ww w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Original
article
Locomotive
syndrome
in
the
elderly:
translation,
cultural
adaptation,
and
Brazilian
validation
of
the
tool
25-
Question
Geriatric
Locomotive
Function
Scale
Daniela
Regina
Brandão
Tavares
a,∗,
Fania
Cristina
Santos
baUniversidadeFederaldeSãoPaulo(UNIFESP),ProgramadeGeriatria,SãoPaulo,SP,Brazil
bUniversidadeFederaldeSãoPaulo(UNIFESP),Servic¸odeDoreDoenc¸asOsteoarticulares,DisciplinadeGeriatriaeGerontologia(DIGG),
SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received26January2016 Accepted23May2016 Availableonline1August2016
Keywords: Elderly
Locomotivesyndrome GLFS-25
Assessmenttool
a
b
s
t
r
a
c
t
Objective:ThetermLocomotiveSyndromereferstoconditionsinwhichtheelderlyareat highriskofinabilitytoambulateduetoproblemsinlocomotorsystem.ForLocomotive Syndromescreening,the 25-QuestionGeriatricLocomotiveFunctionScalewascreated. Theobjectiveherewastotranslate,adaptculturallytoBrazil,andstudythepsychometric propertiesof25-QuestionGeriatricLocomotiveFunctionScale.
Method:Thetranslationandculturaladaptationof25-QuestionGeriatricLocomotive Func-tionScalewerecarriedout,thusresultinginGLFS25-P,whosepsychometricproperties wereanalyzedinasampleof100elderlysubjects.Sociodemographicdataonpain,falls, self-perceivedhealthandbasicandinstrumentalfunctionalitiesweredetermined.GLFS 25-Pwasappliedthreetimes:inonesamedaybytwointerviewers,andafter15days,again bythefirstinterviewer.
Result:GLFS25-PshowedahighinternalconsistencyvalueaccordingtoCronbach’salpha coefficient(0.942),andexcellentreproducibility,accordingtointraclasscorrelation,with interobserverandintraobservervaluesof97.6%and98.4%,respectively(p<0.01). Agree-ments foreach item of the instrument were considerable(between 0.248 and 0.673), accordingtoKappastatistic.Initsvalidation,accordingtothePearson’scoefficient,regular andgoodcorrelationswereobtainedforthebasic(BADL)andinstrumental(IADL) activi-tiesofdailyliving,respectively(p<0.01).Statisticallysignificantassociationswithchronic pain(p<0.001),falls(p=0.02)andself-perceivedhealth(p<0.001)werefound.A multivari-ateanalysisshowedasignificantlyhigherriskofLocomotiveSyndromeinthepresenceof chronicpain(OR15.92,95%CI3.08–82.27)andwithaworseself-perceivedhealth(OR0.23, 95%CI0.07–0.79).
Conclusion:GLFS 25-P proved to be a reliable and valid tool in Locomotive Syndrome screeningfortheelderlypopulation.
©2016PublishedbyElsevierEditoraLtda.ThisisanopenaccessarticleundertheCC BY-NC-NDlicense(http://creativecommons.org/licenses/by-nc-nd/4.0/).
∗ Correspondingauthor.
E-mail:[email protected](D.R.B.Tavares).
http://dx.doi.org/10.1016/j.rbre.2016.07.015
Síndrome
locomotora
em
idosos:
traduc¸ão,
adaptac¸ão
cultural
e
validac¸ão
brasileira
do
instrumento
25-
Question
Geriatric
Locomotive
Function
Scale
Palavras-chave: Idoso
Síndromelocomotora GLFS-25
Instrumentodeavaliac¸ão
r
e
s
u
m
o
Objetivo:Otermosíndromelocomotora(SL)designacondic¸õesnasquaisosidosos apresen-tamaltoriscodeincapacidadeparadeambulac¸ãoemdecorrênciadeproblemasemórgãos locomotores.Paraseu rastreiofoicriado o25-QuestionGeriatricLocomotiveFunctionScale (GLFS-25).Objetivou-seaqui,traduzir,adaptartransculturalmenteparaoBrasileestudaras propriedadespsicométricasdoGLFS-25.
