Review
Article
Controversies
in
presacral
tumors
management
Nidal
Issa
a,∗,
Yaniv
Fenig
b,
Nimrod
Aviran
a,
Muhammad
Khatib
a,
Mustafa
Yassin
aaRabinMedicalCenter,Petah-Tikva,andtheFacultyofMedicineTelAvivUniversity,Israel
bMonmouthMedicalCenter,LongBranch,NewJersy,UnitedStates
a
r
t
i
c
l
e
i
n
f
o
Keywords: Presacraltumor Preoperativebiopsy Neoadjuvanttherapy
a
b
s
t
r
a
c
t
Presacraltumorsarerarelesionsoftheretrorectalspacethatcanpresentdiagnosticand therapeuticdifficultybecauseoftheiranatomiclocationandthedifferenttissuetypesand etiology.Althoughthediagnosisandmanagementofthesetumorshasevolvedinrecent years,severalpointsstilltobeaddressedinordertoimproveperioperativediagnosisand treatment.Intheupcomingwewilltry tohighlightsomecontroversialpoints;the pre-operativebiopsies,neoadjuvanttherapy,thenecessityofsurgeryandtheroleofminimally invasivesurgeriesofpresacraltumors.
©2017SociedadeBrasileiradeColoproctologia.PublishedbyElsevierEditoraLtda.This isanopenaccessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/ licenses/by-nc-nd/4.0/).
Controvérsias
no
tratamento
de
tumores
pré-sacrais
Palavras-chave: Tumorpré-sacral Biópsiapré-operatória Terapianeoadjuvante
r
e
s
u
m
o
Tumorespré-sacraissãolesõesrarasdoespac¸oretrorretalquepodemtrazerdificuldades diagnósticaseterapêuticasporcausadesualocalizac¸ãoanatômicaetambémpelos difer-entestiposde tecidoseetiologia.Emboranosúltimosanosodiagnósticoetratamento dessestumorestenhamevoluído,diversospontosaindadevemserestudadoscomvistasà melhoradodiagnósticoetratamentonoperioperatório.Maisadiante,tentaremosesclarecer algunspontoscontroversos;biópsiaspré-operatórias,terapianeoadjuvante,anecessidade decirurgiaeopapeldascirurgiasminimamenteinvasivasparaostumorespré-sacrais.
©2017SociedadeBrasileiradeColoproctologia.PublicadoporElsevierEditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http://creativecommons.org/ licenses/by-nc-nd/4.0/).
Introduction
Presacraltumorsareheterogeneousandrelativelyrare.Given thesecharacteristics,theclinicalpresentation,naturalhistory andtreatmentofpresacraltumorsisnotwellunderstood.
∗ Correspondingauthor.
E-mail:[email protected](N.Issa).
Thepresacralspaceisboundedbytheperitoneal reflec-tionandtherecto-sacralfascia.Theembryologicdevelopment at this anatomical site iscomplex due tothe presenceof totipotentialgermcellsthatdifferentiateinto3germcell lay-ers.Thisinturnleadstothedevelopmentofdifferenttypes oftissuesincludingconnectivetissue,nerves,fat,andblood vessels. Themultitudeoftissuetypesgives riseto numer-ous tumor pathologies. In addition, because the presacral spacehasdiversehistopathologicalfindings,physiciansfrom
http://dx.doi.org/10.1016/j.jcol.2017.06.006
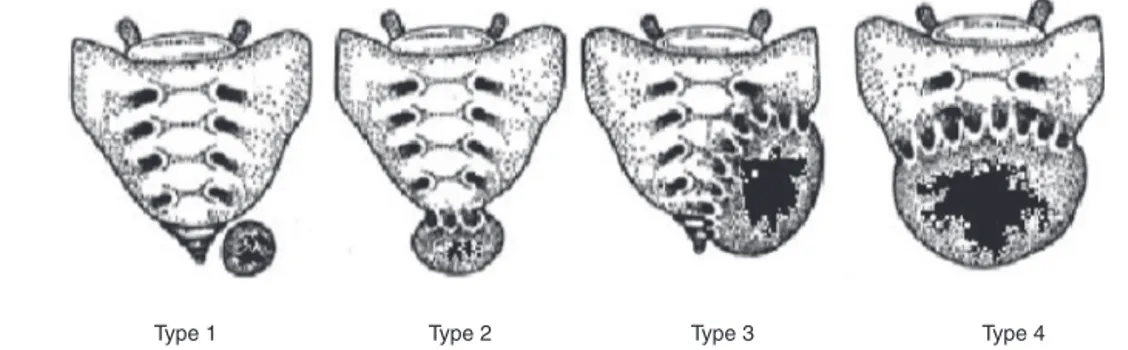
Type 1 Type 2 Type 3 Type 4
Fig.1–Classificationbasedontumorlocation.
diverse subspecialtiesincluding colorectal surgeons, obste-tricians and gynecologists, urologists, neurosurgeons, and orthopedicsareofteninvolvedinpatientcare.
