CROSS-CULTURAL ADAPTATI ON AND VALI DATI ON OF THE I NSTRUMENT DI ABETES – 3 9
( D-3 9 ) : BRAZI LI AN VERSI ON FOR TYPE 2 DI ABETES MELLI TUS PATI ENTS – STAGE 1
1Fláv ia Alline de Queir oz2 Ana Em ilia Pace3 Claudia Benedit a dos Sant os4
Queiroz FA, Pace AE, Sant os CB. Cross- Cult ural Adapt at ion And Validat ion Of The I nst rum ent Diabet es – 39 ( D-39) : brazilian version for t ype 2 Diabet es Mellit us Pat ient s – St age 1. Rev Lat ino- am Enferm agem 2009 set em bro-out ubr o; 17( 5) : 708- 15.
The st udy aim ed t o accom plish a cross- cult ural adapt at ion of t he “ Diabet es - 39 - D- 39” inst rum ent for Brazil, t o t est t he v alidit y of t he adapt ed v er sion in a sam ple of t y pe 2 diabet es m ellit us pat ient s and t o descr ibe t he part icipant s of t he st udy, according t o t he scores obt ained on t he Likert - t ype scale. The inst rum ent adapt at ion process followed several st eps: inst rum ent t ranslat ion; achievem ent of t he consensus in Port uguese; evaluat ion by an expert com m it t ee; back- t ranslat ion; achievem ent of t he consensus in English; com parison of t he original and consensus versions in English; sem ant ic analysis and pre- t est of t he Port uguese version. Result s showed that the instrum ent item s, in the first stage of cultural adaptation to Portuguese, presented high internal consistency levels.
DESCRI PTORS: qualit y of life; diabet es m ellit us, t y pe 2; v alidat ion st udies
ADAPTACI ÓN CULTURAL Y VALI DACI ÓN DEL I NSTRUMENTO DI ABETES – 3 9 ( D-3 9 ) :
VERSI ÓN PARA BRASI LEÑOS CON DI ABETES MELLI TUS TI PO 2 -FASE 1
Est e est udio t uvo com o obj et ivos adapt ar , cult ur alm ent e, par a el Br asil el “ Diabet es – 39 – D- 39” , com pr obar la v alidez de la v er sión adapt ada, en una m uest r a de per sonas con diabet es m ellit us t ipo 2 , y descr ibir los par t icipant es del est udio, según los punt aj es obt enidos por m edio de la aplicación de la escala t ipo Liker t . El pr oceso de adapt ación del inst r um ent o siguió las siguient es et apas: t r aducción del inst r um ent o, obt ención del con sen so en p or t u g u és, ev alu ación p or u n com it é d e j u eces, b ack - t r an slat ion , ob t en ción d el con sen so en inglés, com paración de las versiones originales y consenso en inglés, análisis sem ánt ica y prueba pilot o de las v er sion es en p or t u g u és. Los r esu lt ad os m ost r ar on q u e el in st r u m en t o, en su p r im er a f ase d e ad ap t ación cult ur al par a el por t ugués, pr esent ó índices elev ados de consist encia int er na de sus ít em s.
DESCRI PTORES: calidad de v ida; diabet es m ellit us t ipo 2; est udios de v alidación
ADAPTAÇÃO CULTURAL E VALI DAÇÃO DO I NSTRUMENTO DI ABETES – 3 9 ( D-3 9 ) :
VERSÃO PARA BRASI LEI ROS COM DI ABETES MELLI TUS TI PO 2 - FASE
Est e est u do t ev e com o obj et iv os adapt ar , cu lt u r alm en t e, par a o Br asil o “ Diabet es – 3 9 – D- 3 9 ” , t est ar a v alid ad e d a v er são ad ap t ad a, em u m a am ost r a d e p essoas com d iab et es m ellit u s t ip o 2 , e d escr ev er os part icipant es do est udo, segundo os escores obt idos por m eio da aplicação da escala t ipo Likert . O processo de adapt ação do in st r u m en t o segu iu as segu in t es et apas: t r adu ção do in st r u m en t o, obt en ção do con sen so em por t uguês, av aliação por um com it ê de j uízes, back- t r anslat ion, obt enção do consenso em inglês, com par ação d as v er sões or igin ais e con sen so em in glês, an álise sem ân t ica e p r é- t est e d as v er sões em p or t u gu ês. Os r esu lt ad os m ost r ar am q u e o in st r u m en t o, em su a p r im eir a f ase d e ad ap t ação cu lt u r al p ar a o p or t u g u ês, apr esent ou índices elev ados de consist ência int er na dos seus it ens.
DESCRI TORES: qualidade de v ida; diabet es m ellit us t ipo 2; est udos de v alidação
1Paper ext ract ed from Mast er ’s Thesis; 2RN, M.Sc. in Nursing, e- m ail: [email protected] .br; 3RN, Ph.D. in Nursing, Associat e Professor, Escola de Enferm agem de Ribeirão Pret o, Universidade de São Paulo, WHO Collaborat ing Cent re for Nursing Research Developm ent , Brazil, e- m ail: [email protected]; 4St at ist ician, Associat e Professor, Escola de Enferm agem de Ribeirão Pret o, Universidade de São Paulo, WHO Collaborat ing Cent re for Nursing Research Developm ent , Brazil, e- m ail: cbsant [email protected].
I NTRODUCTI ON
D
iabet es m ellit u s ( DM) is a h et er ogen eou s gr oup of m et abolic disor der s w it h hy per gly cem ia ast h e co m m o n ch ar act er i st i c, r esu l t i n g f r o m i n su l i n
a c t i o n a n d / o r s e c r e t i o n d e f e c t s . Th e c u r r e n t
classificat ion is et iology- based. I n t he pr esent st udy,
t ype 2 DM is highlight ed, which is present in 90- 95%
of cases and is charact erized by defect s in t he act ion
and/ or secr et ion of insulin. I t s im por t ance for public
healt h is j ust ified by t he increasing prevalence rat es,
t he im pact of m ort alit y and t he healt h problem s t hat
affect t he qualit y of life ( QoL) of pat ient s and t heir
r elat iv es( 1 ).
