SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Case
Report
Monosegmental
combined
anterior
posterior
instrumentation
for
the
treatment
of
a
severe
lumbar
tuberculous
spondylodiscitis:
case
report
and
literature
review
夽
Petracchi
Matias,
Camino
Willhuber
Gaston
∗,
Tripodi
Maria,
Bassani
Julio,
Gruenberg
Marcelo,
Sola
Carlos
ItalianHospitalofBuenosAires,InstituteofOrthopedics“CarlosE.Ottolenghi”,BuenosAires,Argentina
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received4July2016
Accepted30August2016
Availableonline29December2016
Keywords:
Discitis
Lumbarvertebrae
Tuberculosis,spinal
Thoracicvertebrae
Spinalfusion
Debridement
a
b
s
t
r
a
c
t
Spinaltuberculosis(Pottdisease)canproduceseveredeformitieswhenitisnotproperly
treated. Longinstrumentationsthroughsingleorcombineddoubleapproachesare
usu-allyrequiredtopreventandcorrectthedeformity.Theauthorspresentacaseofsevere
deformity secondarytotuberculousspondylodiscitisinthelumbarspinetreatedwitha
monosegmentalinstrumentationthroughadoubleapproachinapatientwithidiopathic
scoliosis.Deformitycorrectionandinfectionresolutionthroughdebridementand
arthrode-sisisobservedafteroneyearoffollow-up.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora
Ltda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http://
creativecommons.org/licenses/by-nc-nd/4.0/).
Instrumentac¸ão
monossegmentar
anterior
e
posterior
combinada
para
o
tratamento
de
uma
espondilodiscite
tuberculosa
severa:
relato
de
caso
e
revisão
da
literatura
Palavras-chave:
Discite
Vértebraslombares
Tuberculosedacolunavertebral
Vértebrastorácicas
r
e
s
u
m
o
A tuberculoseespinhal(doenc¸adePott)podeproduzirdeformidadesseverassenãofor
tratadaadequadamente.Instrumentac¸õeslongasatravésdeumaabordagemsimplesou
duplageralmentesãonecessáriasparacorrigiradeformidade.Osautoresapresentamum
casodedeformidadeseveraemregiãolombarsecundáriaaespondilodiscitetuberculosa
tratadacominstrumentac¸ãomonossegmentáriaporduplaabordagememumpacientecom
夽
StudyconductedattheItalianHospitalofBuenosAires,InstituteofOrthopedics“CarlosE.Ottolenghi”,BuenosAires,Argentina.
∗ Correspondingauthor.
E-mail:[email protected](C.W.Gaston).
http://dx.doi.org/10.1016/j.rboe.2016.12.010
2255-4971/©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditoraLtda.Thisisanopenaccessarticle
736
rev bras ortop.2017;52(6):735–739Fusãovertebral
Debridamento
diagnósticoinicialdeescolioseidiopática.Acirurgiacorretivaearesoluc¸ãodainfecc¸ão
atravésdedebridamentoeartrodeseéobservadaapósumanodeacompanhamento.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier
EditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http://
creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Tuberculosis(TBC)diseaseisanunsolvedproblemin
develop-ingcountries,morethan80%representapulmonarydisease,
tuberculous spondylitis (Pott disease) represent a site for
extra-pulmonarytuberculosis, it occurs in less than 1% of
patientswithtuberculosis.1
Tuberculous spondylitistypicalpresentationcaninvolve
anteriorelements,usuallytwoadjacentvertebralbodiesand
theintervertebraldisc,andformsaparavetebralabscess.It
rarelyinvolvestheposteriorelements(neuralarch
tuberculo-sis)inisolationorcombinationwithlamina,spinoutsprocess,
transverseprocess,articularprocessandpedicles,itcanalso
makeanepiduralabscessand/orpyomyositisoftheposterior
spinalmuscles.
