REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
PublicaçãoOficialdaSociedadeBrasileiradeAnestesiologiawww.sba.com.br
CLINICAL
INFORMATION
Multimodal
therapeutic
approach
of
vaginismus:
an
innovative
approach
through
trigger
point
infiltration
and
pulsed
radiofrequency
of
the
pudendal
nerve
Joana
Chaves
Gonc
¸alves
Rodrigues
de
Carvalho
∗,
Luís
Miguel
Agualusa,
Luísa
Manuela
Ribeiro
Moreira,
Joana
Catarina
Monteiro
da
Costa
HospitalPedroHispano,DepartamentodeAnestesiologia,Matosinhos,Portugal
Received7July2014;accepted2October2014 Availableonline16September2016
KEYWORDS
Vaginismus; Pulsed
radiofrequency;
Pudendalnerve;
Triggerpoint;
Chronicpain
Abstract Vaginismusisapoorlyunderstooddisorder,characterizedbyaninvoluntarymuscular spasmofthepelvicfloormusclesandouterthirdofthevagina duringintercourseattempt, whichresultsinaversiontopenetration.Itisreportedtoaffect1---7%ofwomenworldwide. Withthisreporttheauthorsaimtodescribethecaseofayoungpatientwithvaginismusin whomtechniquesusuallyfromthechronicpaindomainwereusedaspartofhermultimodal therapeuticregimen.
©2015SociedadeBrasileiradeAnestesiologia.PublishedbyElsevierEditoraLtda.Thisisan openaccessarticleundertheCCBY-NC-NDlicense( http://creativecommons.org/licenses/by-nc-nd/4.0/).
PALAVRAS-CHAVE
Vaginismo; Radiofrequência pulsada;
Nervopudendo;
Pontogatilho;
Dorcrônica
Terapêuticamultimodaldovaginismo:abordageminovadorapormeiodeinfiltrac¸ão depontosgatilhoeradiofrequênciapulsadadonervopudendo
Resumo Ovaginismoéumadoenc¸apoucocompreendidaquesecaracterizaporumacontrac¸ão muscularinvoluntáriadosmúsculosdopavimentopélvicoedoterc¸oexternodavaginadurante astentativasdeintercursosexual,oqueresultaemaversãoàpenetrac¸ão.Estima-sequepossa afetar entre1%-7% dapopulac¸ão femininamundial. Com esterelato os autores pretendem apresentarocasodeumapacientejovemcomvaginismonaqualforamusadastécnicas habit-ualmentedo domínio da medicinada dorcrônica como partedo seu esquema terapêutico multimodal.
©2015SociedadeBrasileiradeAnestesiologia.PublicadoporElsevierEditoraLtda.Este ´eum artigoOpen Accesssobumalicenc¸aCCBY-NC-ND( http://creativecommons.org/licenses/by-nc-nd/4.0/).
∗Correspondingauthor.
E-mail:[email protected](J.C.Carvalho).
http://dx.doi.org/10.1016/j.bjane.2014.10.011
Introduction
Vaginismus is a disorder characterized by involuntary contractionof thepelvicfloorandvaginalmuscles,which makessexintercoursedifficult or impossible.1 Althoughit was firstdescribed over 100 years ago, it remains poorly diagnosedandundertreated,afactthatbecomesmore rel-evant if one takes into account that compared to other sexualdisorders,especiallyofdesireandorgasm,itappears to be one whose treatment has the greatest potential for success.2 Several treatmentshave been usedover the years,includingsexualtherapy,desensitization, hypnother-apy,vaginaldilatorsandinjectionofbotulinumtoxin,among others.2,3Nevertheless,theoptimalapproachhasnotbeen determined,and both ourclinical experienceandcurrent international literature point toward the pulsed radiofre-quency (PRF) becauseits neuromodulatory properties are usefulinthetreatmentofrefractorypain.4---7
Clinical
case
Femalepatient,29yearsold,nulliparous,ASAIIdueto dia-betesmellitus(DM)typeIsinceadolescence,takinginsulin withgoodglycemiccontrolinoutpatientservice,andwith a history of repeated vaginal infections. The patient was referencedtothePainMedicineUnit(PMU)ofourinstitution duetocomplaintsofvulvodyniaanddyspareuniawithtwo yearsofevolution.Shehadnohistoryofaggression,trauma oraccident;hadsurgicalhistoryofconization.Atthetime ofreferral, shewasattendingpsychiatricandgynecologic consultations and in treatment with estazolam, escitalo-pramandtopicaldibucaineforusebeforesexintercourse. She described a self-limited and only temporary reliefof painsymptomswiththelatterdrug.
