REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
OfficialPublicationoftheBrazilianSocietyofAnesthesiologywww.sba.com.br
SCIENTIFIC
ARTICLE
Effects
of
various
anesthesia
maintenance
on
serum
levels
of
selenium,
copper,
zinc,
iron
and
antioxidant
capacity
Mehmet
Akın
a,
Hilal
Ayoglu
a,∗,
Dilek
Okyay
a,
Ferruh
Ayoglu
b,
Abdullah
Gür
a,
Murat
Can
c,
Serhan
Yurtlu
a,
Volkan
Hancı
a,
Gamze
Küc
¸ükosman
a,
Is
¸ıl
Turan
aaDepartmentofAnesthesiologyandReanimation,BülentEcevitUniversity,SchoolofMedicine,Zonguldak,Turkey bDepartmentofPublicHealth,BülentEcevitUniversity,SchoolofMedicine,Zonguldak,Turkey
cDepartmentofBiochemistry,BülentEcevitUniversity,SchoolofMedicine,Zonguldak,Turkey
Received9March2014;accepted9April2014 Availableonline10May2014
KEYWORDS
Propofol; Desflurane; Sevoflurane; Selenium; Zinc;
Antioxidantcapacity
Abstract
Backgroundandobjectives: Inthisstudy,weaimedtoinvestigatetheeffectsofsevoflurane,
desfluraneandpropofolmaintenancesonserumlevelsofselenium,copper,zinc,iron,
malon-dialdehyde,andglutathionperoxidasemeasurements,andantioxidantcapacity.
Methods:60 patients scheduledfor unilaterallowerextremitysurgerywhichwould be
per-formedwithtourniquetundergeneralanesthesiaweredividedintothreegroups.Bloodsamples
werecollectedtodeterminethebaselineserumlevelsofselenium,copper,zinc,iron,
malon-dialdehyde andglutathionperoxidase.Anesthesiawasinducedusing2---2.5mgkg−1 propofol,
1mgkg−1lidocaineand0.6mgkg−1rocuronium.Inthemaintenanceofanesthesia,under
car-riergasof50:50%O2:N2O4Lmin−1,1MACsevofloranewasadministeredtoGroupSand1MAC
desfluranetoGroupD;andundercarriergasof50:50%O2:air4Lmin−16mgkgh−1propofoland
1gkgh−1fentanylinfusionwereadministeredtoGroupP.Atpostoperativebloodspecimens
werecollectedagain.
Results:Itwas observedthatonlyinGroupS andP, levelsofMDAdecreasedat
postopera-tive48thhour;levelsofglutathionperoxidaseincreasedincomparisontothebaselinevalues.
SeleniumlevelsdecreasedinGroupSandGroupP,zinclevelsdecreasedinGroupP,andiron
levelsdecreasedinall threegroups,andcopperlevelsdidnotchangeinanygroups inthe
postoperativeperiod.
Conclusion: Accordingtothemarkersofmalondialdehydeandglutathionperoxidase,itwas
concluded thatmaintenanceofgeneralanesthesiausingpropofol andsevoflurane activated
∗Correspondingauthor.
E-mail:periayogluzku@yahoo.com(H.Ayoglu).
http://dx.doi.org/10.1016/j.bjane.2014.04.001
theantioxidantsystemagainstoxidativestressandusingdesfluranehadnoeffectsonoxidative
stressandantioxidantsystem.
©2014SociedadeBrasileiradeAnestesiologia.PublishedbyElsevier EditoraLtda.Allrights
reserved.
PALAVRAS-CHAVE
Propofol; Desflurano; Sevoflurano; Selênio; Zinco; Antioxidantes
Efeitosdamanutenc¸ãodeváriasanestesiassobreosníveisséricosdeselênio,cobre, zincoeferroeacapacidadeantioxidante
Resumo
Justificativaeobjetivos: Investigar os efeitos da manutenc¸ão de sevoflurano, desflurano e
propofol sobre nos níveis séricos de selênio, cobre, zinco, ferro e malondialdeído, as
mensurac¸õesdeglutationaperoxidaseeacapacidadeantioxidante.
Métodos: Foramalocadosem trêsgrupos 60pacientesagendadosparacirurgiaunilateralde
membrosinferiores,feitacomtorniquetesobanestesiageral.Amostrasdesangueforam
cole-tadasparadeterminarosníveisséricosbasaisdeselênio,cobre,zinco,ferro,malondialdeído
eglutationaperoxidase.Aanestesiafoiinduzidacom2-2,5mgkg−1depropofol,1mgkg−1de
lidocaínae0,6mgkg−1derocurônio.Namanutenc¸ãodaanestesia,sobgásdetransportede50%
O2e50%N2O(4Lmin−1),sevofluranoa1CAMfoiadministradoaoGrupoSedesfluranoa1CAM
aoGrupoDe,sobgásdetransporteemmisturade50%O2e50%ar(4Lmin−1),6mgkgh−1de
propofole1mgkgh−1defentanilforamadministradosaoGrupoP.Nopós-operatório,amostras
desangueforamnovamentecoletadas.
Resultados: ApenasnosgruposSePosníveisdeMDAdiminuíramem48horasdepós-operatório;
osníveisdeglutationaperoxidaseaumentaramemcomparac¸ãocomosvaloresbasais.Osníveis
deselêniodiminuíramnoGrupoSenoGrupoP,osníveisdezincodiminuíramnoGrupoP,os
níveisdeferrodiminuíramemtodososgruposenãohouvealterac¸ãonosníveisdecobreem
nenhumgruponoperíodopós-operatório.
Conclusão:De acordocom os marcadoresde malondialdeído eglutationa peroxidase,
con-cluímos quea manutenc¸ão daanestesia geralcom propofole sevoflurano ativouo sistema
antioxidantecontraoestresseoxidativoeousodedesfluranonãoteveefeitossobreoestresse
oxidativoeosistemaantioxidante.
©2014SociedadeBrasileiradeAnestesiologia.PublicadoporElsevierEditoraLtda.Todosos
direitosreservados.