Método: Feitastraduc¸ãoeadaptac¸ãotransculturaldoGLFS-25queoriginaramoGLFS25-P, cujaspropriedadespsicométricasforamanalisadasnumaamostrade100idosos.Apurados dadossociodemográficosrelativosador,queda,autopercepc¸ãodasaúdeefuncionalidades básicaeinstrumental.OGLFS25-Pfoiaplicadoemtrêsmomentos:nummesmodiapor doisentrevistadoreseapós15diasnovamentepeloprimeiroentrevistador.
Resultado: OGLFS25-Papresentoualtovalordeconsistênciainterna,segundoocoeficiente AlfadeCronbach(0,942);ereprodutibilidadeótima,segundoacorrelac¸ãointraclasses: val-oresde 97,6%e98,4%,interobservador eintraobservador,respectivamente(p<0,01).As concordânciasparacadaitemdoinstrumentoforamconsideráveis(entre0,248e0,673), segundoaestatísticaKappa.Navalidac¸ão,segundoocoeficientedePearson,foramobtidas correlac¸õesregulareboaparaasatividadesdevidadiáriabásicas(AVDB)einstrumentais (AIVD),respectivamente(p<0,01).Encontradasassociac¸õesestatisticamentesignificantes comdorcrônica(p<0,001),queda(p=0,02)eautopercepc¸ãodesaúde(p<0,001).Aanálise multivariadaevidenciouriscodeSLsignificativamentemaiornapresenc¸adedorcrônica (OR15,92,IC95%3,08–82,27)epiorautopercepc¸ãodesaúde(OR0,23,IC95%0,07–0,79). Conclusão: OGLFS25-PdemonstrouserconfiáveleválidonorastreiodaSLemidosos.
©2016PublicadoporElsevierEditoraLtda.Este ´eumartigoOpenAccesssobuma licenc¸aCCBY-NC-ND(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
TheagestructureoftheBrazilianpopulationhasundergone majorchangesoverthe past50years.Lifeexpectancy rose from 48 years in 1960 to 73.4 years in 2010. In the same period,thenumberofelderlyindividualsincreasedfrom3.3 million(4.7%ofthepopulation)to20.5million(10.8%ofthe population).Itisexpectedthatin2060thisvaluewillreach approximately73millionofelderlysubjects,accountingfor 33.7%ofthepopulation.1
Thisdemographictransitionhasanimportantimpacton publichealth.2Itisestimatedthatthenumberofolder peo-plewithfunctionaldependencyincreasesexponentiallywith theagingofthepopulation,whichwouldresultina signifi-cantfinancialburdentosociety.3Locomotorsystemdiseases arethemaincausesofdisabilityassociatedwithaging,and oneofthe main targets fortheir prevention.3,4 Data show that21.5%ofthesepatientshavesomediseaseofthe muscu-loskeletalsystemsuchasosteoporosis(andrelatedfractures), spondyloarthrosis,andosteoarthritis.5
Forthepreventionoflocomotivedysfunction,theJapanese OrthopedicAssociation(JOA)proposedin2007theconceptof “LocomotiveSyndrome”(LS)todescribetheconditionsunder whichtheelderlybecomedependentoncare,orareathigh riskofbecoming dependentinthefuture, duetoproblems inthelocomotorsystem.6Sevenwarningsignsthatindicatea highriskforLShavebeendescribed:notbeingabletoputona pairofsockswhilestandingononeleg;oftenstumblesorslips insidethehouse;needtouseahandrailwhengoingupstairs;
havedifficultyinperforminghouseholdactivitiesofmoderate intensity;finditdifficulttowalkhomecarryingashoppingbag weighingabout2kg;notbeingabletowalkcontinuouslyfor 15min;andnotbeingabletocrossthestreetbeforethetraffic lightchanges.7
Severalcampaignshavebeen conductedinJapanto dis-seminateLSamongthepopulation.InarecentInternetbased survey, JOA reported that only 26.6% of the Japanese pop-ulation knewabout LS.Even amongpatients inoutpatient centers,theidentificationofLSwasalsolow(24.6%).7
