RevBrasAnestesiol.2017;67(5):548---551
REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
PublicaçãoOficialdaSociedadeBrasileiradeAnestesiologiawww.sba.com.br
CLINICAL
INFORMATION
Sudden
motor
and
sensorial
loss
due
to
retroperitoneal
hematoma
during
postoperative
periods:
a
case
report
夽
Pelin
S
¸en,
Havva
Gül
Gültekin, ˙Ismail
Caymaz,
Ömer
Özel,
Ayda
Türköz
∗BaskentUniversity,IstanbulTrainingandMedicalResearchCenter,DepartmentofAnesthesiology,Istanbul,Turkey
Received28November2015;accepted10February2016
Availableonline30April2016
KEYWORDS
Epiduralanesthesia; Flaccidparalysis; Retroperitoneal hematoma
Abstract A68year-oldmalepatientwashospitalizedforradicalprostatectomy.Hehadno
abnormalmedicalhistoryincludingneurologicaldeficitbeforetheoperation.Priortogeneral anesthesia,anepidural catheterwas insertedintheL3---4 interspacefor intraoperativeand postoperativeanalgesia.Aftersurgeryforninehours,hedevelopedconfusionandflaccid paral-ysisofbilaterallowerextremitiesoccurred.Nopathologywasdetectedfromcranialcomputed tomography anddiffusionmagnetic resonanceimaging nopathologywas detected.His tho-racic/lumbarmagneticresonanceimaging.Intraabdominalpressurewasshowntobe25mmHg, andabdominalultrasonographyrevealedprogressionintheinflammation/edema/hematomain theperirenalregion.TheBromagescorewasbackto1intherightfootonthe24thhourandin theleftfootonthe26thhour.Paraplegiadevelopedinpatientsafterepiduralinfusionmightbe causedbypotentiatedlocalanestheticeffectduetoretroperitonealhematomaand/orelevated intra-abdominalpressure.
©2016SociedadeBrasileiradeAnestesiologia.PublishedbyElsevierEditoraLtda.Thisisan openaccessarticleundertheCCBY-NC-NDlicense( http://creativecommons.org/licenses/by-nc-nd/4.0/).
PALAVRAS-CHAVE
Anestesiaperidural; Paralisiaflácida; Hematoma retroperitonial
Súbitaperdasensitivaemotoradevidoahematomaretroperitonealduranteos períodosdepós-operatório:relatodecaso
Resumo Pacientedosexomasculino, 68 anosdeidade,hospitalizado paraprostatectomia
radical. O paciente não tinha história médica anormal, inclusive nem déficit neurológico antes da operac¸ão. Antes da anestesia geral, um cateter peridural foi inserido no espac¸o intermédio L3-4 para analgesia nointra e pós-operatório. Após a cirurgia que durou nove
夽 ThestudywasconductedintheDepartmentofAnesthesiology,BaskentUniversityIstanbulTrainingandMedicalResearchCenter,Istanbul,
Turkey.ThestudywaspresentedintheTurkishSocietyofAnesthesiologyandReanimation48thNationalCongressheldonOctober25---29, 2014.PatientIdentification:Patientconsentwasobtainedfromthepatient.
∗Correspondingauthor.
E-mail:[email protected](A.Türköz).
http://dx.doi.org/10.1016/j.bjane.2016.02.006
Retroperitonealhematomamimicsepiduralanesthesiacomplications 549
horas,opaciente desenvolveuconfusãoeparalisiaflácidabilateraldosmembrosinferiores. Tomografia computadorizadadecrânio eimagemdedifusãoporressonância magnéticanão detectaram lesão.Osachadosnasimagensde ressonânciamagnéticatorácica/lombareram normais.Apressãointra-abdominalerade25mmHgeoultrassomabdominalrevelouprogressão deinflamac¸ão/edema/hematomanaregiãoperirrenal.OescoredeBromagevoltoua1nopé direito na24a horaenopé esquerdona26a hora.A paraplegiadesenvolvida nospacientes
apósainfusãoepiduralpodetersidocausadaporumefeitopotencializadodoanestésicolocal devidoahematomaretroperitoneale/oupressãointra-abdominalelevada.
