SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Original
article
In
vivo
evaluation
of
porous
hydrogel
pins
to
fill
osteochondral
defects
in
rabbits
夽
Túlio
Pereira
Cardoso
a,∗,
André
Petry
Sandoval
Ursolino
a,
Pamela
de
Melo
Casagrande
a,
Edie
Benedito
Caetano
a,
Daniel
Vinicius
Mistura
b,
Eliana
Aparecida
de
Rezende
Duek
a aPontifíciaUniversidadeCatólicadeSãoPaulo,FaculdadedeCiênciasMédicasedaSaúdedeSorocaba,Sorocaba,SP,BrazilbUniversidadeFederaldeSãoCarlos,Sorocaba,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received14January2016
Accepted29March2016
Availableonline29December2016
Keywords:
Articularcargilage
Hydrogels/chemistry Rabbits
a
b
s
t
r
a
c
t
Objective:Thisexperimentalstudyaimedtoevaluatethebiologicalperformanceofpoly
(l-co-D,l-lacticacid)-co-trimetilenecarbonate/poly(vinylalcohol)(PLDLA-co TMC/PVA),
hydrogelscaffolds,asanimplantinthefilling(andnotintherepair)ofosteochondraldefects
inNewZealandrabbits,assessingtheinfluenceofthematerialintissueprotectioninvivo.
Methods:Twelverabbitsweredividedintogroupsofnineand16weeks.Ineachanimal,an
osteochondraldefectwascreatedinbothmedialfemoralcondyles.Inoneknee,ahydrogel
scaffoldwasimplanted(pingroup)andintheother,thedefectwasmaintained(control
group).Ahistologicalanalysisofthematerialwasperformedaftereuthanasia.
Results:The condylesofthepingroupshowednoinflammatoryreactionandwere
sur-roundedbyafibrouscapsule.Thecontrolgrouppresentedhigherbonegrowthintheareasof
thedefect,butwithdisorganizedarticularcartilage,evidentfibrosis,boneexposure,atrophy,
andproliferationofsynovialmembrane.
Conclusion: Thehydrogelpinsarepromisinginfillingosteochondraldefects,generallydonot
causeinflammatoryreactions,andarenoteffectiveintherepairofosteochondraldefects.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora
Ltda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http://
creativecommons.org/licenses/by-nc-nd/4.0/).
夽
StudyconductedatthePontifíciaUniversidadeCatólicadeSãoPaulo,LaboratóriodeBiomateriais,FaculdadedeCiênciasMédicase
daSaúdedeSorocaba,Sorocaba,SP,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](T.P.Cardoso).
http://dx.doi.org/10.1016/j.rboe.2016.03.009
2255-4971/©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditoraLtda.Thisisanopenaccessarticle
Avaliac¸ão
do
desempenho
in
vivo
de
pinos
porosos
de
hidrogel
para
preenchimento
de
defeito
osteocondral
em
coelhos
Palavras-chave:
Cartilagemarticular
Hidrogéis/química Coelhos
r
e
s
u
m
o
Objetivo: Trabalhoexperimentalparaavaliarodesempenhobiológicodearcabouc¸osde
hidrogelpoli(l-co-D,lácidolático)-co-trimetilenocarbonato/poli(álcoolvinílico)
(PLDLA-co-TMC/PVA)comoimplantenopreenchimento,enãonoreparo,dedefeitoosteocondral
emcoelhosNovaZelândiaeverificarainfluênciadomaterialnaprotec¸ãotecidualinvivo.
Métodos: Foramusados12coelhosdivididosemgruposdenovee16semanas.Emcada
animalfoicriadoumdefeitoosteocondralemambososcôndilosfemoraismediais,emum
foiimplantadoumarcabouc¸odehidrogel(grupopino)enooutrofoimantidoodefeito
(grupocontrole).Apósosacrifíciodosanimais,foifeitaanálisehistológicadomaterial.