Resear ch o n t h e r el at i o n b et w een al t er ed
g l u co se m e t a b o l i sm a n d q u a l i t y o f l i f e sh o w e d a
g r a d u a l d e cr e a se i n Qo L t h r o u g h t h e ca t e g o r i e s
g l u c o s e t o l e r a n c e , r e c e n t l y d i a g n o s e d D M a n d
pr eviously know n DM. The aut hor s show ed t hat poor
QoL can increase t he probabilit y of developing t ype 2
DM, an d can also b e associat ed w it h less h ealt h y
lifest yle opt ions( 2). On t he ot her hand, DM can cause p o o r Qo L d u e t o t h e i n c r e a s e d s y m p t o m s o f
hy per gly cem ia and ot her diseases r elat ed t o DM and
obesit y( 3 ).
Th e i m p o r t a n ce o f sp e ci f i c i n st r u m e n t t o
assess DM pat ient s’ QoL is due t o t he fact t hat t his
t y pe of in st r u m en t is dir ect ed at t h e m ost r elev an t
charact erist ics of t he disease or condit ion t hat is being
st u d ied , an d of t h e p at ien t s, con sid er in g t h at QoL
m e a su r e s su p p o r t i n t e r v e n t i o n st r a t e g i e s i n t h e
at t em pt t o m inim ize t he im pact of t ype 2 DM( 4). H e a l t h - r e l a t e d q u a l i t y o f l i f e ( H RQo L)
represent s t he int ent t o quant ify t he consequences of
a disease and it s t reat m ent s, according t o how people
perceive t heir capacit y t o have a useful life and develop
t heir skills. Hence, it s m easur em ent is subj ect ive, as
m an y o f i t s d i m en si o n s can n o t b e m easu r ed i n a
phy sically dir ect w ay and, also, because it is r elat ed
t o how people see t he im pact not of t heir dysfunct ion,
but of it s exist ence( 5).
No w a d a y s, m a n y i n st r u m e n t s h a v e b e e n
d e v e l o p e d t o a sse ss H RQo L, b a se d o n d i f f e r e n t
d e f i n i t i o n s o f t h e c o n c e p t . I n t h i s r e s p e c t , t h e
p r olif er at ion of m easu r em en t in st r u m en t s p ar t ially
affect s t he grow ing need t o dem onst rat e t he efficacy
of a g iv en car e or t r eat m en t , t h u s ex p an d in g t h e
consensus about t he need t o st abilize t he effect s of a
g iv en d isease or t r eat m en t in t h e p at ien t ’s lif e, or
even t o look beyond t he disease, in order t o guarant ee
a m or e holist ic v iew on t he pat ient and incor por at e
t h e p a t i e n t ’ s p e r s p e c t i v e i n t o t h e a s s e s s e d
in t er v en t ion s( 6 ).
Alt hough a r ange of inst r um ent s is av ailable
t o assess t he HRQoL of DM pat ient s, t he researchers
did not ident ify any research in lit erat ure t hat described
t he use of Port uguese- language inst rum ent s t o assess
HRQoL and which are specific for Brazilian DM pat ient s,
independent ly of t he t y pe.
D i a b et es- 3 9 ( D - 3 9 ) i s a m u l t i d i m en si o n a l
scale elabor at ed in t he USA. I t consist s of 39 it em s
t hat assess HRQoL wit h respect t o five dom ains in t he
pat ient ’s life: energy and m obilit y ( 15 it em s) , diabet es
cont rol ( 12 it em s) , anxiet y and w orry ( 4 it em s) , social
bu r den ( 5 it em s) an d sex u al f u n ct ion in g ( 3 it em s) .
Each it em is calculat ed based on t he DM pat ient s’
self-assessm ent of t heir qualit y of life, t he ext ent t o which
it was affect ed during t he previous m ont h by t he act ion
or act ivit y expressed in each it em , placing an “ X” on
a scale in t he form of a st raight line, divided by vert ical
m arks int o spaces num bered from 1 t o 7, in which 1
r epr esen t s qu alit y of lif e n ot af f ect ed at all, an d 7
ex t r em ely affect ed. For r eliabilit y analy sis, t he scale
a u t h o r s( 6 ) u se d Cr o n b a ch ’ s a l p h a co e f f i ci e n t ( á ) , r an g in g f r om 0 . 8 1 t o 0 . 9 3 in t h e f iv e d im en sion s,
consider ing lev els of 0.70 or m or e as accept able.
I n 2006, t he D- 39 was adapt ed and validat ed
for t he Mexican cult ure in a sam ple of 249 pat ient s. I t
r ev eal ed t o b e a r el i ab l e an d v al i d i n st r u m en t t o
m easu r e t h e q u alit y of lif e of Mex ican t y p e 2 DM
p a t i e n t s ( Cr o n b a ch ’ s a l p h a = 0 . 9 5 f o r t h e t o t a l
scor e)( 7 ).
Co n si d e r i n g t h a t t y p e 2 D M i s t h e m o st
p r e v a l e n t t y p e o f d i a b e t e s w i t h d i f f e r e n t cl i n i ca l
char act er ist ics t han t y pe 1, t hus gener at ing differ ent
care needs, t his st udy focused on t ype 2 DM pat ient s.
Th e s t u d y a i m e d t o p e r f o r m t h e c r o s s - c u l t u r a l
a d a p t a t i o n o f t h e “ D i a b et es – 3 9 – D - 3 9 ” t o t h e
Brazilian cult ure, t o t est t he reliabilit y and validit y of
t he adapt ed version in a sam ple of t ype 2 DM, and t o
describe t he st udy part icipant s according t o t he scores
obt ained by apply ing t he Lik er t - t y pe scale.
METHOD
Th e st u dy w as dev eloped aft er appr ov al by
t he Et hics and Resear ch Com m it t ee at Faculdade de
Medicina de Rio Pret o - FAMERP, São José do Rio Pret o,
Th e in st r u m en t u sed w as t h e Diab et es- 3 9
which, in t his st udy, t ook t he form of a horizont al bar
divided in boxes t hat were num bered from 1 t o 7, t o
replace t he st raight line used in t he original inst rum ent .