Introduction
Thepurposeingeneralanesthesiapracticesistodecrease thepotentiallyharmfulconditionsfor theorganismtothe lowest level as well as conducting the anesthesia effec-tively.Duringgeneralanesthesia, stressdue toanesthesia andsurgeryandimmunologicaldefensemechanismscanbe disrupted, and macrophages cause releasing of free oxy-gentotheenvironmentbyinducinginflammatoryreaction. Theseradicalsleadformationoftoxicmetabolitessuchas malonyldialdehyde(MDA)bycausingcellulardamagewith lipidpreoxidation.1,2
MDAisusedasanindirectindicatorofoxidativedamage thatitslevelcanbe detectedin thesystemiccirculation, andasamarkerofischemia---reperfusiondamage.3
Antioxidant enzymes such as glutathione peroxidase (GPx),superoxidedismutase(SOD)andcatalase(CAT)play role as the defense mechanism in the body against tis-suedamagecausedbyreactiveoxygensubstrates (ROCs).4
Activities of these enzymes are dependent on the syn-thesis and degradation rates of free radicals, nutrition, and condition of trace elements. Trace elements play
cofactor-key role in cleaning of free oxygen radicals in antioxidantsystems.5,6
Tourniquet is used to decrease bleeding in extrem-ity surgery,and presence ofischemia reperfusiondamage caused by free oxygen radicals depending on tourni-quet application was shown in previous studies.7 Use of
immunosuppressants, corticosteroids, anesthetics, various anesthetic methods and antioxidants for the purpose of decreasing free radicalsin the preventionof this damage wasstudied.3,8---10
It was shown in the studies that effects of anes-theticagents onoxidative stress andantioxidantcapacity vary.1,11,12Volatileanestheticswereshowntoinduce
oxida-tivestressandinflammatoryresponsewithcausingrelasing of free radicals such as inflammatory mediators and superoxide anions, with decreasing antioxidant defense mechanisms, and withinducing geneexpression of proin-flammatorycytokines,aswellasitwasreportedthatsome anestheticscouldalsohaveantioxidanteffects.13---19Besides
Inthepresent study,weplannedtoresearcheffectsof threedifferentgeneralmaintenanceofanesthesia (sevoflu-rane,desfluraneandpropofol)ontraceelements,oxidative stressandantioxidantcapacitywithmeasuringserum lev-els of Se, Cu, Zn, Fe, MDA and GPx in the patients who wereplanned toundergo extremitysurgery withapplying tourniquet.
Materials
and
methods
This study was conducted prospectively with approval of theBulentEcevitUniversityEthicsCommittee(08.03.2011, Meeting decisionno:2011/02) andafterreceivingwritten informedconsentformsfromthepatients.
A total of 60 patients over 18 years old and between 60 and 100kg in weight who were American Society of AnesthesiologistsStatus (ASA) I---IIIand whowere planned lowerextremity surgerywithapplyingaunilateral tourni-quet in elective conditions and under general anesthesia wereincludedinthestudy.Theexclusioncriteriawerethe presenceofanycardiovascular,respiratoryand cerebrovas-cular diseases, severe liver or kidney failure (creatinin clearence<60mLmin−1), diabetes mellitus, pregnancy, obesity (BMI>30kgm2), autoimmune disease, history of treatmentwithimmunosuppressants,historyofSe,Zn,Cu, Fe and antioxidanttherapy withinthe lastthree months, historyofallergytothedrugsthatwouldbeused,andcases withatourniquetperiodshorterthan60minorlongerthan 150min.
Thecaseswererandomlydividedintothreeequalgroups [Group S (sevoflurane), Group D (desflurane), Group P (propofol)].
Premedication of midazolam 0.07mgkg−1 was admin-istered to all patients 30min before the operation. Standard anesthesia monitorization [electrocardiogram (ECG), peripheral oxygen saturation (SpO2) and noninva-sivearterialbloodpressure]wasperformedforthepatients taken intothe operation room,and baseline values were recorded.Avascularaccesswasestablishedthroughawide cubital vein using a 16G angiocath. Blood samples were takenfordetectionofbaseline(T1)serumlevelsofSe,Cu, Zn,Fe,MDAandGPx.Avascularaccesswasestablishedin the other arm for liquid infusions usinga 20G angiocath. Salineinfusionof8---10mgkgh−1wasstarted.
Allthepatientswereadministeredpreoxygenationwith 10Lmin−1 of 100% oxygen for 1min. Anesthesia induction wasprovidedusing2---2.5mgkg−1ofpropofoland1mgkg−1 oflidocaine.Intubationwasperformed2minafter adminis-trationof0.6mgkg−1ofrocuroniumasthemusclerelaxant. Maintenanceofanesthesiawasprovidedunder4Lmin−1 carrier gas as 50:50% O2:N2O using 1 MAC sevoflurane in Group S, under 4Lmin−1 carrier gas as 50:50% O2:N2O using 1 MAC desflurane in Group D, and administering 4Lmin−1freshgasas50:50%O2:airusing6mgkgh−1 propo-fol and i.v. infusion of 1gkgh−1 fentanyl in Group P. In allthreegroups, ventilationtidalvolumewasprovidedas 6---8mLkg−1,I:Eratewas1:2,andrespirationratewas pro-videdtoachievenormocapniaassettingtheEtCO2levelto 35---40mmHg.
Following theintubation, the extremity that would be operatedwaswrappedusingEsmarchbandageafteritwas elevated, and tourniquet was applied at a pressure of
300mmHg.Itwasplannedtoadminister50gi.v.fentanyl incasesofincreaseof20%ormoreinthebaselinevaluesof intraoperativearterialbloodpressureorheartrate.
Patients’ demographic data, operative and tourniquet time, bleeding, quantities of the blood given, ASA lev-els,smokingandalcoholabuse(recordedaspresent/none), typesofoperations(recordedas1---footfracture,2---tibia fracture,3 --- knee meniscopathy,4 --- ankle fracture, 5 ---kneeprosthesis),occupationalgroups(recordedas1--- min-ers,2---self-employed,3---officer,4---smith,5---welder,6 ---unemployed),intraoperativeadditionaldruguse(recorded as1---none,2---pheniraminemaleate+dexamethasone,3 --- methylprednisolone+ranitidine,4 --- glyceryltrinitrate), postoperativeadditionalproblems(recordedas1---present, 2---none, 3---bronchospasm, 4---nausea,5--- vomiting,6 ---itch)weresaved.When thelastskinsuturewasstarted beforetheoperation ended,the patientswere ventilated using100%O2 afteranesthetics werediscontinued.Muscle relaxanteffectwasantagonizedusing0.05mgkg−1 neostig-mineand0.01mgkg−1atropineintravenously.
Allthepatientswereadministered1mgkg−1i.v.tramadol forpostoperativepaincontrol15minbeforetheoperation ended.Postoperative analgesia wasmaintained using tra-madolas10mgbolusand10minlockwithpatient-controlled analgesia(PCA)method.Amountoftramadolconsumedwas recorded.