Resultados: Oscôndilosdogrupopinonãoevidenciaramreac¸ãoinflamatóriaeestavam
rodeadosporcápsulafibrosa.Jánogrupocontrole,umamaiorproliferac¸ãoósseafoi
obser-vadanasáreasdodefeito,porémcomcartilagemarticulardesorganizada,fibroseevidente,
atrofiacomexposic¸ãoósseaeproliferac¸ãodemembranasinovial.
Conclusão: Ospinosdehidrogelsãopromissoresnafunc¸ãodepreenchimentodedefeitos
osteocondrais,nãoocasionam,demodogeral,reac¸ãoinflamatóriaenãosãoeficazesno
reparodedefeitososteocondrais.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier
EditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http://
creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Osteoarthritis is one of the diseases that most commonly
affect humans.1 Its prevalence increases with age, being
common after 60 years.2 The articular cartilage and the
subchondralboneformalubrication,stabilization,and
uni-formloaddistributionsystem,absorbingshocksandallowing
movementwithlowfrictionforseveraldecades.2–4Thus,
car-tilageprotectssubchondralbonefromhighstressandreduces
normalcontactpressure.2,5Degradedcartilageevolvestojoint
pain,stiffness,anddecreasedmovement.Duetolow
chon-dralregenerationcapacity,osteoarthritisisoneofthemost
importantproblemsinorthopedics.Withincreasinghuman
longevityandthepracticeofsportsinrecentdecades,
osteo-chondralinjurieshavebeenincreasinglyobserved.2
Normal joint cartilage features a solid phaseconsisting
mostly ofcollagen and proteoglycans (15–32%) and a fluid
phasecomposedpredominantlyofwater(68–85%).2 Hyaline
cartilage consists of 10% cells (chondrocytes) and a dense
extracellularmatrix,composedof60–80%water,10–20%type
IIcollagenfibers,and10–15%proteoglycans.Themechanical
propertiesofthearticularcartilageallowittotransmitloads
ofapproximatelyeighttimesthebodyweight,dueto
exuda-tionandmovementofthefluidthroughtheporesofcartilage,
conferringafrictioncoefficientof0.008(mi).4,6
Thesubchondralboneisathinlayerofdense,hardbone
incontactwiththearticularcartilage,whiletrabecularbone
iscomposedofanabundantmatrix(collagenfibersand
min-erals)thatservestotransmitloads.6
Beingavascular,thecartilagedependsonthe
vasculariza-tionofthebonemarrowforthemigrationofmesenchymal
cells responsible for the healing process.7,8 Furthermore,
superficiallesionsofthearticularcartilagewithout
subchon-dralboneinvolvementhavelittleintrinsicrepaircapacity.9
Bothinprimaryandsecondaryosteoarthritis,cartilageis
thetissuethatundergoesthegreatestdamage.
Morphologi-calchangestothecartilageincludelossofitshomogeneous
nature,fragmentation,fibrillation,fissures,andulcerations.
Withdiseaseprogression,occasionallynocartilageremains
andareasofthesubchondralbonebecomeexposed.10
Three stages can be considered in the process of
tis-sue regeneration: necrosis, inflammation, and repair.11,12
Nonetheless,healingoflesionsrestrictedtothehyaline
car-tilage may not occur this way.13 Superficial lesions of the
articularcartilagethatdonotreachthesubchondralbonetend
nottoheal.9Intheselesions,thereisadegenerationofthe
car-tilagefromthesurfacearea;thinportionsofcollagenfibers
withscalyappearanceareobserved.Withlesionprogression,
verticalcrackswithanunevenanddullappearancecanbe
observedinthearticularcartilage.4,14
Chondrallesionstriggeraninflammatoryprocessandthe
hematoma quickly organizes itself into fibrin clots, white
bloodcells,andbonemarrowelements.