Th i s c h a n g e w a s s u g g e s t e d b y t h e r e s e a r c h
part icipant s and previously aut horized by t he original
aut hor( 6). To analyze t he answers, t he num ber m arked w it h an “ X” w as con sid er ed , w it h ou t an y 0 . 5 - p oin t
appr ox im at ion s ( u pw ar ds or dow n w ar ds, f r om 1 t o
7) in case t he part icipant m arked one of t he borders
of t he box, so as t o sim plify t he classificat ion( 6). The sum of scor es for each sect ion, t he t ot al scor e and
classif icat ion s of self - p er ceiv ed q u alit y of lif e an d
diabet es sever it y w er e t r anspor t ed t o a scale fr om 0
t o 100 by applying t he form ula below, wit h a view t o
t heir linear t ransform at ion in t he respect ive dom ains:
( g r oss classif icat ion – m in im u m v alu e) / ( m ax im u m
v al u e – m i n i m u m v al u e) X 1 0 0 . Th is is a g en er ic
form ula t o t ransform any values ranging bet ween t wo
– upper and lower - lim it s, on a scale wit h 0% as t he
m inim um and 100% as t he m ax im um , and does not
depend on any specific inst r um ent . This dev ice w as
only used t o facilit at e com parisons bet ween t he scores
of t h is an d an y ot h er scale, pr ov ided t h at bot h ar e
ex pr essed bet w een 0 and 100% .
CROSS- CULTURAL AD APTATI ON
PROCED URES
I nit ially, t he r esear cher s obt ained per m ission
t o use t he D- 39. Nex t , t he cr oss- cult ur al adapt at ion
process used in t his st udy is described, which follows
t he pr oposal pr esent ed in lit er at ur e( 8), t oget her w it h t he change in t he order of t he st eps proposed for t his
adapt at ion pr ocess( 9- 10).
The expert com m it t ee assessm ent before t he
b ack- t r an sl at i o n p er m i t s t h e d et ect i o n o f p o ssi b l e
e r r o r s o r c o m p r e h e n s i o n p r o b l e m s t h a t c a n b e
m odif ied in t h e t r an slat ed v er sion( 9 - 1 0 ). Each of t h e in st r u m en t it em s w as su b j ect t o sem an t ic an aly sis
before perform ing t he pre- t est , wit h a view t o having
a group of represent at ives from t he t arget populat ion
check t he underst andabilit y of all inst rum ent it em s( 9).
Translat ion of D- 39 t o Por t uguese
Th e t r a n s l a t i o n w a s c a r r i e d o u t b y t w o
Br azilians, one of w hom had m or e t han 20 y ear s of
experience as an English t eacher, while t he ot her was
an ex p er ien ced n u r se an d h ad t au g h t En g lish at a
language school for m or e t han fiv e y ear s. This st ep
r esu lt ed in t w o Por t u gu ese v er sion s, called v er sion
t ranslat ed t o Port uguese ( VTP) , VTP - 1 and VTP – 2,
r esp ect iv ely.
Achievem ent of first consensus version in Port uguese
Th e r e s e a r c h e r s i n v o l v e d i n t h e p r o j e c t
( st udent and advisor) com pared t he version t ranslat ed
t o Por t uguese and elabor at ed a consensus ver sion in
Port uguese, called consensus of versions in Port uguese
– 1 ( CVP – 1) .
Assessm en t by ex per t com m it t ee
An ex p er t com m it t ee w it h sev en m em b er s
w as set up, com pr ising: one exper t on qualit y of life
and m easur em ent inst r um ent s ( nur se, Ph. D., facult y
m em ber) , one endocrinologist , one bilingual t ranslat or,
on e n u r se ex per ien ced in diabet es, on e DM pat ien t
( l a b o r a t o r y t ech n i ci a n a t Ho sp i t a l d a s Cl ín i ca s o f
Ribeirão Pret o Medical School - HCFMRP) and t he t wo
researchers responsible for t he proj ect . All com m it t ee
m em bers were fluent in English. During t his m eet ing,
c o o r d i n a t e d b y t h e p r o j e c t r e s e a r c h e r s , t h e
p a r t i ci p a n t s w er e i n f o r m ed t h a t t h e g o a l o f t h ei r
p ar t i ci p at i o n i n t h i s com m i t t ee w as t o assess t h e
s e m a n t i c , i d i o m a t i c , c u l t u r a l a n d c o n c e p t u a l
equ iv alen ce of t h e t r an slat ed v er sion it em s ( CVP –
1) . I n t his st ep, each Com m it t ee m em ber received a
copy of t h e or igin al v er sion of D- 3 9 ( VO) , t oget h er
w it h it s r espect iv e Por t uguese t r anslat ion ( CVP – 1) .
Next , one of t he researchers read t he t ranslat ion and
t h e p a r t i ci p a n t s d i scu sse d e q u i v a l e n ce s b e t w e e n
t h e En g lish an d t h e t r an slat ed v er sion f or each of
t h e 3 9 i n s t r u m e n t i t e m s . W h e n a n y o f t h e
p a r t i ci p a n t s d i d n o t a g r e e w i t h t h e t r a n sl a t i o n ,
su ggest ion s w er e m ade t o ch an ge t h e w r it in g, an d
c h a n g e s w e r e a p p r o v e d w h e n a t l e a s t s i x
p ar t icip an t s ( m or e t h an 8 0 % ) ag r eed w it h t h e n ew
pr oposal. At t h e en d of t h is st ep, con sen su s v er sion
2 in Por t u g u ese w as ob t ain ed ( CVP – 2 ) .
Back t r anslat ion and consensus v er sion in English
Tw o independent t ranslat ors w ho w ere fluent
in English and lived in Brazil and had lived in t he USA
f o r s e v e r a l y e a r s c a r r i e d o u t t h i s s t e p . Th e s e
did not k now t he or iginal v er sion of t he inst r um ent .
Each of t h em elabor at ed an En glish v er sion , called
English v er sion t r anslat or 1 and t r anslat or 2 , called
VI - 1 and VI - 2. A m eet ing was held bet ween t he st udent
and t he t r anslat or s, w ho did not k now each ot her ’s
v er sion . Th en , t h e r esear ch er p r esen t ed t h e st u d y
goals, t he purpose of D- 39( 6) and it s applicabilit y. Next , bot h v er sion s w er e assessed an d a f in al v er sion in
English ( VI F) w as defined.