Bloodsamplesweretakenagainfordetectionofserum levelsof Se,Cu, Zn,Fe, MDA,and GPx in the postopera-tive 0th (T2), 24th (T3), and 48th (T4) hours. The blood sampleswerecentrifugedat5000rpmfor5mininthe bio-chemistrylaboratoryimmediately,andtheserumextracted werestoredat−40◦
C.
MDAmeasurement
Serum MDA levels were tested using commercial kits (Immundiagnostik, Bensheim, Germany) by high perfor-manceliquidchromatography(HPLC)methodwithanHPLC device(Agilent1200,Munich,Germany).Workingprinciple of the test is based on conversion of MDA to a fluores-centproduct asa result of a sample preparationprocess performed usinga derivation reactive.Fluorometric mea-surementwasdonein515nmexcitationand553nmemission afterseparationof20LreactionmixcontainingMDA con-verted to a fluorescent product using reverse phase C 18 column at 30◦C. Detection limit of the method was
0.15molL−1,anditslinearitywas100molL−1.
GPxmeasurement
SerumGPxactivitywasmeasuredwithPagliaandValentine method.H2O2wasusedassubstrateinthemeasurementof enzymeactivity,andNADPHoxidationwasdetected spec-trophotometricallyat 340nm. The results wereexpressed asUL−1.
Measurements
of
trace
elements
Copperandzinc
Selenium
ThestudywasconductedusingPerkinElmerbrandedAtomic AbsorptionSpectrometer (AAS),andhydride system(FIAS) wasusedasfollows:1unitserum+6unitacidsolution (per-chloric/nitricacidsolution,5/1)washydrolysedat120◦
Cfor 1h.Atotalof3mL50%HClwasadded,andwashydrolysedat 120◦
Cfor1hagain.Then3mLwaterwasaddedandthelast readwasdone.Five-pointcalibrationwasperformed using InorganicVentures brandedstock.Twolevelswereusedas controlssuchasSerenomTraceElementsSerumL-1 (sele-nium level 100---114gL−1) and Serenom Trace Elements SerumL-1(seleniumlevel 153---173gL−1).The reference range was 46---143gL−1 for serum selenium level in the laboratorythatthemeasurementwasperformed.
Iron
Iron measurement was carried out using the Ferrozine method.Accordingtothismethod,ironwasreleasedfrom transferrinunderacidicconditions,wasreducedtoferrous form,and wascoupled with a chromogen for the colori-metricmeasurement.Inthisprocedure,ironwasmeasured directly without any steps of proteindenaturation or any interactionswithanendogenouscopper.
Ferricironwasseparatedfromthecarrierprotein trans-ferrininacidiccondition,andwasreducedsimultaneouslyto ferrousform.Thenironformedacomplexwithferrozine,a sensitiveironindicator,andformedacoloredchromophore thatexhibitsabsorbanceat571/658nm.
Reactionequation
Transferrin(Fe3+) →Apotransferrin +Fe3+
Fe3+
+AscorbicAcid → Fe2+
Fe2+
Ferrozin → Fe2++
Ferrozincomplex
Referencevalues
Male:65---175g/dL(11.6---31.3mol/L). Female:50---170g/dL(9.0---30.4mol/L).
Statisticalanalysis
Surveydatacollectedduringtheresearchweretransferred to the software ‘‘SPSS for Windows 16.0’’, and were
analyzed. Average values were expressed as mean±standard deviation (SD). The chi-square test was used in the comparison of distribution of qualitative datasuchasgender,ASA,occupation,mininghistory,types ofoperation,smoking,alcoholconsumption,intraoperative additional drug use, postoperative additional problems accordingtothegroups.
Kruskal---WallisANOVA and Mann---WhitneyU tests were usedincomparisonsbetweenthegroupsintermsof contin-uousvariablessuchasdurationsofoperationandtourniquet, intraoperativebleeding,bloodamountsgiven,serumlevels ofSe,Cu,Zn,Fe,MDA,andGPx,andamountsoftramadol consumption. Friedman and Wilcoxon tests were used in comparison of these variables withpreoperative baseline valueswithinthegroups.
Analysisresultswereevaluatedwithinconfidence inter-valof95%,andp<0.05valueswereacceptedasstatistically significant.
Results
No significant differences were found in terms of demo-graphicdataandASAriskclassificationofthestudygroups (Table1).
Nosignificantdifferenceswerefoundbetweenthegroups in terms of types of operation and occupation (p>0.05), however,significantdifferencewasfoundintermsofhistory ofalcoholconsumption(p<0.05)(Table2).
Nosignificantdifferencewasfoundbetweenthegroups interms oftramadolconsumptionamountseither intraop-erativeorpostoperativeperiods(p>0.05)(Fig.1).Tramadol consumptionamounts.
Dataconcerningthedurationsofoperationsand tourni-quet application, intraoperative bleeding amounts, blood amounts given (as units), intraoperative additional drug use, and postoperative additionalproblems are shown on
Table 3. Tourniquet duration and intraoperative bleeding amounts of Group D were found tobe significantly lower thanGroupS(p<0.05).Durationsofoperationsand tourni-quetapplicationsandintraoperativebleedingamountswere foundtobesignificantlylowerinGroupDincomparisonto GroupP(p<0.05).Intraoperativebloodtransfusionwas per-formedjustinGroupS.Nosignificantdifferenceswerefound betweenthegroupsintermsotheothervariables(p>0.05). No significant difference was detected between the groupsintermsofSelevels(p>0.05)(Fig.2).Asignificant difference wasfound within the groups in terms of tem-poral changes in Se levels (p<0.05). T2 and T4 values in GroupS,andT3andT4valuesinGroupPwerefoundtobe
Table1 DemographicaldataandASAriskclassificationofthestudygroups.
GroupS(n=20) GroupD(n=20) GroupP(n=20) p
Gender(M/F) 16/4 13/7 11/9 0.241
Age(year) 41.8±12.2 39.4±14.2 41.0±17.7 0.845
Height(m) 1.7±0.1 1.7±0.1 1.7±0.1 0.753
Weight(kg) 71.9±11.1 77.1±12.1 75.7±11.0 0.180
BMI 24.7±2.9 26.1±3.3 25.6±3.6 0.236
ASA(I/II/III) 6/12/2 5/11/4 5/14/1 0.644
Table2 Typesofoperation,occupation,andhistoryofalcoholconsumptionandsmokingaccordingtothegroups.
