r e v b r a s o r t o p . 2017;52(5):535–537
SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Original
article
Fat
embolism
syndrome
in
femoral
shaft
fractures:
does
the
initial
treatment
make
a
difference?
夽
Jânio
José
Alves
Bezerra
Silva
∗,
Diogo
de
Almeida
Diana,
Victor
Eduardo
Roman
Salas,
Caio
Zamboni,
José
Soares
Hungria
Neto,
Ralph
Walter
Christian
IrmandadedaSantaCasadeMisericóridiadeSãoPaulo,SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received29July2016 Accepted30August2016
Availableonline14September2017
Keywords:
Femoralfractures Fracturefixation Multipletrauma Fatembolism
a
b
s
t
r
a
c
t
Objective:Toidentifytheriskfactorscorrelatedwiththeinitialtreatmentperformed.
Methods:This isa retrospective study involvinga total of272patients diagnosed with femoralshaftfractures.Ofthepatients,14%werekeptatrestuntilthesurgicaltreatment, 52%underwentexternalfixation,10%receivedimmediatedefinitivetreatment,and23% remainedinskeletaltraction(23%)untildefinitivetreatment.
Results:Thereweresixcasesoffatembolismsyndrome(FES), whichshowedthat poly-traumaisthemainriskfactorforitsdevelopmentandthatinitialtherapywasnotimportant.
Conclusion: PolytraumapatientshaveagreaterchanceofdevelopingFESandtherewasno influencefromtheinitialtreatment.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
Síndrome
da
embolia
gordurosa
na
fratura
diafisária
de
fêmur:
o
tratamento
provisório
faz
diferenc¸a?
Palavras-chave:
Fraturasdofêmur Fixac¸ãodefratura Traumatismomúltiplo Emboliagordurosa
r
e
s
u
m
o
Objetivo:Identificarosfatoresderiscoecorrelacioná-loscomotratamentoinicial.
Métodos:Estudo retrospectivo que envolveu 272 pacientes com diagnóstico de fratura diafisáriadefêmur;14%permaneceramemrepousoatéotratamentocirúrgico,52%foram submetidos afixac¸ãoexterna,10%fizeramotratamentodefinitivoimediatoe23% per-maneceramcomtrac¸ãoesqueléticaatéotratamentodefinitivo.
Resultados: Foramseiscasosdesíndromeda emboliagordurosa(SEG), nosquaisse evi-denciouqueopolitraumaéoprincipalfatorderiscoparaseudesenvolvimentoequeo tratamentoinicialinstituídonãooinfluenciou.
夽
PaperdevelopedatSantaCasadeSãoPaulo,DepartamentodeOrtopediaeTraumatologia,GrupodeCirurgiadoTrauma,SãoPaulo, SP,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](J.J.Silva). http://dx.doi.org/10.1016/j.rboe.2016.08.021
536
rev bras ortop.2017;52(5):535–537Conclusão: Pacientespolitraumatizadosapresentaramumamaiorchancededesenvolver SEGenãohouveinfluênciadotratamentoinicialinstituído.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Thereleaseoffattyemboliintothebloodstreamcanleadto lesionanddysfunctionofoneormoreorgans,definedasfat embolismsyndrome(FES),mainlyduetothemobilityinthe focusofthefracture1;however, despitenewprotocols with
aggressivesupportandintensivetherapy,itremainsaconcern inshaftfracturesoflongbones.2–4Thus,earlyskeletal
stabi-lizationissuggestedtopreventthissyndrome.1However,the
decisionontheapproachtobeuseddependsonthepatient’s clinicalpictureandavailabilityofresources.5
Thepresentstudyaimsatidentifyingtheriskfactorsfor fatembolism syndrome,and tocorrelateitwiththe initial treatmentestablished.
Casuistry
and
method
This is a retrospective observational study based on data frompatients’recordsfrom theDepartmentofOrthopedics andTraumatology, seen betweenJanuary2011and Decem-ber2015.Theinformationcollectedincludesepidemiological data,traumamechanism,fractureclassificationaccordingto theAOclassification,6treatmentused,andclinicaloutcome
regardingthepresenceorabsenceofFES.
