jcoloproctol(rioj).2017;37(4):332–335
w w w . j c o l . o r g . b r
Journal
of
Coloproctology
Technical
Note
Sphincter-saving
extrasphincteric
rectal
dissection
and
proximal
segmental
sphincteric
excision
techniques
by
using
combined
abdominal
and
transvaginal
anterior
perineal
access
in
female
patients
who
have
lower
rectal
cancer
(
Transvaginal
low
anterior
rectal
resection
)
Ali
Naki
Yücesoy
BatıBahatHospital,GeneralSurgeryDepartment,Istanbul,Turkey
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received29March2017 Accepted17May2017 Availableonline15July2017
Keywords:
Lowerrectalcancer Sphincter-savingsurgery
Combinedabdominalandperineal approach
a
b
s
t
r
a
c
t
Background:Combinedabdominalandtransvaginalanteriorperinealapproacheshavebeen usedasanalternativesurgicalmethodforthesurgicaltreatmentofthelowerrectalcancer. Themainaimofthispaperistodescribethesurgicalstagesofthecombinedabdominal andtransvaginalapproachesperformedforlowerrectalcancer,especiallyintransvaginal anteriorperinealstage.
Method:We have performed sphincter-savingsurgical operationsby using transvaginal anteriorperinealaccessbycombiningwiththeabdominalaccessinfourfemalepatients whohadlowerrectalcancer.
Results:Sphincter-savingextrasphinctericdissectionandproximalsegmentalsphincteric excision techniques were performed in four female patients operated with combined abdominalandtransvaginalanteriorperinealapproach.Allpatientswerefoundtohave con-tinence.Postoperatively,onepatientwasconvertedtoabdominoperinealrectalamputation duetothedetecteddistalresectionmarginpositivity.
Conclusion:Transvaginalanteriorperinealaccessprovidestheextrasphinctericrectal dissec-tionpossibilityintheischioanalfossa.Therefore,thecombinedabdominalandtransvaginal anteriorperinealapproacheshavebeenbasedonthedifferentanatomicalandsurgical fea-tureswhencomparedtointersphinctericdissectiontechniquewhichisthemostcommon usedsurgicalprocedureinlowerrectalcancersurgery.
©2017SociedadeBrasileiradeColoproctologia.PublishedbyElsevierEditoraLtda.This isanopenaccessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/
licenses/by-nc-nd/4.0/).
E-mail:[email protected] http://dx.doi.org/10.1016/j.jcol.2017.05.005
jcoloproctol(rioj).2017;37(4):332–335
333
Técnicas
de
dıssecc¸ão
retal
extra-esfincteriana
e
de
excisão
esfincteriana
segmentar
proximal
com
preservac¸ão
de
esfíncter
com
o
uso
de
acesso
abdominal
e
perineal
anterior
transvaginal
combinado
em
mulheres
portadoras
de
câncer
retal
baixo
(
Ressecc¸ão
anterior
do
reto
baixa
por
via
transvaginal
)
Palavras-chave: Câncerderetobaixo Cirurgiacompreservac¸ãode esfíncter
Abordagemabdominaleperineal combinada
r
e
s
u
m
o
Introduc¸ão:Umacombinac¸ãodeabordagensabdominaleperinealanteriortransvaginaltem sidoempregadacomométodocirúrgicoalternativoparaotratamentocirúrgicodocâncer deretobaixo.Oprincipalobjetivodopresenteartigoéadescric¸ãodosestágioscirúrgicos dasabordagensabdominaletransvaginalcombinadasrealizadasparacâncerderetobaixo, especialmentenoestágioperinealanteriortransvaginal.
Método: Realizamosoperac¸ões cirúrgicascom preservac¸ão de esfíncter como usodo
acessoperinealanteriortransvaginal,emcombinac¸ãocomoacessoabdominal,emquatro pacientesmulheresportadorasdecâncerderetobaixo.
Resultados: Realizamostécnicasdedissecc¸ãoextra-esfincterianaedeexcisãoesfincteriana segmentalproximalcompreservac¸ãodeesfíncteremquatropacientesoperadascomuma combinac¸ãodeabordagensabdominaleperinealanteriortransvaginal.Todasaspacientes estavamcontinentes.Emumapaciente,houvenecessidadedeconversãoparaamputac¸ão retalabdominoperineal,portersidodetectada,nopós-operatório,positividadenamargem deressecc¸ãodistal.
Conclusão: Oacessoperinealanteriortransvaginaltornapossíveladissecc¸ãoretal extra-esfincteriananafossaisquioanal.Portanto,asabordagenscombinadasabdominaleperineal anteriortransvaginalsebaseiamemdiferentescaracterísticasanatômicasecirúrgicas,em comparac¸ãocomatécnicadedissecc¸ãointeresfincteriana,queéoprocedimentocirúrgico deusomaiscomumnacirurgiaparacâncerderetobaixo.