At thephysical examination,thepatienthada marked sensitivityinthelowerhalfofthevaginalintroitus,disabling and limiting for clinical observation itself, andshe toler-atedwithdifficulty,forexample,digitalorcompressvaginal examination.Inthiscontext,infiltrationofthevaginal trig-gerpoints(TP)wasproposed.Thetechniquewasperformed undersedationintheoutpatientunit(Fig.1),andconsisting ofinfiltration oftheintroitusatfour,five,six,seven,and eighto’clock markers, with 0.2% ropivacaine(2mg.mL−1) andclonidine(100g).Nocomplicationswererecorded dur-ingthisprocedure.Fourmonthsafter,thepatientreported improvementofvulvodynia,butvaginismuswaspresentat thephysicalexamination.Thus,shewasadvisedtoundergo individual hypnotherapy sessions and bilateral PRF of the pudendalnerve,whichsheaccepted.
On procedure day, upon arrivaltothe operatingroom, thepatientwaspremedicatedwithintravenous(IV)fentanyl (0.05mg)andmidazolam(1mg)andplacedingynecological position. Subsequently, she was anesthetizedwith propo-fol bolus, a total of 270mg IV. After proper disinfection, theischialspine(IS)andinsertionpointofthesacrospinous ligament were identified transvaginally. Medially to IS, a 23G radio frequency needle with 10cm long and 0.5cm activetipwasintroducedgradually,with2Hzmotor stimu-lusuntilpudendalnerveidentification,visuallyconfirmedby theoccurrenceofcontractionoftheexternalanal sphinc-ter muscle (Fig. 2). Subsequently, an alternating current
Figure1 Patientattheoutpatientunit,underdeepsedation totriggerpointinfiltration.Duringtheprocedure,anAmerican SocietyofAnesthesiologistsstandardmonitoringwasused.
wasappliedbilaterallytothepudendalnervesfor240s(2 cyclesof120s).Ithasbeeninfiltratedalso,forthesecond time,aTPatfiveandseveno’clock with0.2%ropivacaine and methylprednisolone acetate (Depo-Medrol®) (Fig. 3).
The procedure waswell tolerated by the patient,and no complicationswerereported.
Inthefirst12monthsoffollow-up,thepatientreported significant clinical improvement and managed using pro-gressivesizedilatorsandattemptedpenetration.Thepain complaintswerelimitedtothevaginalvault.Fromthe13th month, the pain intensity increased, although toa lower thresholdthanwhenshewasinitiallyreferredtothePMU. Giventhesecircumstances,itwasdecidedtorepeatthePRF withthesameprotocolusedinthefirstintervention.Five monthslater,thepatienthasnotrequiredanew differenti-atedinterventionbythePMU.
Discussion
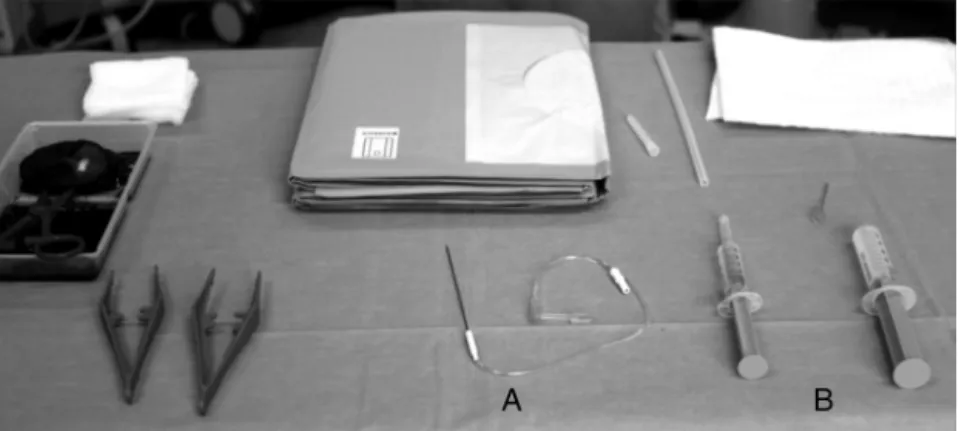
Figure2 Radiofrequency(RF)materials.IntheimageitispossibletoseetheRFneedle(A),aswellasthesyringewith0.2% ropivacaineandDepomedrol® (B)toinfiltrationoftriggerpoints.