Pre-sacraltumorswerereportedforthefirsttimeinthe middleofthe19thcentury.Kiderlenetal.reportedsixcases in1899includingateratoma,whichwasthefirstreportedcase byEmmerich.Thefirstpre-sacraltumorwasresectedbyDr. Middledorpf,andthistumorwasnamedafterhimformany years.1
Thetrueincidenceofpre-sacraltumorsinthegeneral pop-ulationishard toassessbecause many reportscomefrom tertiarycentersandsodonotrepresentthetrueincidence. Theestimatedincidenceisabout1caseinevery40,000 hos-pitaladmissions.Mostofthepublicationsareindividualcase reportsandsmallcaseseries.2–4
Asaresultofthelowincidence,thereisnouniform clas-sificationsystemfortheselesions.Fouryearsago,Uhligand Johnsonsuggestedaclassificationforthesetumorsaccording toitstissueoforigin.2PhysiciansatTelAvivMedicalCenter
proposedanotherclassificationsystembasedonwhetherthe lesioniscongenitaloracquiredaswellaswhetheritisbenign ormalignant.5
Yetanotherclassificationsystemisbasedontumor loca-tionanditscommunicationwiththesacrumand/orcoccyx (Fig.1).Usingtumorlocationasthebasisfortheclassification facilitatesthesurgicalapproach.6 Accordingtothis
classifi-cationtype1:thelesionislocatedatthecoccyxlevel(below S3)andseparatedfromthebonytrunkofsacrococcyx,type2 astype1buthasconnectionwiththecoccyxsacrum.Type3 thelesioninvolvesthesacrumatorabovetheS3nerveroot unilaterally,andtype4whenlargecommunicationwiththe sacrumatoraboveS3bilaterally.
Further, the above classification system reflects post-operativecomplications:resectionoftype1and2usuallydoes nothaveneurologicalsequelaandtypes3and4usuallyresult intemporaryorpermanentincontinence.6
In recent years, the classification system proposed by DozoisandJacofskyfromtheMayoclinicismostcommonly used. According to this classification (Table 1), tumors are divided into 5 categories which are further grouped into benignandmalignant.7
Abouttwothirdsofallthepre-sacraltumorsare congeni-tal.Mostofthosearecysticandbenign.10%areofneurogenic inorigin,5–10%areofboneorigin andabout15% arefrom otherorigins,includingmetastasis.8Ingeneral,benignlesions
are more common in females, while malignanttumorsare
Table1–Classificationofpresacralretrorectaltumors.
Sourceoforigin Histopathology
Congenitalordevelopmental
Benign Developmentalcysts Dermoidcysts Epidermoidcysts Tailgutcysts
Enteric(rectal)duplication Anteriorsacralmeningocele Teratoma
Adrenalresttumors
Malignant Chordoma
Teratocarcinoma
Inflammatory Granulomas(foreignbody)
Perineal/pelvirectalabscessorfistula
Neurogenic
Benign Neurofibroma
Neurolemmoma(schwannoma) Ganglioneuroma
Malignant Ependymoma
Ganglioneuroblastoma Neurofibrosarcoma
Osseous
Benign OsteomaSacralbonecyst Osteoblastoma
Osteogenicsarcoma Giantcelltumor
Malignant Ewing’stumor Chondromyxosarcoma Osteogenicsarcoma Myeloma
Miscellaneous
Benign Lipoma
Fibroma Leiomyoma Hemangioma Endothelioma Desmoidtumor Lymphangioma Ectopickidney
Malignant Fibrosarcoma Liposarcoma Leiomyosarcoma Metastaticdisease
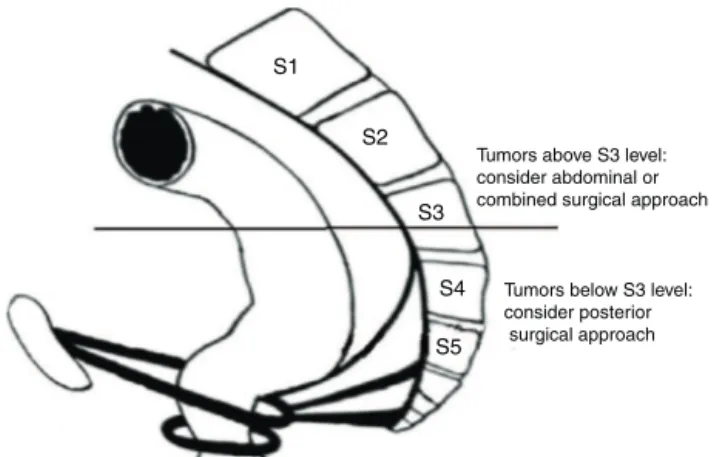
S5
consider posterior surgical approach
Fig.2–Anatomicdelineationinrespecttosurgical approach.