©2017SociedadeBrasileiradeColoproctologia.PublicadoporElsevierEditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http://creativecommons.org/
licenses/by-nc-nd/4.0/).
Introduction
Transvaginalaccessinrectalsurgeryhasbeenusedforover onehundredyears.Transvaginallocalresectionofrectal neo-plasmsusing transvaginalroute isencounteredasMurphy methodinSirCharles Ball’s book “TheRectum”.1 Wehave foundareportdescribingtransvaginalrectalresectionin addi-tiontoabdominalaccesswrittenbyCastro.2
Combinedabdominalandperineal(anteriororposterior) approacheshavebeencollectingarisinginterestas alterna-tivesphincter-savingsurgicalmethodsinlowerrectalcancer surgeryinrecentyears.3–5Also,transvaginalaccessuse pro-videsthe perfect anterior perineal rectal exposition. All of thecombinedabdominalandperineal(anteriororposterior) approacheshavebeenbasedonthesimilaranatomicaland surgicalfeaturesunliketheintersphinctericrectaldissection technique.6Thesefeaturescanbesummarizedastheuseof thesphincter-savingextrasphinctericdissectionandproximal segmentalsphinctericexcisiontechniques.3,5
The main aim of the perineal access use in combined approachesistoprovidetheextrasphinctericrectalexposition ofthesurgicalanalcanalintheischioanalfossa.Surgicalanal canalisconstitutedbytwointertwinedcylindricalmuscular tubes.Theexternalsphinctericmusculature,whichhasa coil-likeshape,canbeconsideredastheouteroneofthesetwo intertwinedmuscletubes.Anatomicalanalcanalanddistal partsofthelowerrectumconstitutetheinnersidemuscular
tubesettledinsidetheexternalanalsphinctericsystem. Inter-sphinctericspaceisapotentialspacebetweentwocylindrical musculartubesinwhichintersphinctericdissectioniscarried out.Extrasphinctericdissectionpossibilityonthesurgicalanal canalprovidedviatheperinealapproachrevealsthe anatom-icalandsurgicaldifferencesofthecombinedabdominaland perineal approaches unlike the intersphincteric dissection technique.
Method
The patients were prepared inthe Lloyd-Davies lithotomy positionontheoperatingtable.Operations wereperformed intwophases, includingabdominaland transvaginal ante-rior perinealphases. Therectosigmoiddissectionand total mesorectal excision were done until reaching up to the puborectalmusclelevelintheabdominalphaseofthe oper-ation. In the transvaginal anterior perineal phase of the operation,transsphincteric distalrectalresection, proximal segmentalsphincterexcisionandcoloanalanastomosiswere performed after providing the extrasphincteric rectal dis-section in the ischiorectal fossa. Ischioanal fossa do not contain the mesorectal tissue. Therefore, total mesorec-tal excision is performed in the abdominal phase of the operations.
334
jcoloproctol(rioj).2017;37(4):332–335notbefamiliarformostofthem.Therefore, wewouldlike toreferaboutanatomicalandsurgicalfeaturesencountered inthetransvaginalanteriorperinealphaseoftheoperation, ratherthanintheabdominalphase.
Anellipticincisionbetweenthevaginalmucosaandthe dermisattheposteriorvaginalfourchettewasusedfor pro-viding the transvaginal rectal access. Surgical anal canal liberalizationfromsurroundingtissueswasperformedinthe extrasphinctericplaneafterpassingthroughrectovaginal sep-taltissues.Whenthesurgicalexpositionwasprovidedinthe ischioanal fossa by using transvaginal rectal access, distal part ofthe rectum surrounded with external anal sphinc-teric system (the surgicalanal canal) was encountered. At thisstageoftheoperation,abdominalandtransvaginal peri-nealdissectionlineswereconnectedwitheachotherafterthe separationofthefibrousadhesionsatthepuborectalmuscle level.Therefore,fullrectalmobilizationwasprovidedby con-nectingtheabdominopelvicspaceandischioanalfossa.After the distal resection line determinationand the placement ofthefixationsutures,distalrectalresectionwasperformed transvaginally.