GroupS(n=20) GroupD(n=20) GroupP(n=20) p
Occupationa(1/2/3/4/5/6) 3/9/3/1/2/2 4/5/3/1/0/7 1/9/3/0/0/7 0.337
Operationtypeb(1/2/3/4/5) 4/9/5/2/0 0/6/1/3/0/1 3/6/6/2/3 0.063
Smoking(+/−) 12/8 8/12 9/11 0.420
Alcohol(+/−) 1/19 0/20 5/15 0.020
+,yes;−,no.
a Occupationalgroupsrecordedas1---miners,2---self-employed,3---officer,4---smith,5---welder,6---unemployed.
b Typesofoperationsrecordedas1---footfracture,2---tibiafracture,3---kneemeniscopathy,4---anklefracture,5---kneeprosthesis.
0 50 100 150 200 250 300 350
T2 T3 T4
mg
Time
Group S
Group D
Group P
Figure1 Tramadolconsumption(mg).T2,postoperative0th; T3,postoperative24th;andT4postoperative48thhours
significantlylowerthanthebaselinevaluesmeasuredatT1 (p<0.05).
Culevelswerefoundtobesignificantlydifferentbetween the groups in each measurement time (p<0.05). Serum Cu levels were lower in Group D in comparison to the othergroupsineachmeasurement.Nodifferencewasfound withinthegroupsintermsoftemporalchangesinCulevels incomparisontothebaselinevalues(p>0.05)(Fig.3).
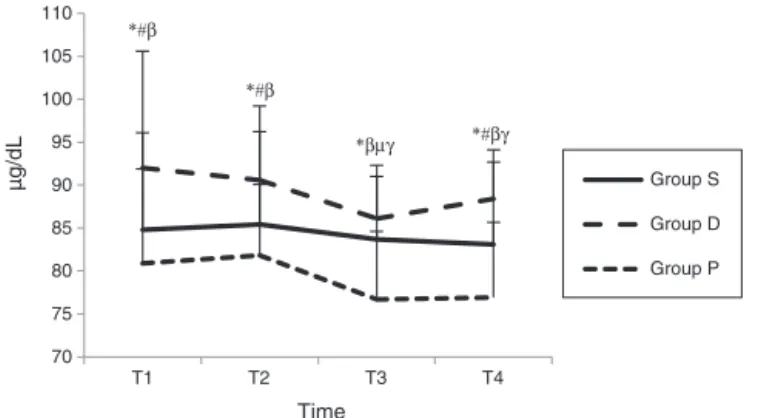
Significant differences were found betweenthe groups intermsofZnlevelsineachmeasurementtime(p>0.05). Serum Zn levels were found to be significantly higher in GroupDincomparisontoGroupSatT1,T2,andT4times, andincomparisontoGroupPatT1,T2,T3,andT4times (p<0.05). When the temporal changes in Zn levels were assessed, T3 value in Group D, and T3 and T4 values in GroupPwerefoundtosignificantlylowerincomparisonto thebaselinevaluesmeasuredatT1time(p<0.05)(Fig.4).
70 80 90 100 110 120 130 140
T1 T2 T3 T4
µg/L
Time
Group S
Group D
Group P
* *#
#
Figure2 SerumSelevels(g/L).*p<0.05T2andT4values comparedwithT1basalvaluesinGroupS;#p<0.05T3andT4 valuescompared with T1 basal valuesin Group P;T1, basal values;T2,postoperative0th;T3,postoperative24th;andT4, postoperative48thhours.
70 80 90 100 110 120 130 140
T1 T2 T3 T4
µg/dL
Time
Group S
Group D
Group P * # * #
*#
*#
Figure 3 Serum Cu levels (g/dL). *p<0.05 comparison acrossgroups; #p<0.05Group S andGroup Pcompared with GroupD;T1,basalvalues;T2,postoperative0th;T3, postop-erative24th;andT4,postoperative48thhours.
Table3 Distributionofdurationsofoperationsandtourniquetapplicationsandintraoperativebleeding,bloodamountsgiven,
intraoperativeadditionaldruguse,postoperativeadditionalproblems(mean±SD).
GroupS(n=20) GroupD(n=20) GroupP(n=20) p
Operationduration(min) 137.7±67.3 102.7±34.6 160.5±62.0a 0.005
Tourniquetduration(min) 88.4±21.6a 77.2±22.3 101.0±21.7a 0.004
Intraoperativebleeding(mL) 163.5±245.2a 52.5±51.5 168.0±107.6a 0.000
Bloodamountsgiven(unit) 0.2±0.5 0.0±0.0 0.0±0.0 0.045 Additionaldruguseb(1/2/3/4) 19/1/0/0 15/0/4/1 14/2/2/2 0.181
Postoperativeadditionalproblem(no/bronchospasm) 20/0 18/2 20/0 0.126
a p<0.05:whencomparedwithGroupD.
b Additionaldruguserecordedas1---none,2---pheniraminemaleate+dexamethasone,3---methylprednisolone+ranitidine,4---glyceryl
70 75 80 85 90 95 100 105 110
T1 T2 T3 T4
µg/dL
Time
Group S
Group D
Group P *#β
*#β
*#βγ *βµγ
Figure4 SerumZnlevels(g/dL).*p<0.05comparisonacross groups; #p<0.05 Group S compared with Group D; ˇp<0.05
GroupPcomparedwithGroupD;p<0.05T3valuescompared
withT1 basal valuesinGroup D; p<0.05T3 and T4 values
comparedwithT1basalvaluesinGroupP;T1,basalvalues;T2, postoperative0th;T3,postoperative24th;andT4, postopera-tive48thhours.
Nosignificantdifferencewasfoundbetweenthegroups intermsofFelevels(p>0.05).Whenthetemporalchanges inFelevelswithinthegroupswereassessed,T3andT4Fe levelswerefoundtobesignificantlylowerthanthebaseline valuesmeasuredatT1time(p<0.05)(Fig.5).
Asignificantdifferencewasobservedbetweenthegroups in the value measured at T2 timein terms of GPx levels (p<0.05).SerumGPxlevelmeasuredatT2timewasfound tobesignificantlyhigherinGroupSincomparisontoGroup P(p<0.05).WhenthetemporalchangesinGPxlevelswere assessedwithinthegroups, T4valuesbothin GroupSand GroupPwerefoundtobesignificantlyhigherthanthe base-line values measured at T1time (p<0.05). No significant differenceswerefoundwithinGroupDintermsoftemporal changesatanytimes(Fig.6).