Thetypicalclinicalpresentationisbackpain,butinthose
whenitinvolvesposteriorelementsalsomayleadtothe
sud-denonsetofaneurologicaldeficit.2
The treatment of tuberculosis spondylitis is based on
the structuraldamage secondary tobone and ligamentary
destruction.Ingeneral;debridement andanterioror
poste-riorfusionproceduresarerequired.Approximately5%ofthe
Tuberculosis inthespine developsseveredeformities3 and
surgicaltreatmentrepresentsachallengeinthisscenario.
Short-instrumentation has been described previously
for one level Tuberculosum spondylodiscitis and mild
deformities,4 however, to our knowledge, monosegmental
instrumentationforthetreatmentofaseveredeformity
lum-barTBChasnotbeendescribedpreviously.
We present the treatment of lumbar TBC treated by
debridementandone-levelanteriorposteriorarthrodesisof
thelumbarspineinapatientwithmildscoliosis.
Case
report
A23-yearsoldfemalewaspreviouslytreatedinother
insti-tutionbecauseofpsoas tearduringthreemonths,because
ofprogressiveseverelumbarpainsheconsultedtoour
insti-tution.Therewasnoneurologicalcompromise.Weightlost
wasnotdetectedandanyothersymptomwasassociatedto
thelumbarpain.Previousspinalradiographyanalysisshowed
rightthoracicidiopathicscoliosiswitha22degreeslumbar
compensatorycurve(Fig.1).
MRIwasthenperformedshowingL2vertebralbody,L2–L3
discandrightpsoascompromise(Fig.2).Spondylodiscitiswas
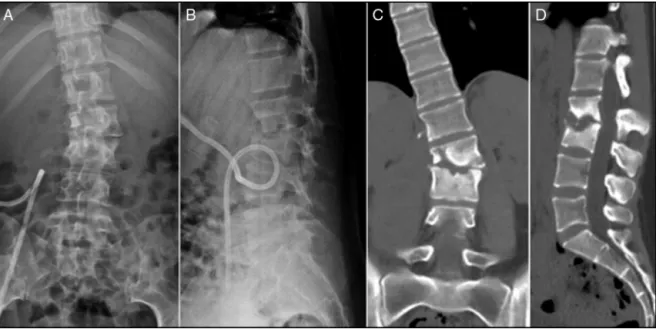
then suspected. CT-scanwas performed in order to
evalu-atealabdominalstructuresandtoruled-outanotherclinical
problems related to this severe pain (Fig. 3). Severe L2–L3
compromisewasobservedonCTscanwithincreasedcurve
deformityatthislevel.
Fig.1–(A)Posteriorview,thoracolumbarscoliosiswith22 gradesatthelumbarregion;(B)Lateralradiologicalview approximatelyoneyearbeforediagnosis.
Percutaneous CT scanguided catheterintervention was
performed with 60cm3 hematogenous material drainage
(Fig.3)butthecultureswerenegative.
Surgerywasplannedtostabilizeandcorrectspinal
defor-mity,drainageofnecroticandinflammatorycomponentand
preventneurologicalcompromise.
Surgicaltreatment
Vertebralsegmentarykyphosisandlateralangulationwere17
and25degreesrespectively.
Monosegmentary instrumentation through a double
antero-posterior approachwas planned.Firststage,a
min-imally invasivelateral right sideapproachforintersomatic
and para-vertebraldebridementwasperformedfollowedby
areconstructionwithL2-L3interbodytitaniumcagewithrib
boneautograft.
Posteriorly,withthesameanesthesia,aposteriorapproach
forL2–L3pedicularinstrumentationwas performedandno
normalspinallevelswereinstrumented(Fig.4).
Estimated blood loss during the entire procedure was
Fig.2–(A)and(B)T1–T2sagittalMRIshowingL2–L3compromise;(C)and(D)AxialMRIshowingrightpsoasmuscle compromise.
monitoring including somatosensory evoked potentials
(SSEPs)andmotorevokedpotentials(MEPs).