Thespecificcharacteristicsofthissyndromearenotfully known;however,itisbelievedthatLSissecondarytothemajor musculoskeletaldiseases.6Someofthesignsandsymptoms thatwouldallowanearlyidentificationare:pain,limitation ofjointmobility,andaslowerdeambulation.5
ForthescreeningforLS,Japaneseresearchersalso devel-opedanevaluationtool:the“25-questionGeriatricLocomotive Function Scale” (GLFS-25). This tool consists of a self-administered questionnaire with 25 items that are easily understoodbytheelderly,andeachitemisgradedfrom0to 4points.Thefinalscoreistheresultofthesumofallitems, rangingfrom 0to100;thehigher thescore,thehigher the physicalimpairmentoftheelderly,and16isthecutoffpoint forthediagnosisofLS.3
GLFS-25coversdifferentaspectsofthelastmonthofthe patient,with4questionsaboutpain,16questionsabout activ-itiesofdailyliving,3questionsaboutsocialperformanceand 2questionsabouthis/hermentalhealthstatus.3
worldisgoingthroughinthe last50 years.Itis,therefore, a concept that does not refer to traditional diseases, but ratherisabroadepidemiologicalconceptrelatedtothehealth systemmanagement.3Giventhistimeoftransition,the con-cernofhealthorganizationsrevolvesaroundhowtoincrease lifeexpectancy with healthand functional independence.8 Accordingly,thescreeningofthissyndromebecomescrucial inordertoallowtheimplementationofanearlyintervention.3 Thisstudyaimedatthetranslation,culturaladaptationto Brazil,andstudyofthepsychometricpropertiesofGLFS-25in theelderlyinourenvironment.
Materials
and
methods
Thisisanepidemiologic,observational,descriptiveand ana-lytical study approved by the Research Ethics Committee of the Universidade Federal de São Paulo/UNIFESP (CEP No.921,390/2014).
ForthetranslationandculturaladaptationofGLFS-25,the methodologyofGuilleminetal.9wasused.Initially,theitems oftheinstrumentintheEnglishlanguagehavebeen trans-latedintoPortuguesebytwoindependent,qualifiedBrazilian translatorswhowereawareofthetranslationgoals.The trans-lationsobtainedwere comparedtoeach other,resulting in aversionwhichwasagaintranslatedintoEnglishand com-paredtotheoriginalversion,astepcarriedoutbytwoothers nativeEnglishtranslatorswithknowledgeofthePortuguese language,andblindedfortheproposedobjectives.
Intermsofcross-culturaladaptation,someequivalences wereobtained:(1)semanticequivalence,basedonthe assess-mentofgrammaticalequivalenceandofvocabulary,asmany wordsofagivenlanguagemaynothaveequivalentinother languages;(2)idiomaticequivalence,basedonanextensive researchindictionaries,forthetranslationofcertainidioms isdifficult,andthemeaningofcertainwordsisnotfixednor stable;(3)cross-culturalorexperimentalequivalence,forthe cross-culturalcontextofcertainexpressionsshouldpresent “contentvalidity”alsoinPortugueseandforthepopulation of Brazil, and considering that the version of the original instrumentwould nowbeusedinacountry differentfrom that for which it was created; (4) conceptual equivalence, as many items may besemantically equivalent, but with-out“equivalenceofconcept”.Inthislaststage,acommittee composedofexpertsfromdifferentfields(Geriatrics, Orthope-dics,Rheumatology,Psychology,andPhysiotherapy)andwith experiencewiththeelderly,wasformed.Intheend,thefinal versionoftheinstrumentGLFS25-Pwasobtained(Table1).