Figure3 RFneedleplacedjuxtaposedtothepudendalnerve duringemissionofalternatingelectriccurrent(A).Infiltration ofatriggerpoint(B)isalsodisplayed.
manyofthesepatientstendtobequitereservedandnotto sharetheirhealthproblem.3
Vaginismustendstobeapsychosomaticproblem.Thatis, althoughinahighpercentageofcasestheetiologyappears toberelatedtopsychologicalproblemsthespasmodic reac-tion preventing penetration is physical.8 Psychologically, manyof thesewomen sharea historyof traumaticsexual intercourse,sexualaversionorfamilyand/orreligious neg-ativeconstraints regardingsex, a historynotdescribed in ourcase.3,8
However, the etiology may also be primarily physical. In fact, women with suspected diagnosis should be the subjectofcarefulexamination,asabasicassessment can-notfindsupportfortheircomplaints.8Possiblepainorigins aremalformationsofthehymen,clitorisor labia;sexually transmitted diseases; endometriosis; pelvic inflammatory disease; cancer; insufficient lubrication; vaginal atrophy or abnormal wound healing.3,8 Furthermore, our patient has DM, an endocrinopathy with multiple microvascular complications,particularly neuropathy.In a meta-analysis publishedin2013byNguyenetal.,fibromyalgiaandirritable bowelsyndromeweresignificantlyidentifiedas comorbidi-ties present in patients with history of vulvodynia.9 This relationshipwasnotfoundforDM,fornotbeingsought,but,
theoretically,theremightbearelationshipconsideringthat both arechronic medicalconditionsdifficult totreat,and theadjectiveschosentodescribevulvarpain(excruciating, burning,tingling)refertoaneuropathiccause.10Eitherbya directorindirectmechanism,forexample,thegreater pre-dispositiontorecurrentvaginal/urinaryinfectionsreported bythispatient,DMseemstobeacauseofvulvodynia.3,8,10
Inthe presenceof oneor moreof the aforementioned predisposing factors, women mayexperience painful sen-sations. Subsequently, the fear of the painful sensation is fixed in sexual intercourse anddevelops an involuntary ‘‘flight or fight’’ reaction whenever there is a possibil-ityofpenetration.8Furthermore,increasedmuscletension secondary topersistent fear of pain, associated with the inability torelax, maybeinvolved in the developmentof smallareasofmusclecontracture,theTP.11
The clinician should keep in mind that penetration not only includes the form that characterizes a sex-ual intercourse(penis×vagina).8Indeed,accordingtothe updatedDiagnosticandStatistical ManualofMental Disor-ders(DSM-5),anyformofpenetration,eitherusingfingers, tampons,vaginalspeculaorextenders,canbeparticularly difficult.2,3,12 This demanded adjustments in the patient assessmentmode,atleastintheinitialphaseofmonitoring, allinordertofosterarelationshipoftrustnecessaryforthe progressoftreatment.
achieving the firsttwo goals, while TP infiltration associ-ated withPRF andgradual use of dilatorsthekey behind thedesensitizationprocess.
AccordingtooursurveyconductedinPubMed,theuseTP infiltrationandPRFofpudendalnervehasneverbeen previ-ouslydescribedaspartofmultimodaltherapeuticstrategy for vaginismus, which reinforces the importance of this report.
TPareintheoriginofmyofascialsyndromesanddefined aslimitedareasof hyperirritability,withfirmconsistency, inside the striated muscles, tendonsor fascia.11 Although more often described in the scapular, lumbar and gluteal areas,theymaybepresentinanyanatomicalregion, par-ticularlyperineal,anddevelop secondarytoacutetrauma or repeated microtrauma,11 particularly increased muscle tension.
Althoughthecausedpainmaybeconstant,itoftenarises onlywhenthereismuscleactivity,suchasduringsex inter-courseorwhenthesetinynoduleformationarepalpated,as inthegynecologicalexamination.11Thepainmaybelocalor referredareasandisassociatedwithaslightcontraction,10 findingsthatwereseeninourpatientontheinitialphysical examination.
In thispatient,theTP managementdecisiondepended notonly onteamexperience,butalsoonitsverynature. Indeed,although thelong-termbenefits ofdifferent ther-apeutictechniquesarequestionable,thechronicityofthe patient’sTP ledthe teamtooptfor infiltrationwithlocal anesthetic andsteroid,a technique reportedasproviding agreater painrelief.11 Infact,physiotherapy and manual therapyaremoresuitableforacutesituations,patientswith fearofneedles,orTPinnoteasilyaccessiblemuscle bun-dles,notpresentinourthecase.11
The radio frequencytechnique (RF)is arelatively new treatmentmodalitybasedonadministrationof ahigh fre-quency alternating current in the vicinity of a nerve or ganglion structure.5---7 Although itsmechanism ofaction is notfullyunderstood,itseemstobebasedontheprinciple ofneuromodulation; thatis,change insignal transduction andtransmissionalongthepainpathways.6
This currentcanbeadministeredintwomajorand dis-tinct forms. Incontinuous RF, the current is administered to produce a thermal lesion on the target tissue, block theconductionofnociceptivesignalandprovidepainrelief while nerveterminals do not regenerate.6,7 In pulsed RF, thecurrentisintermittent,thereisheatdissipation,andno developmentofneuralcoagulationThecellularmorphology of the tissueis maintained. However,it causes molecular alterationsin theexpressionof sometranscription factors thatculminateinchangeinpainsignaltransduction.6
RF techniques are currently used as a therapeutic tool in many chronic pain syndromes and, despite the paucity ofrandomizedcontrolledtrials, numerousreports of RF applied to peripheral nerve structures prove its effectiveness.4---6
Thepudendalnerve,consistingoftheposteriorbranches ofthesacredrootsS2, S3andS4,isresponsibleformotor innervationoftheperinealmusclesandsensoryinnervation ofthe lowerportionofthevagina,vulva, andperineum.4 Becausethesewere theanatomicregions ofourpatient’s complaints, the choice of this nerve for our therapeutic approachiswarranted.