Com par ison bet w een or iginal and consensus v er sions
in English
Aft er defining t he VI F, each t ranslat or received
a copy of t he original inst rum ent ( VO) for com parison
w i t h t h e VI F. At t h a t m o m e n t , e a ch p a r t o f t h e
inst rum ent ( inst ruct ions, it em s and answer scale) was
r ead and t he t r anslat ions w er e assessed w it h a v iew
t o f i n d i n g t h e m o st ad eq u at e v er si o n i n t er m s o f
c o n c e p t u a l a n d c u l t u r a l e q u i v a l e n c e . W r i t i n g
adj ust m ent s were m ade in t he English version of som e
i t e m s, w h i ch t h e n n e e d e d r e f o r m u l a t i o n s i n t h e
Port uguese version CVP- 2. This result ed in consensus
v er sion 3 in Por t uguese.
The final version in English ( VI F) of D- 39 was
com par ed w it h t he or iginal ver sion of t he inst r um ent
( in English) , w it h a v iew t o check ing t he r eplicabilit y
of t he scale t hat w as being subj ect t o cr oss- cult ur al
adapt at ion. Aft er com plet ing t hese st eps, t he VI F was
sen t t o t h e au t h or of t h e or ig in al in st r u m en t( 6 ) f or su ggest ion s. Th r ee day s lat er, t h e au t h or an sw er ed
t h at h e h ad car efu lly r ev iew ed t h e back t r an slat ion
and t hat each quest ion seem ed t o r eflect t he act ual
m e a n i n g o f t h e o r i g i n a l v e r s i o n , a n d g a v e h i s
per m ission t o cont inue t he r esear ch.
Sem ant ic analy sis of it em s
Sem ant ic analysis aim s t o verify whet her t he
t arget populat ion of an inst rum ent can underst and all
of it s it em s. Ther efor e, it is r ecom m ended t hat t his
pr ocedur e be per for m ed w it h sm all gr oups ( t hr ee t o
four )( 9). I n t his r esear ch, four pat ient s w er e involved w ho w er e under follow - up at a basic healt h ser v ice,
aim ing t o analyze t heir underst anding of t he 39 it em s’
w r i t i n g a n d t h e i r a n s w e r s . Th e p a t i e n t s g a v e
suggest ions in t erm s of changing words t hat were lit t le
used in t heir daily life by ot her m ore colloquial t erm s,
h o w e v e r, w i t h o u t a n y ch a n g e i n m e a n i n g . Th u s,
co n sen su s v er si o n 4 i n Po r t u g u ese ( CVP- 4 ) w a s
obt ained. The pat ient s r epor t ed t hat quest ions w er e
easy t o u n der st an d. As f or t h e an sw er scale, all of
t h em af f ir m ed t h at t h ey cou ld g iv e an sw er s m or e
easily when t hese were direct ly relat ed t o t he num ber
shown on t he scale, as shown by opt ions 1 t o 7. Thus,
t h e r e s e a r c h e r s d e c i d e d t o f o l l o w t h e p a t i e n t s ’
suggest ions, t hat is, t he answer opt ions were as shown
by t he num bers, wit hout any 0.5 approxim at ions. This
d i f f e r e d f r o m t h e o r i g i n a l sca l e , w h e r e 0 . 5 w a s
subt ract ed from or added t o t he score in case t he “ X”
m ar k ed appr oach ed t h e lef t or r igh t m ar gin of t h e
answer box, respect ively. Ot her aut hors( 7) also adopt ed t h i s f o r m o f a n a l y zi n g a n sw er s i n t h e st u d y t h a t
perform ed t he cross- cult ural adapt at ion and validat ion
of D- 39 for Mexican t ype 2 DM pat ient s.
Psy ch om et r ic pr oper t y an aly sis
Re l i a b i l i t y a n a l y si s: w a s a n a l y ze d b y t h e
int ernal consist ency of it em s in each dom ain of D- 39,
applying Cronbach’s alpha – levels of 0.70 or higher(
11-1 2 )
. Pear son ’s p r od u ct - m om en t cor r elat ion t est w as
u sed t o access in t er cor r elat ion s bet w een each it em
of D- 39 and t he t ot al scale score.
V a l i d i t y a n a l y s i s : c o n s t r u c t v a l i d i t y
( con v er gen t an d discr im in an t v alidit y ) of D- 3 9 w as
st u died t h r ou gh t h e cor r elat ion bet w een it em s an d
d o m a i n s, u si n g m u l t i t r a i t - m u l t i m e t h o d a n a l y si s.
Mult it r ait Analy sis Pr ogr am ( MAP) soft w ar e w as used
f or t h is p u r p ose( 1 3 ). Discr im in an t v alid it y w as also assessed d escr ip t iv ely b y com p ar in g t h e scor es of
pat ient s using insulin or not .
Dat a collect ion: dat a were collect ed according
t o t he ser v ice r out ine, at a t im e befor e t he nur sing
a n d / o r m e d i ca l co n su l t a t i o n s, i n a p r i v a t e r o o m .
Pa r t i c i p a n t s p r e v i o u s l y r e c e i v e d t h e n e c e s s a r y
in f or m at ion an d a f r ee an d in f or m ed con sen t t er m
( FI CT) , signed by t he part icipant and t he researcher if
t he form er agreed. Next , t he adapt ed D- 39 was applied.
Th e st u d y p o p u l a t i o n co n si st ed o f t y p e 2
diabet es m ellit us ( DM- 2) pat ient s follow ed at a basic
h ealt h ser v ice in São José do Rio Pr et o, SP, Br azil.
I nclusion cr it er ia w er e: older t han 3 0 y ear s of age,
in d ep en d en t ly of g en d er an d t r eat m en t , p r eser v ed
r easoning sk ills and w it hout lim it at ions or disabilit ies
t o fill out t he inst r um ent and agr ee t o par t icipat e in
t he st udy at t he t im es before t he m edical or nursing
consult at ions. The sam ple com prised 52 pat ient s who
at t ended a consult at ion at t he healt h service bet ween
sociodem ographic and clinical dat a were obt ained from
t he r ecor ds cont ained in t he ( adapt ed) HI PERDI A file
of t he service and from t he m edical records, using a
specific inst r um ent elaborat ed by t he r esear cher.
RESULTS
Upon t he pat ient s’ suggest ions, t hr ee it em s
were m odified, as all pat ient s m ent ioned t hat glucose
and sugar ar e under st ood in t he sam e w ay, so t hat
g l u c o s e w a s m a i n t a i n e d ; t h e w o r d p r o v e n i e n t e
( co m i n g f r o m ) w a s n o t w e l l a cce p t e d e i t h e r a n d
replaced by due t o diabet es; t he sam e happened wit h
t he word frequency, replaced by... relax several t im es
per day.