Nocomplicationswereobservedduringtheprocedure.
Histologicalanalysis
Microscopicimages(Fig.5)showedgranulomatosusreaction
withmultinucleatedcells.ZiehlNeelsencolorationtechnique
wasnegative,however,polymerasechainreaction(PCR)was
positivefortuberculosis.
Postoperativetreatmentandfollowup
A Thoraco-lumbo-sacralorthosis (TLSO)was indicated and
usedduringthreemonths.
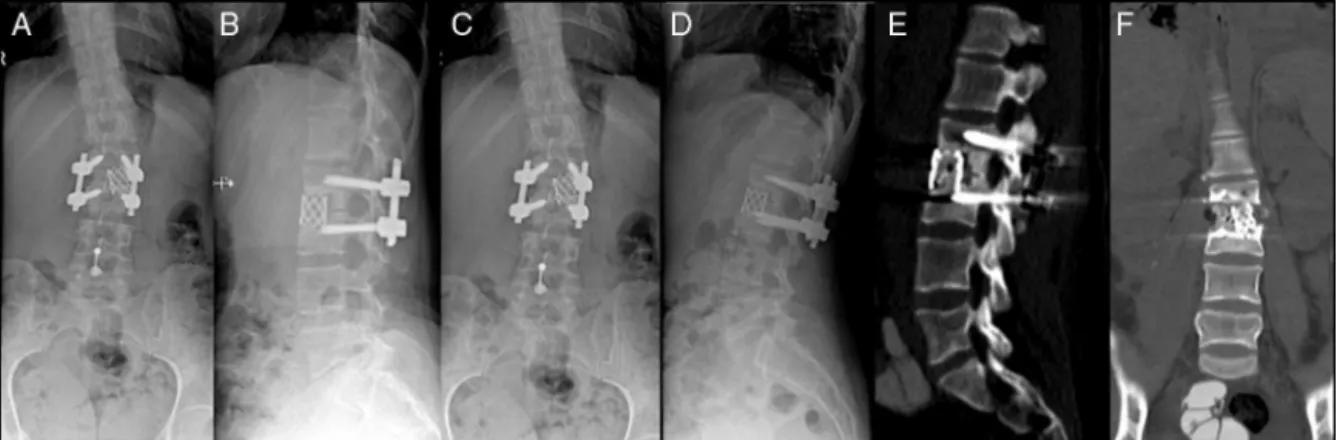
Clinicalandradiologicalcontrolwasperformedeverythree
months,nodeformitiesduringfollowupwereobserved,
post-operativeanteriorandlateralsegmentalangleswere1and2
degreesrespectively.Clinicalparameterswereimprovedand
antituberculosistherapy wassuccessfulafter12monthsof
treatment(Fig.6).
738
rev bras ortop.2017;52(6):735–739Fig.4–Intraoperativeradioscopicstepsfortheanteriorandposteriorarthrodesis,lateralminiinvasiveapproach,vertebral andpsoasdebridementfollowedbyinterbodycageinstrumentationandpostoperativeposteriorinstrumentation.
Postoperative protocol included four anti tuberculosis
agentsfortwomonths(Isoniazide,Ethambutol,Pirazinamide,
Rifampin)followedbytwodrugsforten months(Isonizide,
Rifampin).
Discussion
Thetreatmentofspinaltuberculosisusuallyisnon-surgical,
by the administration of four anti-tuberculosis drugs and
bracing.5Therearesomesituationsinwhichsurgical
treat-mentisrequired:lossofsagittalorcoronalalignmentofthe
spineduetoextensiveosteolysisandspread ofanabscess
intothepara-spinaltissuesandspinalcanal,withprogressive
neurologicdeficit,failedconservativetreatmentoruncertain
diagnosis.2
Posteriorinstrumentationwithorwithoutanteriorfusion
hasdemonstratedgoodclinicalandsurgicalresults.6,7
Anterior fusion alone, is generally indicated for
patients with single level compromise and minor or mild
deformities,8–10 additional posterior instrumentation is
considered in multilevel compromise or severe deformity,
however, short or long instrumentations are performed in
ordertopreventearlyfailureandobtainmorecorrection.11
Theanteriorapproachispossibleonlyiftheposterior
col-umnisintact,anditisdemonstratedthatcandecreasethe
operatingtime,bloodloss,andpostoperativemorbidity.