Malignancyhasbeenreportedatarangeof9–45%ofall pre-sacraltumors.9Themostcommonmalignantpre-sacral
tumorsareChondromas.Theyareslowgrowingcancers, usu-allyasymptomatic,butsymptomsmay presentlaterinthe coursewithinvasionintoneurologictissues. Thesetumors metastasizetobone,liverandlungin20%ofcases.8
Besidesphysicalandrectal examinations,thestandards methodsofevaluationareCTscansandMRIs.ACTscancan determinewhetherthelesioniscysticorsolidandwhether thereisanyboneinvolvement.AnMRIcanprovidemore infor-mationregardingspinalinvolvement,butmoreimportantly, itisabletogiveanestimationofthehistologyofthetumor. Transrectalultrasoundandangiographymayalsohavearole intheworkup.10,11
Theappropriatesurgicalapproachforpre-sacraltumorsis ascertainedbypre-operativediagnosisandthedemonstration ofanatomicconditionssuchaslocation,sizeandinvolvement ofadjacent structures.12 Thecommon surgical approaches
includea)anteriortrans-abdominal,b)posterior-perineal,and c)thecombinedapproach.Smallandlowlyinglesionsbelow S3canberemovedviatheposteriorapproach,either trans-sacralor para-sacral. Tumors above the level ofS3 can be resectedvia the anterior trans-abdominalor thecombined approachdepending onthe needforboneresection. Fig. 2 illustratestheanatomyassociatedwiththevarioussurgical approaches.
Ingeneral,benignlesionsshouldberemovedcompletely, usuallywithlimiteddissection.Malignanttumorsrequire rad-icalresection, sometimeswithextensive excision ofpelvic structuresincludingthesacruminordertoachievenegative surgicalmargins.Oneofthemostimportantprognostic fac-torsare negativesurgical margins.If wide marginsare not achieved,onecan expecthigh recurrenceratesand poorer survival.AstudyfromTelAvivMedicalCentershowedthat afterresectionofmalignantpre-sacraltumors,mostofthe recurrenttumorswereincompletelyresectedand50%ofthese patientsdiedoftheirdisease.6
Theoverallsurvivalforbenignpre-sacrallesionsisnearly 100%,withalowerrecurrencerate.Formalignantlesions,the overallsurvivalis74%andthe10-yearsurvivalrateisabout 32%.Therateofrecurrenceinsuchcasesishigh,reachingas highas75%insomereports.10,13
Pre-operative
biopsy
Theexistingparadigmregardingpre-operativebiopsyisthat itisnotrecommendedbecauseoftheriskofseptic compli-cationsand tumorseeding.Datafrom the Mayoclinic, the largestreportedseriesofalltumorsbetween1960and1979, supportsthis recommendation.5 Theauthors ofthis series
reported higher recurrence rates inpatients that had pre-operativebiopsyasopposedtothosewhodidnot.Ontheother hand,inacaseseriesfromMemorialSloanKetteringCancer Center(MSKCC)of27patientswhohadapre-operativebiopsy, 12viatheopenapproachand15vianeedlebiopsy,noneofthe patientsexperiencedcomplicationsandthepathologyresults werehighlyaccurateindetectingmalignancy.14A
retrospec-tiveanalysisconductedbytheMayoclinicusingalltheircases inthelast20yearsprovidesfurtherevidenceoftherelative safetyofperformingapre-operativebiopsy.Inthisseries,they onlyhad2hematomasoutof76biopsies.Theyalsoshowed thatpre-operativebiopsycanguidethesurgicalapproachand avoidextensiveresectionsinpatientswithabenignpathology. Theyshowedthatthepre-operativebiopsywasin concord-ancewiththe finalpathologiesatahigherratethan those resultingfromthevariousimagingtechniques.15
In cases wherea tumoris resectable, it may seem like apre-operativebiopsyisnotrequired.But,inthecaseofa similarlesionlikeneuro-fibromaandneuro-fibro-sarcoma,a pre-operativebiopsyisneededtodistinguishbetweenthem. Sothisleadstothequestion:Shouldwebiopsyalltumors?All solidtumors?