Significantdifferenceswerefoundateachmeasurement timebetweenthegroupsintermsofMDAvalues(p<0.05). MDAvalueswerehigherinGroupSincomparisontoGroup DatT1,andin comparisontoGroup Pat T1,T2,T3,and T4times(p<0.05).WhenthetemporalchangesinMDA lev-elswereassessedwithinthegroups,T4valueswerefound tobesignificantly lowerin Group S and Group Pat T4in
20 40 60 80 100 120 140
T1 T2 T3 T4
µg/dL
Time
Group S
Group D
Group P *
*
Figure5 SerumFelevels(g/dL).*p<0.05allgroupsT3and T4levelscomparedwithinitselfwithT1basalvalues;T1,basal values;T2,postoperative0th;T3,postoperative24th;andT4, postoperative48thhours.
70 90 110 130 150 170 190
T1 T2 T3 T4
U/L
Time
Group S β#
*βγ
Group D
Group P
Figure6 SerumGPxLevels(U/L).*p<0.05comparisonacross groups;p<0.05GroupPcomparedwithGroupS;#p<0.05T4 valuescomparedwithT1basalvaluesinGroupS;ˇp<0.05T2
andT4valuescomparedwithT1basalvaluesinGroup P;T1, basalvalues;T2,postoperative0th;T3,postoperative24th;and T4,postoperative48thhours.
0 0.5 1 1.5 2 2.5 3
T1 T2 T3 T4
µmol/L
Time
Group D Group S
Group P *β#
*β *β
*β
Figure 7 Serum MDA levels (mol/L).*p<0.05comparison acrossgroups;#p<0.05T4valuescomparedwithT1basalvalues inGroupSandGroupP;ˇp<0.05GroupPcomparedwithGroup
S;T1,basal values;T2,postoperative 0th; T3,postoperative 24th;andT4,postoperative48thhours.
comparisontothebaselinevaluesmeasuredatT1(p<0.05) (Fig.7).
Discussion
Inthepresentstudyconductedonthecaseswounderwent extremitysurgeryusingtourniquetundergeneral anesthe-sia, it was observed that both sevoflurane and propofol maintenancedecreased Se andMDA levels,andincreased GPx values, sevoflurane did not change Zn levels but propofoldecreased Znlevels,andthat implementationof desfluranedidnotcausechangesinZn,Se,MDA,andGPx levels.Besidesthis,allthesethreedifferentgeneral anes-thesiamaintenancesignificantlyincreasedserumFelevels incomparisontothebaselinevalues,anddidnotchangeCu levels.
Itwasreportedthatanestheticagentscouldantioxidant activityin ischemiareperfusiondamageduetotourniquet viapreventingofformationofhighlyreactiveoxygen radi-calsaswellastheyinhibitedleukocytefunctions.22---24
Allaouchicheetal.,11 compared the activities of
sevoflurane(2.5%)inpigsfordeterminationofeffectof gen-eralanesthesiaonoxidative condition.In theirstudy that theyevaluatedplasmaandalveolarconcentrationsofMDA, SOD and GPx during general anesthesia for 120min, they showedthatpropofolcausedincrease inGPxlevelseither inbronchoalveolarlavage(BAL)fluidor incirculation,and decrease inMDA levels.In contrast,they found that des-fluranecausedincreaseinMDAlevelsbothinBALfluidand in circulation,and decreasein GPxvalues.They reported no significant changes in both GPx and MDA levelseither inBAL fluidorincirculation inthegroupthat sevoflurane was administered. As a result, they concluded that des-flurane had a potential effectof increasingthe oxidative stress,propofolhadpositiveeffectsonantioxidantsystem viadecreasinglipidperoxidation,andthatsevofluranehad noeffectsonoxidativestressandantioxidantsystem.Inour study,generalanesthesiawithpropofolcausedincreasein GPxlevels,anddecreaseinMDA.Sevofluraneconcentration usedinthestudyofAllaouchicheetal.,11 was2.5%,andit
was2%inourstudy.Besidesthis,itiswellknownthatN2O itselfcouldincreaseoxidative stressviacausingformation of reactive oxygen species.25 In our study,we considered
thattheincreaseinGPxlevelsinthesevofluranegroupin comparisontothebaselinevaluesmighthavebeencaused bythedifferenceinconcentrationofsevofluraneused,and byuseofN2Oasthecarriergas.
In the previous reports, similar to the present study, it was reported that sevoflurane prevented myocardial dysfunctionandnecrosisinpost-myocardialischemia reper-fusion phase; it effected oxidative stress and antioxidant mechanisms positively by causing less lipid peroxida-tion in laparoscopic cholecystectomy; it protected the heart againstATPdepletion induced by ischemia,calcium currents,andoxidativestressviaproteinkinaseactivation, opening of mitochondrial K+ATPase channels, and forma-tion of reactive oxygen particles; it decreased adhesion of postischemic polymorphonuclear neutrophils; and that it had more antioxidant activity in comparison to spinal anesthesia.1,26---30
In the studies in which administrations of sevoflurane and desfluranein laparoscopic surgery werecompared,it wasshownthatdesfluraneincreasedoxidativestressmore, andthatitchangedantioxidantmechanismsnegatively.1,12
Besidesthis,it wasstatedthatthiseffectincreasedmore whendesfluraneandnitrogenmixwasused.12
It was shown that propofol had a supportive effect to antioxidantcapacity,andthatitinhibitedproductionoflipid peroxidase in theprevious studies.31---33 Antioxidant effect
ofpropofolwasattributedtoitschemicalsimilaritytothe otherknownantioxidantssuchasbutylhydroxytolueneand alpha-tocopherol.32,34,35Theseantioxidantsbindmembrane
phospholipids,andcapturefreeradicals,andsotheyshow antioxidantpropertiesbyinhibitingthetransmissionchain withmembranefattyacidmolecules.36
It wasreportedthatin thecaseswithkneeartroplasty thatischemiareperfusiondamagedevelopeddueto tourni-quet, propofol showed antioxidant effect by decreasing MDA levels below the baseline values after opening the tourniquet.37
Arnaoutoglouetal.,38 found thatMDAlevelsdecreased
incomparisontothebaselinevaluesinthepropofolgroup, andincreased ina smallamount in thesevoflurane group
30minaftertheopeningofthetourniquetintheirstudyin whichtheyresearchedtheeffectsofthegroupthey admin-istered6---10mgkg−1 propofolmaintenanceafterinduction of 3gkg−1 fentanyl+2---2.5gkg−1 propofol, and of the groupthattheyadministeredsevofluranein1.5---2% concen-trationunder66:33%N2O:O2carriergasmaintenanceafter induction of 3gkg−1 fentanyl+5mgkg−1 thiopental in ischemia---reperfusion damage due to tourniquet in knee surgery on MDA levels. MDA, in fact, is a lipid peroxida-tionindicatorthatmayincreaseinearlyperiods.OurMDA measurementswereperformedearlierincomparisontothe studyofArnoutoglou etal.,andN2O:O2 concentrationwe used was also less. We administered propofol to our all groupsforinduction.IncontrasttothestudyofArnaoutoglu etal.,weconsideredthatantioxidantactivityofsevoflurane mightbecausedbythesefactors.