Undifferentiatedbonemarrowandvascularendothelium
cellsareconvertedintoprimitivefibroblasts,which,withinput
ofcapillariesandfibrinclots,turn intovascularfibroblastic
repair tissue.11 Depending on the mechanical and
biologi-calstimuli,thisfibrocartilagetissuewillformacartilaginous
tissue.13 Newlyformedbonemigrates fromthe baseofthe
defect to the articular surfacein the area in contactwith
subchondralbone.Fibrocartilaginoustissuefillsthetransition
Osteochondraldefect repairtissue has adifferent
com-position than normal cartilage.15 Chondrocytes synthesize
proteoglycansoflowermolecularweight.AscollagentypeII
fibershaveasmallerdiameter andmoreirregular
arrange-ment,thisconfigurationfavorswaterpermeability.Thisnewly
formedtissuepresentsalowerelasticmoduluswhen
com-paredwithnormalcartilagetissue.4,16,17
Surgicaltreatmentofchondralandosteochondrallesionsis
amajorchallenge.Theformationofcartilaginousor
fibrocarti-laginoustissuecanbestimulated,repairingorreplacingsuch
injurieswithatissuethatpresentssimilarcharacteristics.4,13
Therearenoreplacementtissueswhosemechanical
prop-ertiesare similartothat oftheoriginal tissue.18 Currently,
thereisongoing researchon tissueengineeringusing
syn-theticthree-dimensionalsystemswithporousscaffolds.19,20
Polymerssuchaspoly-p-dioxanone(PPD),polylacticacid
(PLA),polyglycolic acid (PGA)and its copolymers PLLAand
PLGA,andpoly-␣-hydroxyacids,aswellastheirdecay,
bio-reabsorption,andbiocompatibilitycharacteristics,havebeen
thoroughlystudied.4,21–24
A non-porous and non-absorbable hydrogel
(PLDLA-co-TMC/PVA) was used in the present study to fill the
osteochondraldefectratherthantomakearepairthatallowed
thegrowthofnewtissue.
The in vivo biological response to PLDLA-co-TMC/PVA
hydrogel pins in the filling of osteochondral defects is
unknown.
Thisstudyaimedtoevaluatethebiologicalperformance
ofPLDLA-co-TMC/PVAhydrogelscaffoldsasanimplantinthe
filling,ratherthanintherepairofosteochondraldefectsinNew
Zealandrabbits,andtoassesstheinfluenceofthematerialin
invivotissueprotection.
Material
and
methods
ThisstudywasapprovedbytheResearchEthicsCommitteeof
thisinstitution(CEUA/FCMS/PUCSP,Number2013/10).
Preparationofpolymerscaffolds(hydrogelpins)
Hydrogelpinsarecomposedofasemi-interpenetrating
poly-merbasedonpolyvinylalcohol(PVA)andpoly-l-co-d,l-lactic
acid-co-trimethylenecarbonate (PLDLA-TMC).Thehydrogel
wasmadewitha10%m/vPVAsolutioninwaterand10%ofthe
PLDLA-TMCcompoundrelativetothemassofthePVAused.
Thesolution was then pouredinto polytetrafluoroethylene
(PTFE)scaffoldswitha4.1mmdiameter,andwassubmitted
toafreeze–thawprocessfortwodays.Afterthisprocess,pins
wereremovedfromthescaffolds,cutatalengthof13mm,
sterilizedwithUVradiation,andimplanted(Fig.1).
Invivostudyoftheimplantedpinsandcontrols
TwelveNewZealand rabbitsofbothsexes wereused, aged
between120and150daysandweighingbetween3.5kgand
4.5kg.
Afterapreoperativeeight-hourfasting,theanimalswere
submittedtogeneralanesthesiawithintramuscularketamine
hydrochloride (30mg/kg) associated with xylazine chloride
Fig.1–PLDLA-co-TMC/PVAhydrogelpinsandscaffold
usedformakingthedevices.