Fortheanalysisofthepsychometricpropertiesofthenewly originatedBrazilianversion,elderlysubjectsaged60orover,of bothgenders,andseenonanoutpatientbasisintheDivision ofGeriatricsand Gerontology,Universidade Federal deSão Paulo–DIGG/UNIFESP,wererandomlyselected. Those sub-jectswithcognitiveandbehavioralimpairment,severeacute orchronicdecompensateddisease,limitingsensorydeficits, andhistory offracturesinthe lower limbsand/or spinein thelast6monthswereexcluded.Allparticipantssignedan informedconsent.
For the whole group of participants, demographic data (age,gender,maritalstatus,ethnicgroup,andeducation),and
functional statusfor basic (BADL) and instrumental (IADL) activitiesofdailyliving,accordingtoKatzandLawtonindices, respectively, were obtained.Data onthe frequency offalls in the last year, self-perceived health (poor, fair, good or excellent), and presenceofchronic pain (lasting 6months ormore)werecollected;forthislattervariable,itsintensity was recorded,according toaverbaldescriptivescale (mild, moderate,severeorverysevere).
GLFS25-Pwasadministeredbytwoindependent interview-ers(E1andE2),inonesameday;andafteraperiodof15days (duringwhichtherewasabsolutelynointervention)thethird applicationwasconductedbythefirstinterviewer(nowcalled E3).InthestudyofthepsychometricpropertiesofGLFS25-P, firstofall,itsreliabilitywasanalyzed,accordingtoits inter-nalconsistencyand reproducibility; andlaterits validation wascarriedout,takingintoaccountitsconstruct.Construct validity– astagecriticallyimportantinthevalidation pro-cess–involvescomparingtheinstrumenttobestudiedwith anestablished“goldstandard”,andwhenthisstandardisnot available,onemakesacomparisonagainstcommonlyused clinicalparameters.10Inthisstudy,theconstructvaliditywas obtainedbythecorrelationbetweenGLFS25-Pandfunctional indices,accordingtoBADLandIADL.
Regarding the statistical analysis, the Two-Proportion Equality Test was used in the distribution of the relative frequencyofqualitativevariables,andCronbach’salpha coef-ficient was applied to obtain the internal consistency. In addition,thePairedStudent’st-TestandtheIntraclass Corre-lationIndex(ICI)forintra-andinter-observerreproducibility, theKappacoefficientforreproducibilityofeachquestionof the instrument,and the Pearson’scorrelation for the vali-dationwerealsoemployed.TheassociationbetweenLSand chronicpain,thefrequencyoffallsinthelastyear,andwith different levels ofself-perceivedhealth was alsoevaluated withtheuseofthechi-squaredtestandbyalogisticregression analysis.Thelevelofsignificancewassetat0.05(5%).
Results
Inthisstudy,thesamplewascomposedof100elderlysubjects withamean ageof82±1.5(61–100)years,witha predomi-nanceoffemales(73%),Caucasians(50%),stateofwidowhood (52%),andlowlevelofeducation(meanof5.1years,57%had only1–4years)(Table2).
Asforthefunctionalityoftheparticipants,therewasa pre-dominanceofafunctionalindependencestatusunderBADL (96%, withamean of5.5±0.1points)andofmild depend-ence(41%,withameanof23.6±08points)accordingtoIADL (Table2).
Asfortheotherfeatures,61%hadchronicpain,considered mildby5%,moderateby33%,severeby42%,andverysevereby 20%;and15%ofparticipantswerechronicfallers(2ormore fallsinthepastyear).For theself-perception ofhealth,5% reporteditasbad,53%fair,36%goodand6%excellent.