It is considered that desflurane may cause less oxida-tivestress, and less antioxidant activity depending on its lessmetabolism.Inthestudyof Türkanetal.,39 thatthey
investigated oxidative conditions of sevoflurane and des-flurane in erythrocytes, they showed that desflurane had nooxidantor antioxidantactivitiesthough severalstudies reported that desflurane had local and systemic antioxi-dant activity.1,12,11,40,41 It wasstated that oxidative stress
developed by desflurane anesthesiain pig lungs couldbe relatedtoexcessiveincreaseinproinflammatorycytokines in macrophages.11 Ceylan et al.,42 found that desflurane
causedlipidperoxidationbydecreasingvitaminElevelsin thepatientsunderwentsurgeryunderdesflurane anesthe-sia.
It wasshown that free radicalsformed during ethanol metabolism in alcohol consumption caused increase in oxidative stress, and that they had negative effects on antioxidantcapacity.43,44Besides this,itisknownthatcell
damageand oxidative stress due to ischemia---reperfusion increase depending on the severity and duration of ischemia.45
Wardle et al.,46 reported that oxidative damage
increasedfollowingbloodtransfusioninprematureinfants. Itwasstated thatthe association between blood transfu-sion and MDA levels might be due to oxidative effect of excessfreeFeformedbydestructionoferythrocytes.47Free
ironcausestissuedamageviaformation ofhighlyreactive hydroxyl radicals fromH2O2 and superoxides with Fenton andHaber---Weissreactions.48Inourstudybloodtransfusion
wasnotperformedintwogroupsotherthanthesevoflurane group.
In the present study, when analysing the factors of the lack of oxidative stress in the desflurane group, we consideredthatitmighthavebeencausedbylackof alco-holconsumption,shorterdurationoftourniquetapplication incomparisontotheothergroups,andlackofuseofblood productsinthedesfluranegroup.
In the previous studies, it was shown that plasma MDA levels increased in smokers as an indicator of lipid peroxidation.49Inthepresentstudy,webelievethat
smok-inghadnoinfluenceontheresultsduetolackofdifference betweenthegroupsintermsofsmoking.
nutrition,andtakingoftraceelements(Se,Mn,Zn,Cu,Fe). Amongsttheantioxidantenzymes,Cu,Zn,andMnarefound inthestructureofSOD,andSeionisfoundinGPx.5,6
Selenium has numerous biological functions, and the most important one of these is antioxidant activity. This activitydependsonthepresenceofselenocysteininactivity inthioredoxins reductasesand GPxs.Therefore,activities of these enzymes decrease in cases that serum Se levels arelow.50,51 Intheirstudythattheyinvestigatedgenotoxic
effectsofrepeatingsevofluraneanesthesiainrabbitsusing Comettest, Kaymak etal.,52 reportedthat selenium
sup-portadministeredintoperitonhadprotective roleagainst DNAdamagecausedduetoanesthesia.
Itwasreportedthatchangesinthelevelsoftrace ele-mentscaused increase in negative effects of freeoxygen radicalsontheintegrityofthecellbydecreasingthe effi-ciencyofantioxidantdefensemechanism.Traceelements, particularlyZn,Cu,andFe,havesignificanteffectsonlipid peroxidation.53 Salonen et al.,54 showed that myocardial
infarctionriskwasfourtimesmoreinthehumanswithhigh plasmaCulevelsincomparisontothenormalpopulationasa resultofnegativeeffectsoflipidperoxidationonthevessel walls.
Zn,cofactor ofSODenzyme,playsanimportantrolein capturingoffreeoxygenradicals.InSODenzyme,Zncauses theenzymetokeepthestability,andCuisresponsiblefor theactivity of theenzyme.55---57 Znlevelsdecreased after
surgerymay reduce theactivity of the enzyme, andmay causeincreaseinserumCulevelsdependingonthis.58,59
Intheindividualswithcancer, itwasstatedthatserum Cu/Zn rate did not change in the early stages, but this rateincreasedsignificantlyintheadvancedstages.60Itwas
reportedthatanincreasedCu/Znrateeitherinthetissueor inserummightindicateanimpairedantioxidantdefense.57
Inthepresentstudy,whenthemeasurementsof48thhour werecomparedtothebaselinevalues,Culevelshavenot changed, and Zn levels decreased in the propofol group, and nodifferences were observed in the sevoflurane and thedesfluranegroupsintermsofCuandZn.
The most important feature of ironis its capability to befound in two-oxidation condition asferric andferrous forms.Ironinferricformisnon-functional.Mostoftheiron (75%)isfoundboundtohemproteinssuchashemoglobinand myoglobin.Therestisfoundinstorageproteinssuchas fer-ritinandhemosiderin,andincriticalenzymesystemssuch asCATinvolvedincytochromeandantioxidantsystems.61It
wasshown that increasedoxidative stressmight play role inthe pathogenesis of irondeficiency anemiathat better responses might have been provided by administrationof antioxidantvitaminstogetherwithironreplacement ther-apyinthepatientswithirondeficiencyanemia,andsothat earlierimprovementofthesymptomsrelatedtoiron defi-ciencyanemiacouldbeachieved.62Inourstudy,ironlevels
decreased in all threegroups in the postoperative period (p<0.05).
Türkanetal.,20foundthatantioxidantenzymeactivityof
erythrocyte(SOD,GPx)andtraceelementlevelsdecreased in the patients who were administered halothane, enflu-raneandisofluraneanesthesia.InanotherstudyofTürkan et al.,21 levels of SOD and GPx antioxidant enzymes and
cofactorsofthese,Se,Cu,andZn,wereshowntobelower intheindividualsexposedtoanestheticgaseschronicallyin
theoperationroomswithpassivewastesystemsin compar-isontothe staffofthe otherdepartmentsof thehospital who were notexposed to these gases. As a result of the mentioned study, it was reported that exposure to anes-theticgaseschronicallyhadinfluenceonantioxidantenzyme system.