(5mg/kg).Atrichotomyoftheoperatedareawasmade,and
rabbitswereplacedonaproperoperatingtableinthesupine
position.Sterilizationwasconductedwithalcoholic
chlorhex-idine0.5%,appliedwithsterilegauze.Surgeonusedsterile
surgicalglovesandthesurgicalmaterialsweresterilizedby
autoclavingat180◦Cfor2h.
Amedialparapatellarincisionwasused,withdissectionby
planes(subcutaneousandcapsulotomyforpatellarmedial).
Then,alateralpatellardislocationwasmadetoexposethe
femoralcondyles.Withthekneeflexedat90◦, acylindrical
defectwascreatedinthearticularcartilageandinthe
sub-chondralboneofthemedialfemoralcondylewiththeuseof
a3.3mm/38.5mmtrephinedrill;a1cmdeeposteochondral
cylinderwasremovedfrombothknees7,13(Figs.2and3).
Fig.3–Implantandosteochondralcylinder.
The chondral defect was created in both medial and
femoralcondyles;ononeside,thehydrogelpinwasimplanted
(implantside)whileontheother(controlside),thedefectwas
kept(Fig.4).
Suturesweremadeinplanesafterwashingwith0.9%saline
solution;nobandagesorimmobilizationdeviceswereused.
Allanimalswerekeptinindividualcageswithfoodandwater
adlibitum.
Removalofthematerial–euthanasiaandtissuecollection
Sevenanimals wereeuthanized afternineweeks,and five,
after16weeks.
Halothaneinhalationwasused.Afterdeathwasconfirmed,
theanimalwasplacedinthesupineposition.Then,themedial
femoral condylesofbothknees were resected through the
medialpatellaraccessroute.
Macroscopicevaluation
The condyles were individually identified, macroscopically
observed,andphotographed(Fig.5).Accordingtothe
modi-fiedOuterbridgeclassification,notissuegrowthwasobserved
onthepin(bothat9and16weeks),andthepingroupcould
notbeincludedintheclassification.Inthecontrolgroup,with
nineor16weeks,alterationscharacteristicofOuterbridgeII
wereobserved.
Materialprocessing–histologicalanalysis
Thefemoralcondyleswere placedinglass containerswith
Bouin’s solution (consisting ofpicric acid, acetic acid, and
formaldehyde)for24hforfixation, whichmaintainstissue
integrityafterdeath.
ThematerialwasdecalcifiedinEDTA4.13%(the
decalcifica-tionsolutionconsistedoftetrasodiumEDTA,sodiumtartrate,
potassium sodiumtartrate, hydrochloricacid, and distilled
water)for21days.
For histologicalprocessing, longitudinalparallel
(cranio-caudal)incisions weremadeandsequentiallyidentifiedfor
eachsample.Thistechniqueallowedapreciseevaluationof
theentireareaofthecondyle,includingtheinitiallyinjured
areaandtheentiresurfacearoundthelesion.
Samples,properlyidentified,weredehydratedinaseriesof
alcoholsolutions,sequentiallyclearedinxyleneI,II,andIII,
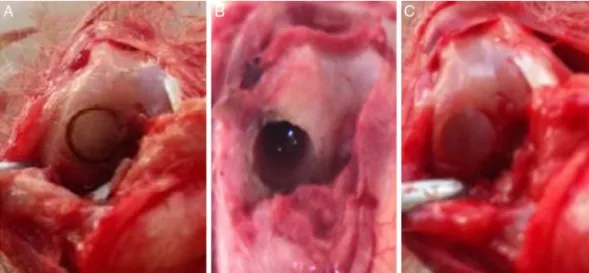
Fig.4–(A)Osteochondraldefectinsitu;(B)defectafterremovaloftheosteochondralcylinder;(C)defectfilledwiththe
Fig.5–(A)Withthehydrogelpin;(B)withoutthepin(controlgroup).
andembeddedinparaffinat70◦C.Aftercutting3mslices,
sampleswerestainedwithhematoxylin–eosinandanalyzed
byconventionallightmicroscopy.