Table1(Continued)
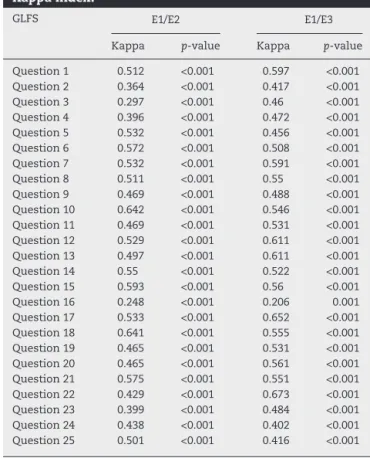
IntheanalysisofthepropertiesofmeasuresofGLFS25-P, andinitiallywithreferencetotheproperty“reliability” accord-ingtoitsinternalconsistency,highCronbach’salphavalues wereobtained:0.942forE1,0.952forE2,and0.949forE3.As toreproducibility,threeanalyseswerecarriedout.According tothe Paired Student’st-Test, whichcompared the means of GLFS 25-P in E1, E2, and E3, no statistically significant differences were found(Table 3). According to ICI, optimal results were obtained: 97.6% of inter-observer correlation (E1andE2)and98.4%ofintra-observercorrelation(E1andE3) (Table3).Intheagreementanalysisbetweeninterviewersfor each itemofthe instrument inquestion, considerable val-ueswerefound(between0.248and0.673)forKappastatistics (Table4).
Inthevalidationprocess,statisticallysignificant correla-tionswerefoundwiththefunctionalityindicesinbasicand instrumentalactivities,withregularindicesforBADL(>45%) andgoodindicesforIADL(>60%),accordingtothePearson’s coefficient.Suchcorrelationswerenegative,thatis,thehigher thescoresofGLFS25-P,thelowerthefunctionalindicesfor BADL and IADL(Table 5). Significant (and positive) associ-ations were also verified between LS and the presenceof chronicpain(p<0.001)andoccurrenceoffalls(p=0.02); fur-thermore,asignificantassociationwithself-perceivedhealth wasalsodetermined,butinthiscasewithanegative correla-tion(p<0.001),accordingtothechi-squaredtest.
Table2–Samplecharacterization.
n % p-value
Age(years) Mean(CI)82(1.5) Min–Max61–100
60–70 9 9 <0.01
71–80 28 28 <0.01
81–90 53 53
>90 10 10 <0.01
Gender
Male 27 27 <0.01
Female 73 73
Ethnicgroup
White 50 50
Brown 39 39 0.118
Black 11 11 <0.01
Maritalstatus
Married 35 35 0.015
Single 8 8 <0.01
Widow(er) 52 52
Separated/divorced 5 5 <0.01
Scholarship(years)
Illiterate 16 16 <0.01
1–4 57 57
5–8 11 11 <0.01
9–11 3 3 <0.01
≥12 13 13 <0.01
BADL
Mean(CI)5.5(0.1) Min-Max3–6
Independent 96 96 <0.01
Partialdependency 4 4
IADL
Mean(CI)23.6(0.8) Min–Max11–27
Independent 40 40 0.885
Mildlydependent 41 41
Moderatelydependent 13 13 <0.01
Severelydependent 6 6 <0.01
CI,confidenceinterval;Min–Max,minimum–maximum.
Table3–ReproducibilityofGLFS25-P,accordingto Student’st-testandICI.
GLFS-25P E1 E2 E1 E3
Student’st-test
Mean 27.6 27.3 27.6 28.1
Median 25 23.5 25 27
Standarddeviation 20.7 22.3 20.7 21.4
CI 4.1 4.4 4.1 4.2
p-value 0.66 0.304
ICI E1/E2 E1/E3
% 97.60 98.40
p-value <0.001 <0.001
CI,confidenceinterval.
Table4–ReproducibilityofGLFS25-P,accordingto Kappaindex.