Patientswithadiagnosisoffemoralshaftfractureofboth genders,withaminimumageof16yearswereincluded,and patientswithafractureinapathologicalbonewereexcluded. Two groupswere considered:polytraumatized and non-polytraumatized. The former group included those with multiplelesionsexceedingadefinedseverity(ISS≥17).6
Regarding the initial treatment, they were divided into: rest (patients who were kept resting in bed with cush-ions), transtibial skeletal traction; external fixation for damage control, and definitive surgical treatment, either withintramedullarynail or fixationwithplate andscrews. No patient was definitively treated with external fixation (Table1).
Table1–Distributionofpatientsastoinitialtreatment.
Initialtreatment n %
Rest 39 14.3
Externalfixation 144 52.9
Definitive 27 9.9
Skeletaltraction 62 22.8
n,numberofpatients.
Source:Dataobtainedfrommedicalrecordsstudied.SAME,ISCMSP andHEFR.
Ofthepatients,272patientswhosemedicalrecordswere reviewed met the inclusion criteria. There were 43 (16%) femalepatientsand229(84%)malepatients.Asfortheage group,theywerepredominantlybetween16and30years(63%) (Table2).FESwasevidencedinsixcases(2.2%).
Regardingthemechanismoftrauma,therewasa predom-inanceofvictimsofmotorcycleaccidents(57%),followedby caraccidents(17%),andfalls(14%).
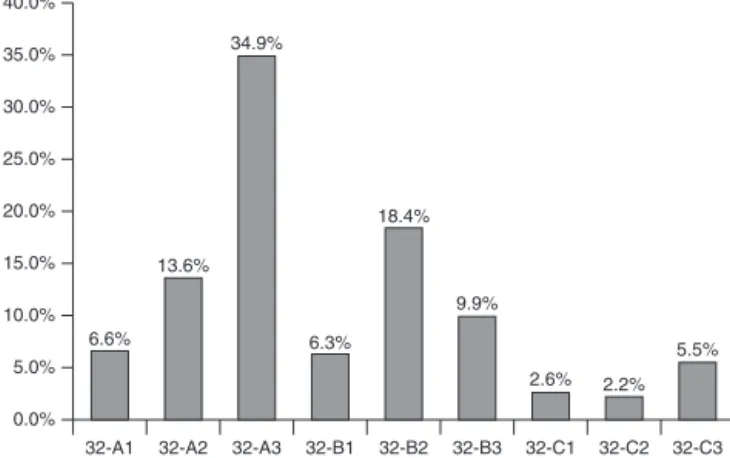
WeusedtheAO6groupclassificationforthefracturesand
obtainedthefollowingdistributionaccordingtoFig.1. Forty-three patients were considered polytraumatized (ISS>17)(16%),and67(25%)hadcompoundfractures.
Results
Five out of229 male patients(2.2%) developedFES,and in thegroupof43femalepatientsweobservedonlyone(2.3%) (p=0.954).
TherewasaprevalenceofFESinadults,mainlybelow30 years(83.3%),butwithoutstatisticalsignificance(p=0.302).
Considering only the fact that the patient was poly-traumatized as a variable, out of 43, five (12%) developed FES, and in the non-polytraumatized group, only one did (p<0.001).
Sixpatients(4%)developedFES,fivewerepolytraumatized, ofthe144casesundergoingexternalfixationasinitial treat-ment.
Inthegroupof43polytraumatizedpatients,30underwent externalfixation,andofthesefive(17%)developedFES.Inthe remainderofthegroup(13patients),fourweresubmittedto bedrest,fourhaddefinitivetreatmentintheemergencyroom, fiveunderwentskeletaltraction,butnoneofthesecaseshad FES.
Regarding theAOclassification,6 patientswithFESwere
distributedbetween32-B2(50%),32-A2(33%)and32-A3(17%). WedidnotfindcasesofFESamongpatientswithfractures classifiedas32-C.
Table2–Distributionofpatientsbyagegroup.
Agegroup n %
16–30years 172 63.2
31–40years 48 17.6
41–50years 19 7.0
51–60years 10 3.7
Over61years 23 8.5
n,numberofpatients.
rev bras ortop.2017;52(5):535–537
537
0.0% 6.6%
13.6% 34.9%
6.3% 18.4%
9.9%
2.6% 2.2% 5.5%
32-A1 32-A2 32-A3 32-B1 32-B2 32-B3 32-C1 32-C2 32-C3 5.0%
10.0% 15.0% 20.0% 25.0% 30.0% 35.0% 40.0%
Fig.1–DistributionofpatientsbyAOclassification.
Source:Datafrommedicalrecordsstudied.SAME,ISCMSP
andHEFR.