Microscopicevaluation
Onhistologicexaminationofthesectionsofthedistalfemur,
attentionwasdirectedparticularlytothefollowingelements:
1. typeoftissuecoveringthearticularsurface:hyaline
carti-lage,fibrocartilage,bonetissue,orfibroustissue;
2. stateofthecartilaginoussurface:smooth,witha
depres-sion,orirregularwiththepresenceofcracksorfragments;
3. subchondralbonepattern;
4. presenceorabsenceofnecrosisandproperinflammatory
response;
5. presenceorabsenceofhyperplasticalterationsonthe
car-tilageorbone;
6. assessmentofsynovialmembranes,whenpossible.
Results
Theevaluationofresultsconsideredtheamountoffibrosis,
boneneoformation,andpresenceofcartilaginoustissueon
thecondylarsurface.
Inthepingroup,euthanizednineweeksaftertheimplant
was placed, mild fibrosis was found in four animals, and
marked fibrosis in two; no animal presented moderate
fibrosis.
Inthecontrolgroup,euthanizednineweeksafterthe
cre-ationoftheosteochondraldefect,mildfibrosiswasfoundin
twoanimals,moderateintwo,andsevereintwo.
In thepin group, euthanizedafter nineweeksafter the
implantwasplaced,oneanimalshowedboneneoformation;
infive, thisneoformationwas notobserved.In thecontrol
group,boneneoformationwaspresentinfouranimals,and
absentinone.
Regardingthepresenceofcartilageinthejointsurface,it
wasabsentinfourrabbitsinthecontrolgroupandpresent
inonecase.Inoneoftherabbits,anareathatcouldnotbe
defined as organized cartilaginous tissue was observed. In
the pingroup,presenceofcartilagetissuewasobservedin
four rabbits,whileintwo,itwasnotobserved(Table1and
Figs.6and7).
Oneofthe animalsincludedinthegroupeuthanizedat
16weekspresentedsurgicalsiteinfectionandwasexcluded
fromthestudy.
Fourrabbitsfromthepingrouphadmildfibrosisandone
hadnofibrosis.
Bone neoformation occurred infour rabbits in the
con-trol group; fragmentation of the material was observed
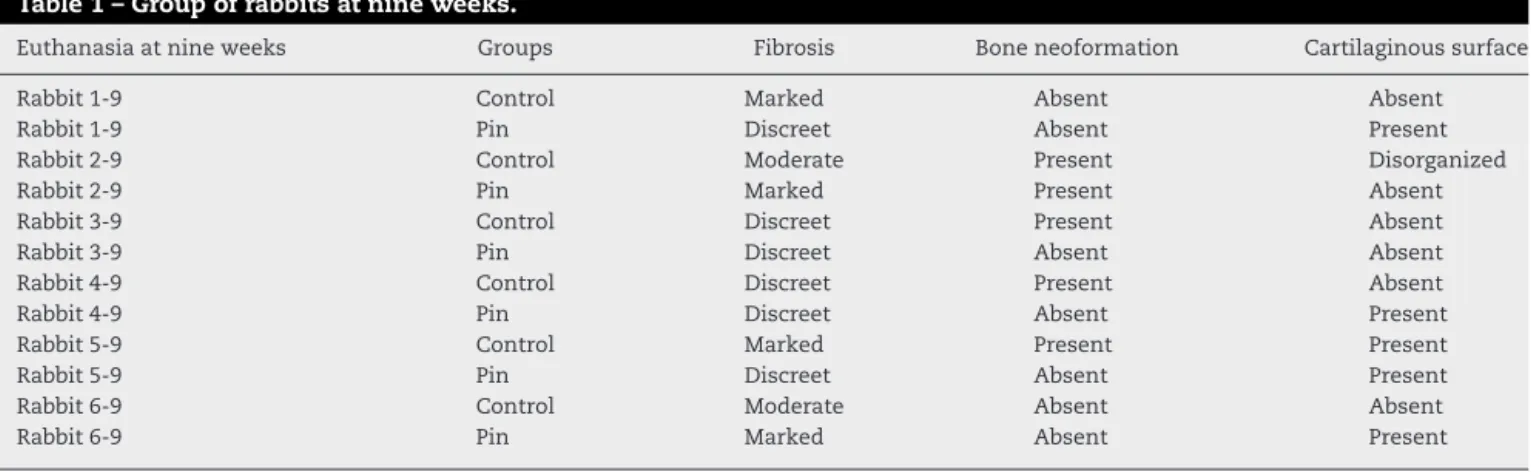
Table1–Groupofrabbitsatnineweeks.