GLFS E1/E2 E1/E3
Kappa p-value Kappa p-value
Question1 0.512 <0.001 0.597 <0.001
Question2 0.364 <0.001 0.417 <0.001
Question3 0.297 <0.001 0.46 <0.001
Question4 0.396 <0.001 0.472 <0.001
Question5 0.532 <0.001 0.456 <0.001
Question6 0.572 <0.001 0.508 <0.001
Question7 0.532 <0.001 0.591 <0.001
Question8 0.511 <0.001 0.55 <0.001
Question9 0.469 <0.001 0.488 <0.001
Question10 0.642 <0.001 0.546 <0.001
Question11 0.469 <0.001 0.531 <0.001
Question12 0.529 <0.001 0.611 <0.001
Question13 0.497 <0.001 0.611 <0.001
Question14 0.55 <0.001 0.522 <0.001
Question15 0.593 <0.001 0.56 <0.001
Question16 0.248 <0.001 0.206 0.001
Question17 0.533 <0.001 0.652 <0.001
Question18 0.641 <0.001 0.555 <0.001
Question19 0.465 <0.001 0.531 <0.001
Question20 0.465 <0.001 0.561 <0.001
Question21 0.575 <0.001 0.551 <0.001
Question22 0.429 <0.001 0.673 <0.001
Question23 0.399 <0.001 0.484 <0.001
Question24 0.438 <0.001 0.402 <0.001
Question25 0.501 <0.001 0.416 <0.001
theunivariatemodel;itwasnotedasignificantlyhigherriskof LSinthepresenceofchronicpain(OR15.92,95%CI3.08–82.27) andalsointhepresenceofaworseself-perceptionofhealth (OR0.23,95%CI0.07–0.79)(Table6).
Discussion
GLFS-25wascreatedinJapanin2011and,untilthen,hadnot yetbeentranslated,culturallyadaptedorvalidatedinother populations,despitetheimportanceofthetopicdiscussed.
Inthisstudy,theBrazilianversionofGLFS-25(GLFS25-P) used known and frequently used terms in ourmidst, and thuswaseasilyunderstoodbyolderpeoplefromdifferentage groupsandlevelsofeducation.
Theinstrumentinquestionallowsanimportant multidi-mensionalanalysisoftheagingindividual,bybeingcomposed
Table5–CorrelationsbetweenGLFS25-Pandfunctional status,accordingtoPearson’scoefficient.
BADL IADL
E1
Corr.(r) −50.30% −62.30%
p-value <0.001 <0.001
E2
Corr.(r) −45.90% −61.30%
p-value <0.001 <0.001
E3
Corr.(r) −49.50% −63.90%
Table6–Logisticregressionofstudiedvariables.
Variable Coefficient p-value OddsRatio
Constant 0.0468
Chronicpain 2.7673 0.001 15.92
Fall 0.5437 0.526 1.72
Self-perceptionofhealth −1.4506 0.019 0.23
ofquestions relatedtohealthandmobilityand groupedin areas, namely: daily care (5 questions), difficulties related to the motion (3 questions), pain (4 questions), cognition (2 questions), and items associated with social activities (4questions).Thisinstrumentpresentsalsoasixthdomain (7items),withquestionsrelatedtofunctionalityindailylife, whichhas provedto bestronglyassociatedwiththe other areas.Thus, this isconsidered a key domain,or a critical dimension,oftheinstrument.3
Oursampleiscomposedprimarilyofwomen(80.4%),in linewith datafrom the scientificliteraturethat pointto a feminizationoftheagingprocess.11Furthermore,thisseries countedon“veryold”elderlysubjects(63%oftheparticipants wereaged80yearsorolder).Therefore,oursampleduly rep-resentedthatpartofthepopulationwiththefastestgrowth rateintheworld:thelong-livedindividuals.12,13
ByanalyzingthepsychometricpropertiesofGLFS25-P,and initiallyconsideringitsinternalconsistency,wecouldobserve ahighvalueforCronbach’salphainallinterviews(above0.9), similartothevalueobtainedinthevalidationoftheoriginal studyinstrument(0.961).3
AstothereproducibilityofGLFS25-P,theinstrumentwas considered outstanding,taking into accountthe intra-and inter-observercorrelationsandthefactthatnosignificant dif-ferenceswereobservedintheanalyses.Inaddition,foreach questionoftheinstrument,theagreementsobtainedfromthe interviewerswereconsiderable,accordingtoKappastatistics. Thus,theoverallreliabilityofwassatisfactory,inviewofall reproducibilityanalysesoftheinstrument.