Discussion
FES is related to multiple factors, such as trauma energy, patient predisposition and initial resuscitation.1,7 Pinney
etal.8describedthatthereisarelationofFESinyoungadult
patients,becausetheyareabletosurvivehighenergytraumas, whichfavorsthissyndrome.Ourstudyshowedthatamongthe sixpatientswithFES,fivewerelessthan30yearsold,butthis wasalsotheageatwhichthisfracturewasmoreprevalent, with172patients(63%).Thus,thereisapredominanceofFES inthegroupofyoungadults,butwithoutstatistical signifi-cance(p=0.302).Thesamewasobservedforthemalegender, inwhichfemoralshaftfractures weremorecommon (84%) andaccountfor83%ofpatientswithFES.
Theinitialmanagement ofapatientwith femoralshaft fracturedependsontheclinicalconditionsoftheirhospital admission,takinginto accountthe conceptsalready estab-lishedintheliteratureofEarlyTotalCareandDamageControl. In the patients submitted to definitive primary treatment, therewasnoFES,whichcorroboratesstudiesbyBoneetal.9
andLasanianosetal.7Theydemonstratedthattheearly
fixa-tionoftheindividualfemoralshaftfractureinstablepatients maybebeneficial.
Inthegroupofpatientswithindicationoftemporary fixa-tion,Scannelletal.demonstratedthattherewasnodifference inclinicaloutcomesinpatientsundergoingbothexternal fix-ation(EF)and skeletal traction.10 Inourstudy,therewas a
higherprevalenceofFESinEFpatients(p<0.02),andnocases ofFESinthoseundergoingskeletaltraction,orbedrest. How-ever,amongthepatientsundergoingEF,in144(sixwithFES), 30werepolytraumatized(fivewithFES),whichwasconsidered themostimportantfactor(p=0.016).
Regarding the classification of fractures (classification AO6),whichtakesintoaccounttheenergyofthetrauma, a
higherprevalenceoftypeCfractureswasexpectedinpatients withFESbecausetheyarefractures withgreater instability andgreatermobilityinthefocus;therefore,agreaterrelease offatemboli isexpected.1,6 However,inourstudy,typeB2
fractures werethe mostprevalent intheFESpatientgroup (50%),butamongthese50patientswithfractureclassification AO32-B2,eightwerealsopolytraumatized(twowithFES),and 42 non-polytraumatized(one withFES).If wewere to mea-suretherelationshipbetweenembolismandpolytraumain this groupoffractures,therewasnostatisticalsignificance betweenthesevariables(p=0.098).
Conclusion
ThepolytraumatizedpatientismorelikelytodevelopFES,and inourcasuistrytheinitialtreatmentdidnotinfluenceinits development.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.WhiteT,PetrisorBA,BhandariM.Preventionoffatembolism syndrome.Injury.2006;37Suppl.4:S59–67.
2.RobinsonCM.Currentconceptsofrespiratoryinsufficiency syndromesafterfracture.JBoneJointSurgBr.
2001;83(6):781–91.
3.FilomenoLTB,CarelliCR,SilvaNCLF,BarrosFilhoTEP, AmatuzziMM.Emboliagordurosa:umarevisãoparaaprática ortopédicaatual.ActaOrtopBras.2005;3(4):96–208.
4.SaigalR,MittalM,KansalA,SinghY,KolarPR,JainS.Fat embolismsyndrome.JAssocPhysIndia.2008;56:245–9. 5.PapeHC,GiannoudisPV,KrettekC,TrentzO.Timingof fixationofmajorfracturesinbluntpolytrauma:roleof conventionalindicatorsinclinicaldecisionmaking.JOrthop Trauma.2005;19(8):551–62.
6.RuediTP,BuckleyR,MoranCG.AOprinciplesoffracture management.2nded.NewYork:Thieme-Verlag;2007. 7.LasanianosNG,KanakarisNK,DimitriouR,PapeHC,
GiannoudisPV.Secondhitphenomenon:existingevidenceof clinicalimplications.Injury.2011;42(7):617–29.
8.PinneySJ,KeatingJF,MeekRN.Fatembolismsyndromein isolatedfemoralfractures:doestimingofnailinginfluence incidence?Injury.1998;29(2):131–3.
9.BoneLB,JohnsonKD,WeigeltJ,ScheinbergR.Earlyversus delayedstabilizationoffemoralfractures:aprospective randomizedstudy,1989.ClinOrthopRelatRes. 2004;(422):11–6.