Pr e- t est o f t h e ad ap t ed v er si o n : t h e f i n al
v er sion in Por t u gu ese ( VFP) of D- 3 9 w as su bm it t ed
t o a pr et est , inv olv ing four pat ient s fr om t he t ar get
p op u lat ion . Af t er com p let in g t h e in st r u m en t , each
p at ien t w as ask ed ab ou t t h e u n d er st an d ab ilit y an d
relevance of t he D- 39. I n t his st ep, no problem s were
m et , n eit h er f or u n d er st an d in g n or com p let in g t h e
inst r um ent . Thus, it w as consider ed t er m inat ed and
t he researchers decided t o m ove on t o t he prelim inary
v alidat ion of t h e in st r u m en t . Af t er t h e pr et est , t h e
version of D- 39 was called final version in Port uguese
( VFP) .
Th e Por t u gu ese v er sion of t h e Diabet es- 3 9
( D- 39 VFP) w as applied t o a gr oup of DM- 2 pat ient s
bet w een Oct ober 2 0 0 7 an d Jan u ar y 2 0 0 8 . Fift y - t w o
p ar t icip an t s com plied w it h t h e in clu sion cr it er ia, of
w hom 18 ( 34. 6% ) w er e m en. Ages r anged fr om 45
t o 84 years, wit h 62.8 ( SD= 8.6) as t he m ean and 63
y ear s as t he m edian age. Low educat ion lev els w er e
f ou n d ( 3 1 / 5 2 ; 5 9 . 6 % ) , w it h eit h er u n f in ish ed basic
ed u cat ion , n ot k n ow in g h ow t o r ead an d w r it e or
alphabet ized. The m ean durat ion of t he disease am ong
t h e p ar t icip an t s w as 9 . 1 5 ( SD= 4 . 2 ) y ear s an d t h e
m ed ian 9 y ear s, w it h a m in im u m of 1 y ear an d a
m ax im um of 20 y ear s. Wom en pr edom inat ed am ong
insulin users, wit h 20 ( 68.9% ) out of 29 users. As t o
t he body m ass index ( BMI ) in t he st udy sam ple, eight
pat ien t s ( 1 5 . 3 8 % ) fell w it h in t h e n or m al r an ge an d
4 4 ( 8 4 . 6 % ) w e r e c l a s s i f i e d a s o v e r w e i g h t a n d
o b e s e( 1 4 ). M e a n d i s e a s e ( D M - 2 ) t i m e o f s t u d y p a r t i ci p a n t s w a s 9 . 2 ( SD : 4 . 2 ) y ea r s a n d g l u co se
cont r ol lev els w er e inadequat e, w it h a m ean lev el of
175.37 ( 35; 67.3% ) ; overweight and obesit y in a large
par t of t he sam ple ( 44; 84.6% ) ; insulin user s t ot aled
2 9 p ar t i ci p an t s, 2 0 of w h om w er e w om en . As f or
com orbidit ies, a large num ber of hypert ensive wom en
was founds ( 28; 82.3% ) . This clinical profile is sim ilar
t o w h at w as fou n d in t h e st u dy t h at dev eloped t h e
or iginal ver sion of t he D- 39( 6).
Pe a r s o n ’ s c o r r e l a t i o n c o e f f i c i e n t s v a r i e d
b e t w e e n e a ch i t e m o f D - 3 9 a n d t h e t o t a l sca l e
c o e f f i c i e n t ( f r o m 0 . 2 4 t o 0 . 7 0 ) , w h i c h d i d n o t
consider able int er fer e in t he Cr onbach’s alpha lev els,
w hich varied from 0.913 t o 0.918.
Result s for t he dom ains of t he D- 39 are shown
in Table 1.
s n i a m o D 9 3
-D Noofitems Cronbach's
a h p l A e l b i s s o P l a v r e t n i d e n i a t b O l a v r e t n
i Median Mean (SD)
l o r t n o c s e t e b a i
D 12 0.85 12-84 14-77 51.5 48.8 (14.5) y r r o w d n a y t e i x n
A 4 0.58 4-28 6-27 18 17.8 (5.2) n e d r u b l a i c o
S 5 0.62 5-35 5-30 18.5 17.2 (6.5) g n i n o i t c n u f l a u x e
S 3 0.83 3-21 3-21 13 12 (5.5) y t il i b o m d n a y g r e n
E 15 0.79 15-105 20-83 60 56.5 (15.3) e r o c s l a t o
T 39 0.92 39-273 49-217 163 152.5 (38.6)
Table 1 – Descr ipt iv e st at ist ics and r eliabilit y of D- 39 dom ains and t ot al scor e for st udy sam ple ( n= 52) . São
José do Rio Pret o, SP, 2008
Cr on b ach ’s alp h a coef f icien t s r an g ed f r om
0.58 (anx iet y and w or r y) t o 0.85 (diabet es cont r ol) ,
w h i ch a r e co n si d e r e d a d e q u a t e( 1 1 ) t o a sse ss t h e int ernal consist ency of it em s in t he different dom ains.
The t ot al scor e, w it h a coefficient of 0. 917, show ed
good int er nal consist ency.
Th e par t icipan t s’ dist r ibu t ion w as descr ibed
accor ding t o t heir answ er s t o t he inst r um ent , w it h a
view t o checking for t he exist ence of floor and ceiling
effect s. These effect s w er e not found in t he dom ains
of t he D- 39, as each dom ain concent r at ed less t han
w i t h t h e f o l l o w i n g co n cen t r at i o n o f m i n i m u m an d
m axim um scores, respect ively: diabet es cont rol: 2.78
equal t o 1 ( 1.9% ) and 90.28 equal t o 1 ( 1.9% ) ; anxiet y
and worry: 8.33 equal t o 1 ( 1.9% ) and 95.83 equal t o
2 ( 3 . 8 % ) ; social bu r den: 0 equ al t o 3 ( 5 . 8 % ) an d
83.33 equal t o 1 ( 1.9% ) ; sexual funct ioning: 0 equal
t o 7 ( 13.5% ) and 100, equal t o 3 ( 5.8% ) ; energy and
m obilit y: 56 equal t o 1 ( 1.9% ) and 75.56 equal t o 1
( 1.9% ) . The inst rum ent ’s convergent and discrim inant
v alidit y w as assessed t hr ough m ult it r ait - m ult im et hod
an aly sis ( MTMM) , w h ich ex am in es t h e cor r elat ion s
bet ween it em s and dom ains. MTMM analysis explores
t h e r el at i o n s b et w een t h e i n st r u m en t ’s i t em s an d
dim en sion s, t h r ou gh w h ich it ev iden ces con v er gen t
and discr im inant validit y. The m et hod is quit e useful
when t he inst rum ent cont ains a large num ber of it em s,
w hich im plies a consider able quant it y of cor r elat ions.