Euthanasiaatnineweeks Groups Fibrosis Boneneoformation Cartilaginoussurface
Rabbit1-9 Control Marked Absent Absent
Rabbit1-9 Pin Discreet Absent Present
Rabbit2-9 Control Moderate Present Disorganized
Rabbit2-9 Pin Marked Present Absent
Rabbit3-9 Control Discreet Present Absent
Rabbit3-9 Pin Discreet Absent Absent
Rabbit4-9 Control Discreet Present Absent
Rabbit4-9 Pin Discreet Absent Present
Rabbit5-9 Control Marked Present Present
Rabbit5-9 Pin Discreet Absent Present
Rabbit6-9 Control Moderate Absent Absent
Fig.6–Histologicalslideofthepingroupatnineweeks
showingnoinflammatoryreactionandmildfibrosis.
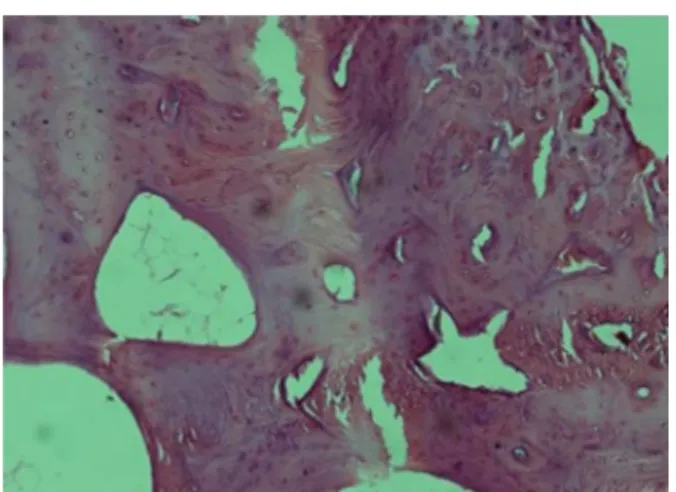
Fig.7–Histologicalslideofthecontrolgroupatnineweeks
showingboneneoformation,markedfibrosis,andtissue
disorganization.
in one rabbit, which prevented the correct analysis. Bone
neoformationwasnotobservedinthepingroup.
Inthecontrolgroupat16weeks,cartilagedegenerationwas
observedinonecase,whileinthecasewithfragmentationof
thematerial,itwasnotpossibletoanalyzethepresenceor
absenceofcartilage.Inthecontrolgroup,cartilageonthejoint
surfacewasobservedintworabbits,anditwasnotpresentin
Fig.8–Histologicalslideofthepingroupat16weeks
showingmildfibrosiswithoutboneformation.
onerabbit.Inthepingroup,fiverabbitspresentedcartilage,
vs.oneinwhichitwasabsent(Table2andFigs.8and9).
Discussion
Ofthe12rabbitsstudied,onlyonefromthegroupeuthanized
atnineweekswasexcludedduetolocalinfection.Thus,11
animalswereincludedinthisstudy.
ThehistologicalanalysisofthePLDLA-co-TMC/PVA
scaf-foldimplantsafternineweeksshowedthatthepindoesnot
induceaninflammatoryreaction,butalsodoesnotstimulate
boneneoformation.Thereisastimulusoffibrous
prolifera-tionattheedgesofthelesionfromthearticularcartilage,with
formationofmainlyfibrocartilage,asanattempttohealthe
injury.