Mercheaet al.fromtheMayoclinicprovidesananswer. Theysuggestthatapre-operativebiopsyinnon-cysticlesions shouldbeconsidered,ifthereisanydoubtregardingthe pre-cisediagnosis and if thebiopsy canchange the surgeryor guidethemanagement.29Itseemsthatmanytumorsmeetat
leastoneofthesecriteria.Giventhisrecommendation,wesee anincreasingtendencyinperformingpre-operativebiopsies inpre-sacrallesions.
Neoadjuvant
therapy
Neoadjuvant therapy has many known benefits including treatingmicro-metastasisaswellasdown-sizingand down-stagingthe tumor.Somepre-sacraltumors,likeosteogenic sarcoma and neurofibrosarcoma, are sensitive to chemo-radiation.16Sometumorscanevenreachcompleteresponse.
The
necessity
of
surgery
Ifyouhaveasmallcystthatisbenignandasymptomaticand islocatedbehindtherectum,isitdefinitelyindicatedtoresect it?Therearenoreportsanalyzingconservativemanagement ofpre-sacralbenigncysticlesions,perhapsbecauseofits rar-ity.Paradoxically,theonlyreportofaconservativeapproach wasmorethan50yearsagofromtheMayoClinicanditwas theresultofapoorsurgicaloutcomeandnotbecauseofthe benignnatureofthelesion.19,20 Manyfeelthatallpresacral
lesions,evensmallbenigncysts,shouldberemovedforseveral reasons:cystscanbecomeinfected,haveamalignant trans-formation,ortheycanenlarge andmakethesurgerymore complicated.
The
role
of
minimally
invasive
surgical
approaches
Inadditiontotheadvantagesoflaparoscopyingeneral,the literature reports several specific advantages of minimally invasivesurgery(MIS)inpre-sacraltumorsintermsofsafety, visualizationofthepre-sacralspaceandcompletenessofthe resection.21,22Laparoscopymaybeanalternativetothe
ante-riorabdominalapproachandinsomecasesitcanreplacethe combinedapproach.23,24However,mostpresacraltumorsare
smalllesionsandarebothcysticandbenign.Therefore,there isnotsufficientevidencetosupportlaparoscopicresectionof malignantpre-sacrallesions.
Thereareseveralreportsontheuseofrobotictechniques forpre-sacraltumors.25Thiscansometimesreplacethe
poste-riorapproach,suchastheTransanalEndoscopicMicrosurgery (TEM),byentering the pre-sacralspace through the poste-riorwalloftherectum.TEMhasmanyadvantagesthatcan facilitatetheexcisionofthelesioninalmostanyplace retro-rectally.ThereareseveralseriesofTEMexcisionofretro-rectal pre-sacralcystswithexcellentoutcomesandcomplete exci-sionofthelesions.26,27ArecentreportfromRambamMedical
CenterinIsraelreportedthesuccessfulandnon-complicated resectionoffourpre-sacraltumorsusingTEM.28
TherearealsodisadvantagestousingTEMfortheresection ofpre-sacraltumors.First,infectionsmaybeintroducedwhen enteringthepre-sacralspacethroughtherectum.Second,and moreimportantly,theuseofTEMfortheresectionofpresacral tumorscomeswithariskofsacralbleeding.
Conclusion
Inconclusion,pre-sacraltumorsarequiterare.Isseemsthat thereisanindicationforapre-operativebiopsywheneverit caninfluencethemanagement. Minimallyinvasivesurgery gainsmoreacceptancesrecentlyforresectionofbenign pre-sacral lesions. Though for malignant lesions, neoadjuvant therapy shouldbe considered, sonegative margins can be assured.Thiscanbeachievedbyanexperiencedteamata referralcenterthathassufficientnumbersofpatientswith presacraltumorstogaintheexperiencerequiredtosafelytreat thesepatients.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.WittakerLD,PembertonJD.Tumorsventraltothesacrum. AnnSurg.1938;1:96–106.