I n in it ial v alid at ion st u d ies, con v er g en t v alid it y is
sat isfied if t he cor r elat ion bet w een an it em and t he
dom ain it belongs t o exceeds 0.30 and, in final st udies,
if it ex ceeds 0 . 4 0 . Discr im in an t v alidit y is sat isf ied
w h en ev er t h e cor r elat ion bet w een an it em an d t h e
dim ension it hy pot het ically belongs t o is higher t han
it s cor r elat ion w it h t he ot her dim ensions( 15).
To t est for const ruct validit y, conv ergent and
discrim inant validit y were observed according t o MTMM
analysis, assessing t he correlat ions bet w een t he it em
and t he dim ension it belongs t o and bet ween t he it em
and t he dim ension it does not belong t o. I n case t he
co r r e l a t i o n co e f f i ci e n t b e t w e e n t h e i t e m a n d t h e
d im en sion it b elon g s t o is h ig h er t h an t h at w it h a
dim ension it does not belong t o, conv er gent v alidit y
e x i st s. I n ca se a n i t e m i s m o d e r a t e l y co r r e l a t e d
( re” 0.3) wit h t he dim ension it belongs t o, convergent
validit y also exist s ( 15).
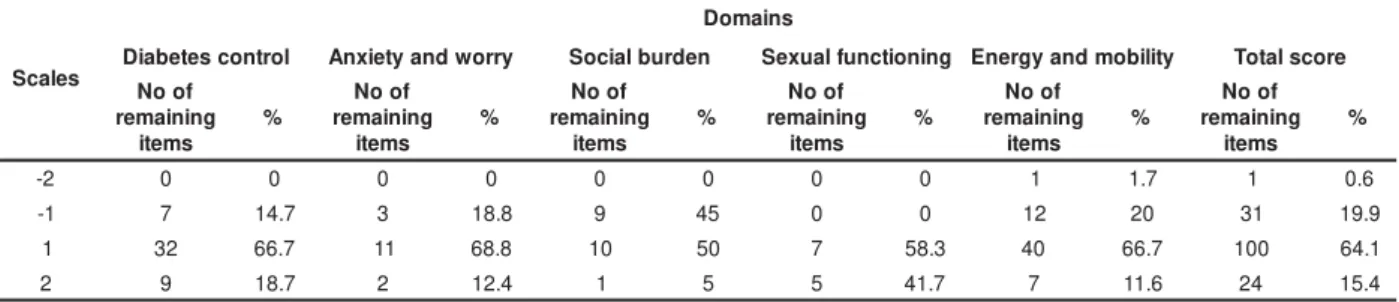
A c c o r d i n g t o t h e M A P p r o g r a m( 1 5 ), t h e p e r ce n t a g e s o f i t e m s i n a g i v e n d i m e n si o n , w i t h
cor r elat ion s t h at ar e sign if ican t ly h igh er, or m er ely
h igh er t h an t h eir cor r elat ion s w it h t h e dim en sion s,
ar e show n in Table 2. Values fr om - 2 t o 2 show n in
Ta b l e 2 m ea n t h e f o l l o w i n g : 2 i n d i ca t es t h a t t h e
correlat ion bet ween t he it em and t he scale it belongs
t o is significant ly higher t han it s cor r elat ion w it h t he
sca l e i t d o es n o t b el o n g t o , 1 i n d i ca t es t h a t t h e
correlat ion bet ween t he it em and t he scale it belongs
t o is higher t han it s correlat ion wit h t he scale it does
not belong t o, - 1 indicat es t hat t he correlat ion bet ween
t he it em and t he scale it belongs t o is lower t han it s
correlat ion wit h t he scale it does not belong t o and - 2
indicat es t hat t he cor r elat ion bet w een t he it em and
t he scale it belongs t o is significant ly low er t han it s
correlat ion wit h t he scale it does not belong t o.
Table 2 – MAP analysis r esult s for D- 39 scor es, Br azilian ver sion. São José do Rio Pr et o, SP, 2008
s e l a c S s n i a m o D l o r t n o c s e t e b a i
D Anxietyandworry Socialburden Sexualfunctioning Energyandmobility Totalscore
f o o N g n i n i a m e r s m e t i % f o o N g n i n i a m e r s m e t i % f o o N g n i n i a m e r s m e t i % f o o N g n i n i a m e r s m e t i % f o o N g n i n i a m e r s m e t i % f o o N g n i n i a m e r s m e t i % 2
- 0 0 0 0 0 0 0 0 1 1.7 1 0.6
1
- 7 14.7 3 18.8 9 45 0 0 12 20 31 19.9 1 32 66.7 11 68.8 10 50 7 58.3 40 66.7 100 64.1 2 9 18.7 2 12.4 1 5 5 41.7 7 11.6 24 15.4
Con sid er in g t h at , f or d iscr im in an t v alid it y,
an sw er p er cen t ag es sh ou ld b e con cen t r at ed in t h e
sum of scales 1 and 2, it is given t hat : diabet es cont rol
( 8 5 . 4 % ) , anx iet y and w or r y ( 8 1 . 2 % ) , social bur den
( 55% ) , sexual funct ioning ( 100% ) , energy and m obilit y
( 78.3% ) and t ot al score ( 79.5% ) . Hence, discrim inant
validit y in t he social burden dom ain is low .