Inthecontrolgroupafternineweeks,morefibrosis and
moreboneformationwereobserved,eitherfromarticular
car-tilagefromtheedgesofthelesionorfromthetrabeculaeof
compactbonesurroundedbyosteoprogenitorcells.However,
therewasnoevidenceofchondrallesionrepair.
Table2–Groupofrabbitsat16weeks.
Euthanasiaat16weeks Groups Fibrosis Boneneoformation Cartilaginoussurface
Rabbit1-16 Control Discreet Present Present
Rabbit1-16 Pin Discreet Absent Absent
Rabbit2-16 Control Discreet Present Present
Rabbit2-16 Pin Discreet Absent Present
Rabbit3-16 Control Discreet Present Degenerated
Rabbit3-16 Pin Discreet Absent Present
Rabbit4-16 Control Fragmented Infeasibleanalysis
Rabbit4-16 Pin Discreet Absent Present
Rabbit5-16 Control Moderate Present Absent
Fig.9–Histologicalslideofthecontrolgroupat16weeks
showingboneformationandfibrosis.
After 16 weeks, the condyles with hydrogel implants
showednoinflammatoryreactionandweresurroundedbya
fibrouscapsule.Thesurroundingtrabecularbonepresenteda
preservedaspectandclosureofthejointsurfacewasobserved,
withthepresenceofhyalinecartilageoratrophiccartilageof
fibro-hyalineappearance.
Inthe controlgroupat16 weeks,boneproliferationwas
observed in the defect areas. However, the articular
carti-lage was disorganized, with obvious fibrosis; atrophy with
exposed bone and proliferation ofthe synovialmembrane
wereobserved.
Regardingboneneoformation,totheauthors’surprise,one
animalfrom the nine-weekpin grouppresentedgrowth of
bonetissuewithfibrouspattern.Theotherrabbitsfromthis
groupshowednobonegrowth;inturn,boneformationwas
observedintheentirecontrolgroup.
As expected, bone filling in osteochondral defect was
observedinthecontrolgroupeuthanizedat16weeks,most
likelyduetotheincreasedtimebetweensurgeryand
euthana-sia.Conversely,noanimalsinthepingrouppresentedbone
growth in the defect. This suggests that the presence of
the implanted pin filled the entire space created by the
defect.
Conclusion
Hydrogelpinsweresuperiorregardingtheprotectionofthe
cartilaginous joint surface asdevices for filling
osteochon-draldefects.Nonetheless,theyshowednoreparativeeffect.
Incontrast,cartilagedegradationinboththedefectandthe
surroundingareawereobservedinthecontrolgroup.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.RedmanSN,OldfieldSF,ArcherCW.Currentstrategiesfor
articularcartilagerepair.EurCellMater.2005;9:23–32.
2.SwieszkowskiW,TuanBH,KurzydlowskiKJ,HutmacherDW.
Repairandregenerationofosteochondraldefectsinthe
articularjoints.BiomolEng.2007;24(5):489–95.
3.BuckwalterJA,EinhornTA,SimonSR,editors.Orthopaedic
basicscience.Biologyandbiomechanicsofthe
musculoskeletalsystem.2nded.Rosemont,IL:AAOS;2000.
4.GarridoLF.Avaliac¸ãododesempenhodeimplantesde
polietilenoedefosfatotricalcio,recobertosporhidrogel,em
defeitososteocondraisnojoelhodecães.Campinas:
UniversidadeEstadualdeCampinas,FaculdadedeCiências
Médicas;2007.Dissertac¸ão.
5.LittleK.Natureofosteopetrosis.BrMedJ.1969;2(5648):49–50.
6.DingM,DalstraM,LindeF,HvidI.Mechanicalpropertiesof
thenormalhumantibialcartilage–bonecomplexinrelation
toage.ClinBiomech(BristolAvon).1998;13(4–5):351–8.