We optedfor apulsed technique given thatit is more innocuousand notassociated withrisk of motor damage, complicationsreportedwithcontinuousRF.Theoccurrence of a motor damage would have devastating effects on the patient’s already poor quality of life, as its clinical translationcouldinclude, amongother findings,sphincter incontinence.6
OtheradvantagesthatinfluencedthechoiceofpulsedRF arerelatedtothefactthatitisaminimallyinvasive tech-nique, safeand well tolerated, which can be repeatedif thereisrecurrenceofcomplaints.4---7Thislatter characteris-ticwasusedinthiscase.Onepotentialdrawbackassociated withthisblockadeisitstechnicaldifficulty,whichmaylead toa significant failure rate when performed by inexperi-encedteams.6
Thepaincomplaintsimprovementreflectedinother per-sonal aspects of the patient’s life. Thus, not only it was possibletoadvanceinthepharmacologicaldesensitization strategy and suspend the benzodiazepines taken by the patient,butan improvement of herself-esteemand self-assurancewasalsoobserved.Indeed,itisimportantthatthe medicalteamdonotneglecttheemotionalchargeentailed bythissyndrome.Patientsoftenpresentwithadiminished imageofthemselvesassociatedwithfeelingsofshame.8
Itisalsoessentialthat thepartnersareincluded atall stages oftreatment, as we tryto do,8 either by the sim-plecoexistenceorbypositivefeedbackmechanisms.Asthe patient’ssexualitydevelopsand grows,more safe,happy, andfulfilledwillbethecouple.8
In summary, we can say that although this is a single report,TP infiltrationand PRFofpudendalnerveseem to beapotentialadjuvanttherapeutictoolinthemanagement ofvaginismus.Inourcase,itprovidedtothepatientapain reliefsuperiortoanyotherexperiencedtechnique.
In order that the therapeutic effectiveness of these casesincreasesandminimizesthephysicaland psychologi-calsequelaedevelopedbythesewomeninthemediumand longterm,itisessentialalsotoimprovethediagnostic abil-ityofhealthprofessionals.Thus,asdescribedbyPacik,itis necessarythatduringtheyearsoftraining,pre-and post-graduation,professionals are able to recognize and treat thissyndromeintheshortestpossibletime.2
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.MelnikT,HawtonK,McGuireH,etal.Interventionsfor vaginis-mus.CochraneDatabaseSystRev.2012;12:CD001760. 2.PacikPT. Vaginismus:another ignoredproblem.Sex Culture.
2014;18:737---8.
3.PacikPT.Vaginismus:reviewofcurrentconceptsandtreatment usingbotoxinjections,bupivacaineinjections,andprogressive dilationwiththepatientunderanesthesia.AesthPlastSurg. 2011;35:1160---4.
5.Cahana A, VanZundert J, Macrea L, et al. Pulsed radiofre-quency:currentclinicalandbiologicalliteratureavailable.Pain Med.2006;7:411---23.
6.ReaW,KapurS,MutagiH.Radiofrequencytherapiesinchronic pain.ContinEducAnaesthCritCarePain.2011;11:35---8. 7.ByrdD,MackeyS.Pulsedradiofrequencyforchronicpain.Curr
PainHeadacheRep.2008;12:37---41.
8.SilvaMCA.Vaginismo/dispareunia.RevSocBrasEstudSexHum. 2009;20:143---8.
9.Nguyen RH, Veasley C, Smolenski D. Latent class analysis of comorbiditypatterns amongwomen withgeneralized and localizedvulvodynia:preliminaryfindings.JPainRes.2013;6: 303---9.
10.Kalra B, Kalra S, Bajaj S. Vulvodynia: an unrecognized diabetic neuropathic syndrome. Indian J Endocrinol Metab. 2013;17:787---9.
11.AlvarezDJ,RockwellPG.Triggerpoints:diagnosisand manage-ment.AmFamPhysician.2002;65:653---61.
12.Araújo AC,Neto FL. Anova classificac¸ãoamericana para os transtornos mentais --- o DSM-5. Rev Bras Ter Comp Cogn. 2014;XVI:67---82.
13.PereiraVM,Arias-CarriónO,MachadoS,etal.Sextherapyfor femalesexualdysfunction.IntArchMed.2013;6:37.