I n a d d i t i o n , Ma n n - W h i t n e y ’ s U- t e s t w a s
applied for discr im inant v alidit y bet w een t he gr oups
t hat used insulin or not for m et abolic cont rol of DM –
2. And it was observed t hat pat ient s who used insulin
obt ained st at ist ically significant p values ( p< 0.05) for
diabet es con t r ol an d social bu r den. The com par ison
of m edians in each dom ain, consider ing par t icipant s
who used insulin or not , shows discrim inat ion bet ween
t he groups wit h respect t o diabet es cont rol and social
burden, w it h t he follow ing scor es 56/ 47; 20/ 16.
DI SCUSSI ON
Th is st u d y aim ed t o accom p lish t h e cr
oss-cult ur al adapt at ion of a healt h- r elat ed qualit y of life
diabet es m ellit us, considering t hat no inst rum ent s for
t h is t ar get popu lat ion ex ist in t h e Br azilian cu lt u r al
con t ex t .
The sam ple consist ed of 52 people wit h a m ean
age of 62.8 y ear s, pr edom inant ly fem ale, m ar r ied or
living wit h t heir children and wit h low educat ion level.
A n e x p e r t c o m m i t t e e a s s e s s e d t h e
i n st r u m en t ’ s sem a n t i c, i d i o m a t i c, co n cep t u a l a n d
cult ural equivalences aft er t he first t ranslat ed version
( CVP – 1) . This com m it t ee involved professionals from
d if f er en t h ealt h ar eas w it h p ar t icu lar k n ow led g e in
t he fields of diabet es, qualit y of life and adapt at ion of
assessm ent inst r um ent s, as w ell as a DM- 2 pat ient .
These m em ber s cont r ibut ed t o t he assessm ent of
D-39 it em s in t er m s of per t inence and under st andable
w r i t i n g . A f t e r t h i s a s s e s s m e n t o f t h e r e v i s e d
v e r si o n , t h e i n st r u ct i o n s o f t h e i n st r u m e n t w e r e
r ew r it t en , m ain ly t h e p ar t r ef er r in g t o t h e op t ion s
t h at af f ect p eop l e’s q u al i t y of l i f e, as w el l as t h e
e x a m p l e i t r e f e r r e d t o – d u r i n g t h e p a st m o n t h ,
h ow m u ch w as t h e q u alit y of y ou r lif e af f ect ed b y :
h a v i n g a n a u t o m o b i l e, w h i ch w a s ch a n g e d t o –
d u r in g t h e p ast m on t h , h ow m u ch w as t h e q u alit y
of y ou r lif e af f ect ed b y : h av in g a h ealt h p r ob lem .
Ot h er m od if icat ion s w er e m in im al an d ar e r elat ed
t o t h e i n s e r t i o n o f p r e p o s i t i o n s b e f o r e e a c h
in st r u m en t it em (p or , p elo[ a]) .
I n t his m et hodological pr ocess, t he or der in
w h i c h t h e b a c k - t r a n s l a t i o n w a s p e r f o r m e d w a s
m odified, as it occur r ed aft er t he exper t com m it t ee’s
assessm en t o f t h e i n st r u m en t . Th e t r an sl at i o n o f
consensus version 2 in Port uguese ( CVP - 2) t o English
and it s com parison w it h t he original version of D- 39,
in English, guarant eed t hat no alt erat ions were m ade
in t he it em s’ m eaning, as confirm ed by t he aut hor of
t he or iginal inst r um ent .
Co n st r u ct v a l i d i t y w a s a sse sse d t h r o u g h
convergent validit y, which was described by com paring
t he scor es obt ained bet w een each it em of D- 39 and
t he respect ive dom ain scores, so as t o assess, in t his
i n i t i al st u d y, i f t h e i t em i s m o d er at el y co r r el at ed
( r e” 0. 3) w it h t he dom ain it belongs t o. Discr im inant
validit y was assessed t hrough t he correlat ion bet ween
an it em and t he dim ension it belongs t o, in or der t o
ch eck if it s cor r elat ion w it h t h e ot h er dom ain s w as
h igh er.
To an aly ze t h e in t er n al con sist en cy of t h e
it em s in t he adapt ed v er sion w it h t he t ot al and t he
r esp ect i v e d o m ai n s, Cr o n b ach ’s al p h a co ef f i ci en t s
w er e calculat ed, gener ally obt aining lev els t hat w er e
considered adequat e: alpha equal t o 0.91 for t he t ot al
scor e, and v ar iat ion bet w een 0 . 5 8 and 0 . 8 5 for t he
dom ains. The dom ain w it h t he low est coefficient w as
a n x i et y a n d w o r r y ( 0 . 5 8 ) , w h i l e d i a b et es co n t r o l
obt ained t he highest coefficient ( 0.85) . Know ing t hat
Cr onbach’s alpha coefficient s below 0 . 7 0 can im pair
t he inst rum ent ’s int ernal consist ency( 11- 12), t he aut hors clarify t hat , in t his init ial phase of t he adapt at ion and
v alidat ion of D- 39, t he sam ple r ev ealed t o be sm all
f or t h e n u m ber of it em s. Hen ce, m or e r espon den t s
w ould be needed.
I n m o s t c a s e s , t h e a n a l y s i s o f t h e
int er cor r elat ion bet w een t he inst r um ent ’s it em s and
dom ains show ed significant and posit iv e cor r elat ions,
w it h st r on g an d v er y st r on g cor r elat ion coef f icien t s
for t he t ot al inst r um ent scor e and m edian t o st r ong
coef f icien t s f or t h e r esp ect iv e d om ain s. Ex cep t ion s
refer t o t he correlat ion bet ween t he sexual funct ioning
and anxiet y and worry dom ains, wit h lower correlat ion
coefficien t s, r an gin g fr om 0 . 2 1 (an x iet y an d w or r y )
t o 0.34 (social bur den) .
CONCLUSI ON
The D- 39, originally in English, was t ranslat ed
t o Por t u g u ese, f ollow in g all st ep s in d icat ed in t h e
m e t h o d s s e c t i o n . A c c o r d i n g t o t h e r e s u l t s , t h e
i d i o m a t i c , s e m a n t i c , c u l t u r a l a n d c o n c e p t u a l
e q u i v a l e n c e s o f t h e o r i g i n a l i n s t r u m e n t w e r e
m a i n t a i n e d , a s w e l l a s i t s v a l i d i t y a n d r e l i a b i l i t y
( i n t er n a l co n si st en cy ) ch a r a ct er i st i cs. Hen ce, t h e
result s show t hat t he version of D- 39 adapt ed t o t he
Brazilian cult ure can be a valid and reliable inst rum ent
t o m easur e t he HRQoL of DM- 2 pat ient s.