7.SouzaTD,DelCarloRJ,ViloriaMIV.Efeitosdaeletroterapiano
processodareparac¸ãodasuperfíciearticulardecoelhos.
CiêncRural.2001;31:819–24.
8.LammiPE,LammiMJ,TammiRH,HelminenHJ,EspanhaMM.
Stronghyaluronanexpressioninthefull-thicknessrat
articularcartilagerepairtissue.HistochemCellBiol.
2001;115(4):301–8.
9.SlatterD.Manualdecirurgiadepequenosanimais.Baureri,
SP:Manole;1998.
10.RezendeUM,HernandezAJ,CamanhoGL,AmatuzziMM.
Cartilagemarticulareosteoartrose.ActaOrtopBras.
2000;8(2):100–4.
11.MankinHJ.Theresponseofarticularcartilagetomechanical
injury.JBoneJointSurgAm.1982;64(3):460–6.
12.CookSD,PatronLP,SalkeldSL,RuegerDC.Repairofarticular
cartilagedefectswithosteogenicprotein-1(BMP-7)indogs.J
BoneJointSurgAm.2003;85Suppl.3:116–23.
13.RibeiroJL,CamanhoGL,TakitaLC.Estudomacroscópicoe
histológicodereparososteocondraisbiologicamente
aceitáveis.ActaOrtopBras.2004;12(1):16–21.
14.EspósitoAR,BonadioAC,PereiraNO,CardosoTP,BarboMLP,
DuekEAR.TheuseofPLDLA/PCL-Tscaffoldtorepair
osteochondraldefectsinvivo.MatRes.2013;16(1):105–15.
15.HuntleyJS,McBirnieJM,SimpsonAH,HallAC.Cutting-edge
designtoimprovecellviabilityinosteochondralgrafts.
OsteoarthritisCartilage.2005;13(8):665–71.
16.HendersonI,FranciscoR,OakesB,CameronJ.Autologous
chondrocyteimplantationfortreatmentoffocalchondral
defectsoftheknee–aclinical,arthroscopic,MRInand
histologicevaluationat2years.Knee.2005;12(3):209–16.
17.HattoriK,TakakuraY,OhgushiH,HabataT,UematsuK,
IkeuchiK.Novelultrasonicevaluationoftissue-engineered
cartilageforlargeosteochondraldefects–non-invasive
judgmentoftissue-engineeredcartilage.JOrthopRes.
2005;23(5):1179–83.
18.BumaP,RamrattanNN,vanTienenTG,VethRP.Tissue
engineeringofthemeniscus.Biomaterials.
2004;25(9):1523–32.
19.MartinI,MiotS,BarberoA,JakobM,WendtD.Osteochondral
tissueengineering.JBiomech.2007;40(4):750–65.
20.JansenEJ,PieperJ,GijbelsMJ,GuldemondNA,RiesleJ,Van
RhijnLW,etal.PEOT/PBTbasedscaffoldswithlow
mechanicalpropertiesimprovecartilagerepairtissue
formationinosteochondraldefects.JBiomedMaterResA.
2009;89(2):444–52.
21.DuekEA,ZavagliaCA,BelangeroWD.Invitrostudyof
22.RahmanMS,TsuchiyaT.Enhancementofchondrogenic
differentiationofhumanarticularchondrocytesby
biodegradablepolymers.TissueEng.2001;7(6):781–90.
23.ZhaoK,DengY,ChunChenJ,ChenGQ.Polyhydroxyalkanoate
(PHA)scaffoldswithgoodmechanicalpropertiesand
biocompatibility.Biomaterials.2003;24(6):1041–5.
24.SakataMM,Alberto-RinconMC,DuekEA.Estudodainterac¸ão
polímero/cartilagem/ossoutilizandopoli(ácido
lático-co-ácidoglicólico)epoli(p-dionaxona)em