2.UhligBE,RoderickLJ.Presacraltumorsandcystsinadults. DisColonRectum.1975;18:581–96.
3.SpencerRJ,JackmanRJ.Surgicalmanagementofprecoccygeal cysts.SurgGynecolObstet.1962;115:449–52.
4.JaoSW,BeartRWJr,SpencerRJ,ReimanHM,IlstrupDM. Retrorectaltumors.MayoClinicexperience,1960–1979.Dis ColonRectum.1985;28:644–52.
5.Lev-CheloucheD,GutmanM,GoldmanG,Even-SapirE,Miller I,IssakovJ,etal.Presacratumors:apracticalclassification andtreatmentofauniqueandheterogeneousgroupof diseases.Surgery.2003;133:473–8.
6.LosanoffJE,SauterER.Retrorectalcysts.JAmCollSurg. 2003;197:879–80.
7.DozsiseEJ,JacofskyDJ,DozoisRR.Presacraltumors.The ASCRStextbookofcolonandrectalsurgery.NewYork: Springer;2007.p.501–14.
8.WoodfieldJC,ChalmersAG,PhillipsN,SagarPM.Algorithms forthesurgicalmanagementofretrorectaltumours.BrJSurg. 2008;95:214–21.
9.HobsonKG,GhaemmaghamiV,RoeJP,GoodnightJE,Khatri VP.Tumorsoftheretrorectalspace.DisColonRectum. 2005;48:1964–74.
10.PapparaldoG,FrattaroliFM,CascianiE,MolesN,MascagniD, SpoletiniD,etal.Retrorectaltumors:thechoiceofsurgical approachbasedonanewclassification.AmSurg.
2009;75:240–8.
11.CocoC,MannoA,MattanaC,VerboA,SermonetaD, FranceschiniG,etal.Congenitaltumorsoftheretrorectal spaceintheadult:reportoftwocasesandreviewofthe literature.Tumori.2008;94:602–7.
12.SzylloK,Lesnik.Sacrococcygealteratoma—casereportand reviewoftheliterature.AmJCaseRep.2013;14:1–5.
13.McMasterML,GoldsteinAM,BromleyCM,IshibeN,ParryDM. Chordoma:incidenceandsurvivalpatternsintheUnited States,1973–1995.CancerCausesControl.2001;12:1–11. 14.CodyHS,MarcoveRC,QuanSH.Malignantretrorectaltumors:
28years’experienceatMemorialSloan-KetteringCancer Center.DisColonRectum.1981;24:501–6.
15.YarramSG,NghiemHV,HigginsE,FoxG,NanB,FrancisIR. Evaluationofimaging-guidedcorebiopsyofpelvicmasses. AmJRoentgenol.2007;188:1208–11.
16.StewartRJ,HumphreysWG,ParksTG.Thepresentationand managementofpresacraltumours.BrJSurg.1986;73:153–5. 17.CattonC,O’SullivanB,BellR,LaperriereN,CummingsB,
FornasierV,etal.Chordoma:long-termfollow-upafter radicalphotonirradiation.RadiotherOncol.1996;41:67–72. 18.ZhangH,YoshikawaK,TamuraK,SagouK,TianM,SuharaT,
etal.Carbon-11-methioninepositronemissiontomography imagingofchordoma.SkeletalRadiol.2004;33:524–30. 19.MacCartyCS,WaughJM,CoventryMB,CopeWFJr.Surgical
treatmentofsacralandpresacraltumorsotherthan sacrococcygealchordoma.JNeurosurg.1965;22:458–64. 20.WaldhausenJA,KolmanJW,VelliosF,BattersbyJS.
Sacrococcygealteratoma.Surgery.1963;54:933–49. 21.BaxNM,vanderZeeDC.Thelaparoscopicapproachto
Endosc.2013;27:4177–83.
25.AgorastosS,AlexA,FeldmanJ,KuncewitchM,DeutschG, SiskindE,etal.Roboticresectionofretro-rectaltumor:an alternativetotheKraskeprocedure.JSolidTumors. 2013;3:13–6.
26.ZollerS,JoosA,DinterD,BackW,HorisbergerK,PostS,etal. Retrorectaltumors:excisionbytransanalendoscopic
EndoscPercutanTechn.2013;1:66–8.