This kind of research is im port ant because it
co n t r i b u t es t o u n d er st an d t h e f act o r s i n v o l v ed i n
qu alit y of life in t h e con t ex t of people’s v alu es an d
cu l t u r e an d i n t h e assessm en t o f a g i v en h eal t h
-d i sease si t u at i o n , acco r -d i n g t o -d i f f er en t p h y si cal ,
psychological, cult ural and social com ponent s( 16), t hus cont r ibut ing t o clinical nur sing pr act ice.
REFERENCES
1 . S o c i e d a d e B r a s i l e i r a d e D i a b e t e s . Tr a t a m e n t o e
a c o m p a n h a m e n t o d o d i a b e t e s m e l l i t u s : d i r e t r i z e s d a
Sociedade Br asileir a de Diabet es. Rio de Janeir o: Diagr aphic
2 . Tap p RJ, Du n st an DW, Ph illip s P, Ton k in A, Z im m et PZ ,
S h a w JE. A s s o c i a t i o n b e t w e e n i m p a i r e d g l u c o s e
m et ab olism an d q u alit y of lif e: r esu lt s f r om t h e Au st r alian
d i a b e t e s o b e si t y a n d l i f e st y l e st u d y. D i a b e t e s Re s Cl i n
Pr a c t 2 0 0 6 ; 7 4 ( 2 ) : 1 5 4 - 6 1 .
3. Roby n JT, Dav id WD, Pat P, Andr ew T, Paul ZZ, Jonat han
ES. Associat ion bet w een im pair ed glu cose m et abolism an d
quality of life: Results from the Australian diabetes obesity and
lifest yle st udy. Diabet es Res Clin Pract , 2006; 74: 154- 61.
4. Lugo LH, Garcia HI , Gom ez C. Calidad de vida y calidad de
v id a r elacion ad a com la at en ción em salu d . I at r eia 2 0 0 2 ;
1 5 ( 2 ) : 9 6 - 1 0 2 .
5 . H o l m e s S. Asse ssi n g t h e q u a l i t y o f l i f e – r e a l i t y o r
im possible dream ? A discussion paper. I nt J Nurs St ud 2005;
4 2 : 4 9 3 - 5 0 1 .
6. Boyer JG, Earp JA. The developm ent of an I nst rum ent for
A s s e s s i n g t h e Qu a l i t y o f Li f e o f Pe o p l e w i t h D i a b e t e s
( Diab et es 3 9 ) . Med Car e 1 9 9 7 ; 3 5 ( 5 ) : 4 4 0 - 5 3 .
7. López- Car m ona JM, Rodr igíguez- Moct ezum a R. Adapt at ion
an d v alidat ion of qu alit y of life in st r u m en t Diabet es 3 9 for
Mexican pat ient s w it h t ype 2 diabet es m ellit us. Salud Publica
Mex 2 0 0 6 ; 4 8 : 2 0 0 - 1 1 .
8 . Gu i l l e m i n F, Bo m b a r d i e r C, Be a t o n D. Cr o ss- cu l t u r a l
adapt at ion of healt h- relat ed qualit y of life m easures: lit erat ure
r e v i e w a n d p r o p o se d g u i d e l i n e s. J Cl i n Ep i d e m i o l 1 9 9 3
D ecem b er ; 4 6 ( 1 2 ) : 1 4 1 7 - 3 2 .
9 . Pa s q u a l i L. Pr i n c íp i o s d e e l a b o r a ç ã o d e e s c a l a s
p sicológ icas. Rev Psiq Clin 1 9 9 9 ; 2 5 ( 5 ) : 2 0 6 - 1 3 .
1 0 . Ech ev ar r ía- Gu an ilo ME, Rossi LA, Dan t as RAS, San t os
CB. Cr o ss- cu l t u r al ad ap t at i o n o f t h e Bu r n s Sp eci f i c Pai n
An x i et y Scal e - BSPAS t o b e u sed w i t h Br azi l i an b u r n ed
pat ien t s. Rev Lat in o- am En f er m agem 2 0 0 6 ; 1 4 ( 4 ) : 5 2 6 - 3 3 .
11. Terwee CB, Bot SD, de Boer MR, van der Windt DA, Knol
DL, Dek k er J, Bou t er LM, de Vet HC. Qu alit y cr it er ia w er e
p r o p o se d f o r m e a su r e m e n t p r o p e r t i e s o f h e a l t h st a t u s
qu est ion n air es. J Clin Epidem iol. 2 0 0 7 ; 6 0 ( 1 ) : 3 4 - 4 2 .
1 2 . Pa s q u a l i L. Pr i n c íp i o s d e e l a b o r a ç ã o d e e s c a l a s
p sicológ icas. Rev Psiq Clin 1 9 9 8 ; 2 5 ( 5 ) : 2 7 - 3 6 .
1 3 . Med i n a CME. Ad ap t ação t r an scu l t u r al e v al i d ação d o
inst r um ent o genér ico de m ensur ação de Qualidade de Vida
Re l a c i o n a d a à S a ú d e , D I S A B K I D S 3 7 p a r a c r i a n ç a s /
adolescent es m ex icanos com doenças cr ônicas e seus pais/
cuidadores: fase I [ Tese de Dout orado] . Ribeirão Pret o: Escola
de Enferm agem de Ribeirão Pret o, Universidade de São Paulo;
2 0 0 7 .
14. Wor ld Healt h Or ganizat ion. Phy sical St at us: t he use and
in t er p r et at ion of An t h r op om et r y. Rep or t of a WHO Ex p er t
Com m it t ee. Gen ev a: WHO; 1 9 9 5 .
15. Fayers PM, Machin D. Qualit y of life assessm ent , analysis
and int er pr et at ion. England. John Wiley ; 2000.
1 6 . Nov at o TS, Gr ossi SAA, Kim u r a M. Cu lt u r al adapt at ion
an d v alidat ion of t h e “ Diabet es Qu alit y of Lif e f or You t h s”
m easur e of I nger soll and Mar r er o int o Br azilian cult ur e. Rev
Lat in o- am En f er m ag em 2 0 0 8 ; 1 6 ( 2 ) : 2 2 4 - 3 0 .