Asa resultofevaluation oftheindicators suchasMDA andGPx,weconcludedthatgeneralanesthesiamaintenance usingpropofolactivatedantioxidantsystem against oxida-tive stress and decreased Se andZn levels due touse of antioxidantsystem; generalanesthesiamaintenanceusing sevofluraneactivatedantioxidantsystem againstoxidative stress and decreased Se levels due to use of antioxidant system; general anesthesia maintenance using desflurane had no impacts on oxidative stress and antioxidant sys-temandsodidnotcausechangesintraceelementlevels, however that each three methods decreased serum iron levels.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgements
ThisstudywassupportedbyBülentEcevitUniversity Scien-tificResearchesProjectsCoordinationUnit.
References
1.KöksalGM,SayilganC,AydinS,etal.Theeffectsof sevoflu-raneand desfluraneonlipidperoxidationduringlaparoscopic cholecystectomy.EurJAnaesthesiol.2004;21:217---20.
2.HalliwellB,BorishE,PryorWA,etal.Oxygenradicalsandhuman disease.AnnInternMed.1987;107:526---45.
3.Bostankolu E, Ayoglu H, Yurtlu S, et al. Dexmedetomi-dine did not reduce the effects of tourniquet-induced ischemia---reperfusion injury during general anesthesia. Kao-hsiungJMedSci.2013;29:75---81.
4.McCordJM.Theevolutionoffreeradicalsandoxidativestress. AmJMed.2000;108:652---9.
5.Rock CL, Jacob RA, Bowen PE. Update on the biological characteristicsof theantioxidant micronutrients:vitamin C, vitamin E, and the carotenoids. J Am Diet Assoc. 1996;96: 693---702.
6.SiesH,StahlW,SundquistAR.Antioxidantfunctionsofvitamins VitaminsEandC,beta-carotene,andothercarotenoids.AnnN YAcadSci.1992;669:7---20.
7.Mathru M, Dries DJ, Barnes L, et al. Tourniquet-induced exsanguination in patients requiring lower limb surgery. An ischemia---reperfusion model of oxidant and antioxidant metabolism.Anesthesiology.1996;84:14---22.
8.FriendlHP,TillGO, TrentzO, et al.Role ofoxygen radicals in tourniquet-related ischemia---reperfusion injury of human patients.KlinWochenschr.1991;69:1109---12.
9.Sarıcao˘glu F, Dal D, Salman AE, et al. Effects of low-dose n-acetyl-cysteine infusion on tourniquet-induced ischaemia---reperfusion injury in arthroscopic knee surgery. ActaAnaesthesiolScand.2005;49:847---51.
11.AllaouchicheB,DebonR, GoudableJ,etal.Oxidativestress statusduringexposuretopropofol,sevofluraneanddesflurane. AnesthAnalg.2001;93:981---5.
12.SivaciR,Kahraman A,SerteserM,etal.Cytotoxiceffects of volatileanestheticswithfreeradicalsundergoinglaparascopic surgery.ClinBiochem.2006;39:293---8.
13.DurakI,OzturkHS,DikmenB,etal.Isofluraneimpairs antiox-idant defence system in guinea pig kidney. Can J Anaesth. 1999;46:797---802.
14.Kotani N, Takahashi S, Sesler DI, et al. Volatile anesthetics augmentexpressionofproinflammatorycytokinesinrat alveo-larmacrophagesduringmechanicalventilation.Anesthesiology. 1999;91:187---97.
15.Kotani N, Hashimoto H, Sesler DI, et al. Expression of genesforproinflammatorycytokinesinalveolarmacrophages during propofol and isoflurane anesthesia. Anesth Analg. 1999;89:1250---6.
16.Aarts L, Van Der Hee R, Dekker I, et al. The widely used anestheticagentpropofolcanreplacealpha-tocopherolasan antioxidant.FEBSLett.1995;357:83---5.
17.DeLaCruzJP,Sede˜noG,CarmonaJA,etal.Invitroeffectsof propofolontissularoxidativestressintherat.AnesthAnalg. 1998;87:1141---6.
18.DeLaCruzJP,VillalobosMA,Sede˜noG,etal.Effectofpropofol onoxidativestressinaninvitromodelofanoxia-reoxygenation intheratbrain.BrainRes.1998;800:136---44.
19.Ya˘gmurdur H, Cakan T, Bayrak A, et al. The effects of etomidate, thiopental, and propofol in induction on hypoperfusion---reperfusion phenomenon during laparo-scopic cholecystectomy. Acta Anaesthesiol Scand. 2004;48: 772---7.
20.Türkan H, Bukan N, Sayal A, et al. Effects of halothane, enflurane,and isoflurane onplasmaand erythrocyte antiox-idant enzymes and trace elements. Biol Trace Elem Res. 2004;102:105---12.
21.TürkanH,AydinA, SayalA. Effectofvolatile anestheticson oxidativestress dueto occupationalexposure.WorldJSurg. 2005;29:540---2.
22.Sarıcao˘glu F, Dal D, Salman AE, et al. Ketamin seda-tion during spinal anesthesia for arthroscopic knee surgery reduced the ischemia---reperfusion injury markers. Anesth Analg.2005;101:904---9.
23.TuranR,YagmurdurH,KavutcuM,etal.Propofoland tourni-quetinducedischemiareperfusioninjuryinnlowerextremity operations.EurJAnaesthesiol.2007;24:185---9.
24.KahramanS,Kılınc¸K,DalD,etal.Propofolattenuatesformation oflipidperoxidesintourniquet-inducedischemia---reperfusion injury.BrJAnaesth.1997;78:279---81.
25.Wro´nska-NoferT,NoferJR,JajteJ,etal.OxidativeDNA dam-ageandoxidativestressinsubjectsoccupationallyexposedto nitrousoxide(N(2)O).MutatRes.2012;731:58---63.
26.Kato R, Foex P. Myocardial protection byanesthetic agents againstischemia---reperfusioninjury.Anupdatefor anesthesi-ologists.CanJAnaesth.2002;49:777---91.
27.Zaugg M, Lucchinetti E, Uecker M, et al. Anaesthetics and cardiacpreconditioning.PartI.Signallingand cytoprotective mechanisms.BrJAnaesth.2003;91:551---65.
28.deRuijterW,MusterRJ,Boer C,et al.Thecardioprotective effectsofsevofluranedependsonproteinkinaseCactivation, openingofmitochondrialK(+)(ATP)channels,andthe produc-tionofreactiveoxygenspecies.AnesthAnalg.2003;97:1370---6.