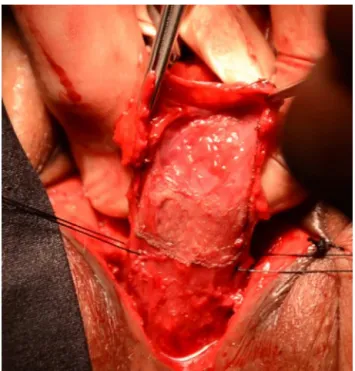
Whenthedistalrectalresectionwascommencedinthe ischioanal fossa transvaginally,it is possible to show that distalresectionlineisinthetranssphinctericplaneas depend-ent to transectionof the external sphinctericmusculature surrounding the distal rectum. At this stage of the oper-ation, the proximal external sphincteric segment, which wouldbeexcised,wasseparated fromcorresponding distal rectalsegmentforshowingtheproximalsegmental sphinc-teric excision (Figs. 1 and 2). After the completion of the transsphinctericdistalrectalresection,thedistalanal exter-nalsphinctericsegmentwasfixatedtoboweledgestoprevent thedistalanalsphinctericsegmentretraction(Fig.3).A full-thicknesscoloanalanastomosisbyusingtransvaginalroute was performed between the colon and distal anal sphinc-tericsegment,aftercompletionoftherectosigmoidresection (Fig.4).Abdominalandvaginalincisionswereclosedfollowing thecoveringileostomy.Postoperatively,coveringileostomies wereclosedinthesecondmonths.
Fig.1–Theverticalincisionperformedtoproximalanal
sphinctericsegmentforshowingthelowerrectum.
Fig.2–Theretractionoftheproximalanalsphincteric
segmentforshowingtheintersphinctericspaceandlower
rectum.
Fig.3–Thefixationofthedistalanalsphinctericsegment
totheboweledgesforpreservingtheremainingdistalanal
sphinctericretractionaftertranssphinctericrectalresection.
Results
jcoloproctol(rioj).2017;37(4):332–335
335
Fig.4–Ultra-lowcoloanalanastomosisviatransvaginal
accessintheischioanalfossa.
exceptonepatientwhohadconvertedtoabdominoperineal rectalamputationduetodistalresectionmarginpositivity.
Discussion
Combinedabdomino-transvaginalrectalresectiontechnique hasdifferent anatomical and surgicalfeatures when com-pared with intersphincteric dissection technique which is themostcommonlyusedsphincter-savingsurgicaltechnique inthe lower rectal cancer surgical treatment described by Schissel et al.6 There is a common truth behind all con-ceptuallysimilarscientificstudies.Themainreasonforthe anatomical and surgical differences in the combined and perineal approaches istouse the perineal access. Perineal accessuse allows extrasphinctericrectal dissectionon the surgicalanal canalinthe ischioanalfossa.All ofthe com-bined abdominoperineal (anterior or posterior) approaches have been based on the similar anatomical and surgical features.3,5 Combined abdominal and perineal (anterior or posterior)approachescanbedescribedassurgicalprocedures in which the sphincter-saving extrasphincteric dissection andproximalsegmentalsphinctericexcisiontechniquesare performed. Itispossibletoreach toischiorectalfossa eas-ily with transvaginal route and to realize an alternative
sphincter-savingresectionmethodinthesurgicaltreatment oflowerrectalcancers.
Although the combined abdominoperineal approaches seemtohavethehighercomplicationratioscomparedtothe intersphincteric dissectiontechnique, it should be remem-beredthatthecombinedabdominoperinealapproacheshave beenperformedintheextrasphinctericplane.Itwasshown that rectal resections performed bymeans of extrasphinc-tericrectaldissectiontechniqueareoncologicallysuperiorto rectal resectionsrealizedbymeans ofintersphincteric dis-section techniqueinlower rectalcancersurgery.7Although itistooearlytodiscussontheoncologicaloutcomesofthe combinedabdominalandperinealapproaches,thesafer onco-logicalresultsintermsoftheradialspreadofthetumorcannot beasurprise.
Conflicts
of
interest
Theauthordeclaresnoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.BallC.Therectum.It’sdiseasesanddevelopmentaldefects.
London:OxfordMedical;1908.p.276–82.
2.CastroAF.Vaginalapproachinresectionoflow-lying
malignantlesions.TexMed.1974;69:65–9.
3.PenaA,HongA.Theposteriorsagittaltrans-sphinctericand
trans-rectalapproaches.TechColoprotocol.2003;7:35–44.
4.WilliamsNS,MurphyJ,KnowlesCH.Anteriorperinealplanfor
ultra-lowanteriorresectionoftherectum(theAPPEAR
technique):aprospectiveclinicaltrialofanewprocedure.Ann
Surg.2008;247:750–75.
5.YücesoyAN,Poc¸anS.Lettertoeditoron“Thecombined
abdominalandperinealapproachfordissectionoftherectum.
Thedevelopmentofnewindications”.Howcanwedescribe
theanatomicalandsurgicalbasisofthecombinedabdominal
andperinealapproachesinlowerrectalcancersurgery?IntJ
Surg.2015;19:33–4.
6.SchiesselR,Karner-HanuschJ,HerbstF,TelekyB,Wunderlich
M.Intersphinctericresectionforlowrectaltumours.BrJSurg.
1994;81:1376–8.
7.WestNP,FinanPJ,AnderinC,LindholmJ,HolmT,QuirkeP.
Evidenceoftheoncologicsuperiorityofcylindrical
abdominoperinealexcisionforlowrectalcancer.JClinOncol.