiakouMA, Christakopoulou I, Giannoulia-Karantana A, et al. Screening for congenital hypothyroidism: the significance of thresh-old limit in false-negative results. J ClinEndocrinol Metab. 2010;95:4283---90.
16.Chiesa A, Prieto L, Mendez V, Papendieck P, Calcagno MEL, Gru˜neiro-Papendieck L. Prevalence and etiology of congenital hypothyroidism detected through an argentine neonatalscreeningprogram(1997---2010).HormResPaediatr. 2013;80:185---92.
17.JonesJH,SmithS,DorrianC,MasonA,ShaikhMG.Permanent congenitalhypothyroidismwithbloodspotthyroidstimulating hormone<10mU/L.ArchDisChild.2016.
18.KrudeH, BlankensteinO.Treatingpatientsnotnumbers:the benefitandburdenofloweringTSHnewbornscreeningcut-offs. ArchDisChild.2011;96:121---2.
19.RamalhoAR,RamalhoRJ,OliveiraCR,SantosEG,OliveiraMC, Aguiar-OliveiraMH.Neonatalscreeningprogramforcongenital hypothyroidisminnortheast ofBrazil:criteria,diagnosisand results.ArqBrasEndocrinolMetabol.2008;52:617---27. 20.MacielLM.Diagnóstico:novosvaloresdecorte?Avaliac¸ãocrítica
dos resultados. In: Neto-Medeiros G, editor. Hipotireoidismo congênitonoBrasilenaAméricadoSul:estadoatuale perspec-tivasfuturas.SãoPaulo:ConectfarmaPublicac¸õesCientíficas; 2012.p.67---71.
21.LoeberJG.NeonatalscreeninginEurope;thesituationin2004. JInheritMetabDis.2007;30:430---8.
22.FreireC,RamosR,AmayaE,FernándezMF,Santiago-Fernández P,Lopez-EspinosaMJ,etal.NewbornTSHconcentrationandits associationwithcognitivedevelopmentinhealthyboys.EurJ Endocrinol.2010;163:901---9.
23.LaFranchi SH. Newborn screening strategies for con-genital hypothyroidism: an update. J Inherit Metab Dis. 2010;33:S225---33.
24.LainSJ,BentleyJP,WileyV,RobertsCL,JackM,WilckenB,etal. Association between borderline neonatal thyroid-stimulating hormone concentrations and educational and developmental outcomes:apopulation-basedrecord-linkagestudy.Lancet Dia-betesEndocrinol.2016;4:756---65.
25.LaFranchi SH. Increasing incidence of congenital hypothy-roidism: some answers, more questions. J Clin Endocrinol Metab.2011;96:2395---7.
26.SackJ,FruchtH,AmadoO,BrishM,LunenfeldB.Breastmilk thyroxineandnotcow’smilkmaymitigateanddelaytheclinical pictureofneonatalhypothyroidism.ActaPaediatrScandSuppl. 1979;277:54---6.
27.BodeHH,VanjonackWJ,CrawfordJD.Mitigationofcretinism bybreast-feeding.Pediatrics.1978;62:13---6.
28.deZegherF,Vanderschueren-LodeweyckxM,HeinrichsC,Van VlietG,MalvauxP.Thyroiddyshormonogenesis:severe hypothy-roidism after normal neonatal thyroid stimulating hormone screening.ActaPaediatr.1992;81:274---6.