29.Heindle B, Reichle FM, Zahler S, et al. Sevoflurane and isofluraneprotectthereperfusedguinea pigheartby reduc-ingpostischemicadhesionof polymorphonuclearneutrophils. Anaesthesiology.1999;91:521---30.
30.IzdesS,Sepici-DincelA,GozdemirM,etal.Theeffectof gen-eralandregionalanaesthesiaonischemia---reperfusioninjury. AnaesthIntensiveCare.2007;35:451---2.
31.DeLaCruzJP,ZancaA,CarmonaJA,etal.Theeffectofpropofol onoxidativestressinplateletsfromsurgicalpatients.Anesth Analg.1999;89:1050---5.
32.TsuchiyaM,AsadaA,KasaharaE,etal.Antioxidantprotection ofpropofolanditsrecyclinginerythrocytemembranes.AmJ RespirCritCareMed.2002;165:54---60.
33.Basu S, MutschlerDK,LarssonAO, et al. Propofol (Diprivan-EDTA) counteracts oxidative injury and deterioratian of the arterial oxygen tension during experimental septic shock. Resuscitation.2001;50:341---8.
34.Murphy PG, Myers DS, Davies MJ, et al. The antioxidant potential of propofol (2,6-diisopropylphenol). Br J Anaesth. 1992;68:613---8.
35.ErikssonO,PolleselloP,SarisNE.Inhibitionoflipid peroxida-tioninisolatedratlivermitochondriabythegeneralanesthetic propofol.BiochemPharmacol.1992;44:391---3.
36.Halliwell B. Reactive oxygen species in living system: source, biochemistryand rolein humandisease. Am JMed. 1991;91:14---22.
37.Aldemir O, C¸elebi H, Cevik C, et al. The effects of propo-fol or halothane onfree radical productionaftertourniquet inducedischemia---reperfusioninjuryduringkneearthroplasty. ActaAnaesthesiolScand.2001;45:1221---5.
38.Arnaoutoglou H, Vretzakis G, SouliolisD, et al. The effects of propofol or sevoflurane on free radical production after tourniquet induced ischemia---reperfusion injury during knee arthroplasty.ActaAnaesthesiolBelg.2007;58:3---6.
39.TürkanH, AydinA, SayalA, et al.Effect ofsevoflurane and desfluraneonmarkersofoxidativestatusinerythrocyte.Toxicol IndHealth.2011;27:181---6.
40.Sedlic F, Pravdic D, Ljubkovic M, et al. Differences in production of reactive oxygen species and mitochondrial uncouplingaseventsinthepreconditioningsignalingcascade betweendesfluraneandsevoflurane.AnesthAnalg.2009;109: 405---11.
41.TürkanH,AydinA,SayalA,etal.Oxidativeandantioxidative effectsofdesfluraneandsevofluraneonrattissueinvivo.Arh HigRadaToxicol.2011;62:113---9.
42.CeylanBG,Nazıro˘gluM,U˘guzAC,etal.EffectsofvitaminC andEcombinationonelementandoxidativestresslevelsinthe bloodofoperativepatientsunderdesfluraneanesthesia.Biol TraceElemRes.2011;141:16---25.
43.PengFC,TangSH,HuangMC,etal.Oxidativestatusinpatients withalcoholdependence:aclinicalstudyinTaiwan.JToxicol EnvironHealthA.2005;68:1497---509.
44.ClotP,TaboneM,AricoS,etal.Monitoringoxidativedamagein patientswithlivercirrhosisanddifferentdailyalcoholintake. Gut.1994;35:1637---43.
45.Cuzzocrea S, Riley DP, Caputi AP, et al. Antioxidant ther-apy:anewpharmacologicalapproachinshock,inflammation, and ischemia/reperfusion injury. Pharmacol Rev. 2001;53: 135---59.
46.WardleSP,DruryJ,GarrR,etal.Effect ofbloodtransfusion onlipidperoxidationinpreterminfants.ArchDisChildFetal NeonatalEd.2002;86:46---8.
47.HiranoK,MorinobuT,KimH,etal.Bloodtransfusionincreases freeradicalpromotingnon-transferrinboundironinpreterm infants.ArchDisChild.2001;84:188---93.
48.MateosF,BrockJH,Perez-ArtellanoJL.Ironmetabolisminthe lowerrespiratorytract.Thorax.1998;53:574---600.
49.Nadiger HA, Mathew CA, Sadasivudu B. Serum malondialde-hyde (TBA reactive substance) levels in cigarette smokers. Atherosclerosis.1987;64:71---3.
50.Holben DH, Smith AM. The diverse role of selenium within selenoproteins;areview.JAmDietAssoc.1999;99:836---43.
52.KaymakC,KadiogluE,BasarH,etal.Genoprotectiveroleof vitaminEandseleniuminrabbitsanaesthetizedwith sevoflu-rane.HumExpToxicol.2004;23:413---9.
53.HalliwellB, GutteridgeJM.Oxygentoxicity, oxygenradicals, transitionmetalsanddisease.BiochemJ.1984;219:1---14.
54.SalonenJT,SalonenR,KorpelaH,etal.Serumcopperandthe riskofacutemyocardialinfarction:aprospectivestudyinmen ineasternFinland.AmJEpidemiol.1991;134:268---76.
55.KhaledS,BrunJF,MicallelJP,etal.Serumzincandblood rhe-ologyinsportsmen.ClinHemorheolMicrocirc.1997;17:47---58.
56.MocchegianiE,MalavoltaM,MutiE,etal.Zinc,metallothioneins andlongevity:interrelationshipswithniacinandselenium.Curr PharmDes.2008;14:2719---32.
57.Richardson J, Thomas KA, Rubin BH, et al. Crystal struc-tureofbovineCu,Znsuperoxidedismutaseat3Aresolution:
chain tracing and metal ligands. Proc Natl Acad Sci USA. 1975;72:1349---53.
58.BrounA,DugdillS,WyattM,etal.Serumtotalantioxidantstatus duringvascularsurgery.BiochemSocTrans.1998;26:127.
59.LasesEC,Duurkens VA,GerritsenWB, etal.Oxidativestress afterlungresectiontherapy.Chest.2000;117:999---1003.
60.MaEL,JiangZM.Ion-exchangechromatographyinsimultaneous determinationofserum,copperandzinclevelsinpatientswith cancerofdigestivetract.ChimMedJ(Engl).1993;106:118---21.
61.BeardJL,DawsonH,PineroDJ.Ironmetabolism:a comprehen-sivereview.NutrRev.1996;54:295---317.