Byanalyzingeachquestion oftheinstrument,wenoted that somequestions are similar,due to the fact that they addressa specifictopic,suchassocialinteraction in ques-tions16,22and23,showingacertainredundancy.However, otherissues,suchasself-perceivedhealthandriskoffalling, whichwereassociatedwithLSinthisstudy,werenotdirectly addressed.Intheinstrumentvalidationprocessunder discus-sion,GLFS25-Pwascorrelatedwithfunctionalityindices,both forbasicactivitiesandforinstrumentalactivitiesofdaily liv-ing,whichiscommoninstudieswithelderlypopulations.To date,thereisnoavailabilityofagoldstandardforthe diag-nosisofLS;however,significantassociationswereobserved betweenthissyndromeandlossoffunctionintheelderly.2
Asdemonstratedinapreviousstudy,anassociationwith theoccurrenceoffallswasobserved,whichemphasizesthe needforanLSscreeningprocedure,inordertoprevent osteo-poroticfractures.14Similarly,chronicpainofmusculoskeletal etiology,asthataffectingtheknee,spine,orshoulders,has alsobeen associated withLS, whichwould strengthen the needforanearlytreatmentinthepreventionofthissyndrome intheelderly.15Asfortheself-perceptionofhealth,ourswas thefirststudytoanalyzethecorrelationofthistopicwithLS. ThesignificantassociationofLSwithaworseself-perceived
health,asverifiedinthepresentstudy,showsapossible neg-ativeimpactofLSintheindividual’squalityoflife.
TheprevalenceofLSamongelderlysubjectsinthisstudy was 63%, representing a high proportion of elderly atrisk of locomotive dysfunction. Screening programs for LS in theelderlycouldassistinimplementingearlyinterventions aimedatpreventingthesedisorders.Tothatend,the availabil-ityofaneasy-to-understand,easy-to-applyinstrumentwould helpthoseprofessionalsinservicesofgreatdemand.
Withreferencetothelimitationsofthisstudy,we men-tionthefactthatwedidnotperformphysicalteststhatcould alsoassesstheriskofLS,forinstance,the“Stand-uptest”and the“Two-steptest”,ashasbeensuggestedbysomeauthors.16 However,onlyveryrecentlythesesametestswereappointed asnewindicesintheassessmentofriskforLS;thatis,they wereidentifiedasindicesofriskanddecliningmobility,inthe samewayasGFLS-25.14,17
GLFS25-Pwas consideredasimpleandquickly applica-bletool,requiringashorttimeperiod(about5–10min)forits application.Inthisstudy,wedidnotmaketheself-application oftheinstrument,asthedifferentlevelsofeducationofthe elderlyinourmidstwouldbeanimportantsecondarybias. However,thiscouldbeaveryinterestingwayofapplication, forexample,inphysician’s“waitingrooms”andinofficesof otherhealthprofessionals,whichwouldfacilitatethe assess-ment ofriskforlocomotivedisordersintheelderly. Inthis latter sense, thesecasestudies would beof greatvaluein ourenvironment,especiallyiflongitudinallyconducted,since theycouldassistinestablishingcausalrelationshipsforLS. Andinthesecases,thestudiesalsowouldhelptoassessthe impactofpreventiveapproaches,suchasmonitoredphysical activityprograms,inthepreventionoflocomotivedisorders, andintheinstitutionalizationoftheelderly.
Inconclusion,GLFS25-Pconstitutesatoolwithappropriate translationandculturaladaptation,andthroughtheanalysis ofitspsychometricproperties,itwasfoundthatthis instru-menthasprovenreliableandvalidforthescreeningofLSin elderlyindividualslivinginourmidst.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgements
WewouldliketothankFabioFreireJose,MD,FabioTeruo Mat-sunaga,MD,ThaisaSeguradaMotta,MD,andPauloMateus Costa Affonso and MariaAngela Mello Barreto Guimarães, whocomposedthepanelofexpertsinthecross-cultural adap-tationprocess.
r
e
f
e
r
e
n
c
e
s
http://biblioteca.ibge.gov.br/visualizacao/livros/liv93322.pdf
[accessed17.10.15].