How-everforapatientwithpanvertebraldisease,orwiththeneed
Fig.6–(A)and(B)Immediatepostoperativecontrol;(C)and(D)Oneyearpostoperativecontrol;(E)and(F)CT-scanshowing L2–L3interbodyarthrodesis.
forposteriorcolumnshorteningtoreducekyphosis,or
multi-leveldisease,posteriorstabilizationisnecessary.12
Wepresentacaseofseverelumbardeformitysecondary
tospondylitistuberculosistreatedthroughadoubleanterior
posterior approach with monosegmental instrumentation,
arthrodesis was observed after a follow-up of one year.
Thistechnique should beattempt aftera carefullypatient
selection.Morecasesarerequiredtoreinforcethis
recommen-dation.
Toourknowledgecombinedmonosegmental
instrumenta-tionforthetreatmentofaseverespinaldeformitysecondary
toTuberculosumspondylitishavenotbeendescribed.More
casesareneededtosupportthistreatment.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. AroraS,SabatD,MainiL,SuralS,KumarV,GautamVK,etal. Isolatedinvolvementoftheposteriorelementsinspinal tuberculosis:areviewoftwenty-fourcases.JBoneJointSurg Am.2012;94(20):e151.
2. KapoorSK,GargV,DhaonBK,JindalM.Tuberculosisofthe posteriorvertebralelements:ararecauseofcompressionof thecaudaequina.Acasereport.JBoneJointSurgAm. 2005;87(2):391–4.
3. IssackPS,Boachie-AdjeiO.Surgicalcorrectionofkyphotic deformityinspinaltuberculosis.IntOrthop.2012;36(2):353–7.
4.KlöcknerC,ValenciaR.Sagittalalignmentafteranterior debridementandfusionwithorwithoutadditionalposterior instrumentationinthetreatmentofpyogenicand
tuberculousspondylodiscitis.Spine(PhilaPa1976). 2003;28(10):1036–42.
5.MoonMS,KimI,WooYK,ParkYO.Conservativetreatmentof tuberculosisofthethoracicandlumbarspineinadultsand children.IntOrthop.1987;11(4):315–22.
6.MakKC,CheungKM.SurgicaltreatmentofacuteTB spondylitis:indicationsandoutcomes.EurSpineJ.2013;22 Suppl.4:603–11.
7.YangP,HeX,LiH,ZangQ,YangB.Clinicalefficacyof posteriorversusanteriorinstrumentationforthetreatment ofspinaltuberculosisinadults:ameta-analysis.JOrthop SurgRes.2014;9(1):10.
8.DaiLY,JiangLS,WangW,CuiYM.Single-stageanterior autogenousbonegraftingandinstrumentationinthesurgical managementofspinaltuberculosis.Spine(PhilaPa1976). 2005;30(20):2342–9.
9.GueradoE,CervánAM.Surgicaltreatmentof spondylodiscitis.Anupdate.IntOrthop.2012;36(2): 413–20.
10.TosunB,ErdemirC,YongaO,SelekO.Surgicaltreatmentof thoracolumbartuberculosis:aretrospectiveanalysisof autogenousgraftingversusexpandablecages.EurSpineJ. 2014;23(11):2299–306.
11.HuJ,LiD,KangY,PangX,WuT,DuanC,etal.Activethoracic andlumbarspinaltuberculosisinchildrenwithkyphotic deformitytreatedbyone-stageposteriorinstrumentation combinedanteriordebridement:preliminarystudy.EurJ OrthopSurgTraumatol.2014;24Suppl.1:S221–9.