2. NakamuraKA.“Super-agedsociety”andthe“locomotive syndrome”.JOrthopSci.2008;13:1–2.
3. SeichiA,HoshinoY,DoiT,AkaiM,TobimatsuY,IwayaT. Developmentofascreeningtoolforriskoflocomotive syndromeintheelderly:the25-questionGeriatric LocomotiveFunctionScale.JOrthopSci.2012;17:163–72.
4. ComprehensiveSurveyofLivingConditions[Internet].Tokyo: MinistryofHealth,LabourandWelfare;2011.Availablefrom:
http://www.mhlw.go.jp/english/database/db-hss/cslc-index. html[accessed17.10.15].
5. NakamuraK.Theconceptandtreatmentoflocomotive syndrome:itsacceptanceandspreadinJapan.JOrthopSci. 2011;16:489–91.
6. HiranoK,ImagamaS,HasegawaY,ItoZ,MuramotoA, IshiguroN.Theinfluenceoflocomotivesyndromeon health-relatedqualityoflifeinacommunity-living population.ModRheumatol.2013;23:939–44.
7. OkuboT,SueharaY,KawasakiT,AkaikeK,TodaM,OkuboN, etal.Anoutpatient-basedsurveyabouttherecognitionof locomotivesyndromeandtheresultsoftheloco-checkata universityhospitalinTokyo.BrJMedMedRes.2014;4:3255–68.
8. LocomotiveSyndromePamphlet[Internet].Tokyo: LocomotiveChallenge!Council,JapaneseOrthopaedic Association;2013.p.1–8.Availablefrom:
https://locomo-joa.jp/en/index.pdf[accessed17.10.15]. 9. GuilleminF,BombardierC,BeatonD.Cross-cultural
adaptationofhealth-relatedqualityoflifemeasures: literaturereviewandproposedguidelines.JClinEpidemiol. 1993;46:1417–32.
10.GambaroRC,SantosFC,ThéKB,CastroLA,CendorogloMS. Avaliac¸ãodedornoidoso:propostadeadaptac¸ãodoGeriatric PainMeasureparaalínguaportuguesa.RevBrasMed. 2009;66:62–5.
11.Projec¸ãodaPopulac¸ãodoBrasilporsexoeidade:2000–2060 [Internet].RiodeJaneiro:InstitutoBrasileirodeGeografiae Estatística(IBGE);August2013.Availablefrom:http:// www.ibge.gov.br/home/estatistica/populacao/projecaoda populacao/2013/default.shtm[accessed17.10.15].
12.KirkwoodTBL.Asystematiclookatanoldproblem.Nature. 2008;451:644–7.
13.MottaTS,GambaroRC,SantosFC.Painmeasurementinthe elderly:evaluationofpsychometricpropertiesoftheGeriatric PainMeasure-Portugueseversion.RevDorSãoPaulo. 2015;16:136–41.
14.IshibashiH.On2015GuidelinesforPreventionandTreatment ofOsteoporosis.Osteoporosisinrelationtolocomotive syndrome.ClinCalcium.2015;25:1313–8.
15.IizukaY,IizukaH,MiedaT,TajikaT,YamamotoA,Takagishi K.Population-basedstudyoftheassociationofosteoporosis andchronicmusculoskeletalpainandlocomotivesyndrome: theKatashinastudy.JOrthopSci.2015;20:1085–9.
16.OgataT,MuranagaS,IshibashiH,OheT,IzumidaR, YoshimuraN,etal.Developmentofascreeningprogramto assessmotorfunctionintheadultpopulation:a
cross-sectionalobservationalstudy.JOrthopSci. 2015;20:888–95.