©2016SociedadeBrasileiradeAnestesiologia.PublicadoporElsevierEditoraLtda.Este ´eum artigo OpenAccess sobumalicenc¸aCCBY-NC-ND( http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
The rate of neurological complications following regional anesthesiais 4/10,000.1 Neurological complications result
fromfactorssuchasdirectnerveinjuryrelatedtoneedleor catheterplacement,drug-relatedneurotoxicity,local anes-theticinjectionintothenerve,neuralischemia.2---5Different
from the common causes of neurological complications, we herein presented development of paraplegia due to retroperitoneal hematoma in a patient who underwent surgeryforprostatecancer.
Case
report
A 68 year-old male patient was hospitalized for radical prostatectomy with the pre-diagnosis of prostate cancer, whichwasconsideredbasedonthetransurethralresection biopsy performed due to asymptomatic prostate-specific antigen elevation. He underwent surgery with the Amer-ican Society of Anesthesiologists (ASA) risk score of 1. Acetylsalicylic acid(150mg.day−1), which thepatient has been receiving, was discontinued 7 days before surgery. He was monitored at the operating room in accordance with ASA standards; an intravenous route was opened and fluid replacement was started. After cutaneous and subcutaneousinfiltrationoflocalanesthesiaperformedinto theL3---L4 intervertebralspaceusing 2mL of2% lidocaine solution with the patient in the sitting position, an 18-G epiduralcatheterwasinsertedbyloss-of-resistancemethod in one sitting. After negative aspiration and test dose, 7mL of 0.5% bupivacaine was administered through the epiduralcatheter. Fifteen minuteslater, general anesthe-sia was performed in the patient, in whom the level of sensory blockade was at T8. The patient, of whom pre-inductionbloodpressurewas130×70mmHg,pulseratewas
84beats/min,andperipheraloxygensaturation(SpO2)was 100%,waspreoxygenatedandgeneralanesthesiainduction wasperformedwith200mgpropofoland40mgrocuronium. Theanesthesiawasmaintainedwith0.8---0.6%isofluranein oxygen-airmixture(50/50%).Ninetyminutesafterepidural bolus dose, 0.25% bupivacaine was administered through the epidural catheter at an infusion rate of 5mL.h−1. During the intraoperative period, 2 units of erythrocyte suspension,500mLofcolloid,and4500mLcrystalloidwere
administered.Thesurgical procedure lastedfora totalof 3h.Atotalof37.5mgbupivacaineinfusionwasperformed. The patient woke up without any problem at the end of surgery. Total amounts of urine and blood loss over the course of surgery were 800mL and 700mL, respectively. He was kept in the postoperative recovery room for an hour.Duringtransfertotheclinic,hishemoglobinlevelwas 10g.dL−1 and hematocrit level was 28.8%. In the postop-erativemonitoringroom,thepatienthadabloodpressure of123×60mmHg,SpO2of99%,pulserateof56beats/min,
Visual AnalogueScale (VAS) score of 0,and Aldretescore of 10. His motor examination was normal (Bromage score1).
Afterthesurgery,thepatientwasmonitoredintheclinic usingthe patient-controlledanalgesiaform.Postoperative analgesia was performed with 0.1% bupivacaine adminis-teredthroughtheepiduralcatheteratarateof5mL.h−1. Aftersurgeryfor 2ndhour,when hisVASscorewas6,the infusion rate was increased to 8mL.h−1. The blood pres-surewasabout100×60mmHgandthepulseratewasabout
80beats/min.On the postoperative6th hour,the infusion ratewasdecreasedto3mL.h−1sincehismotorexamination wasnormal(Bromagescore1)andVASscorewas0.
After surgery for 9th hour, an emergency code was called since he developed confusion and motor loss. When the emergency team arrived, the physical exami-nation of the patient revealed confusion, agitation, and meaninglessspeech.Hisblood pressurewas78×40mmHg.
550 P.S¸enetal.
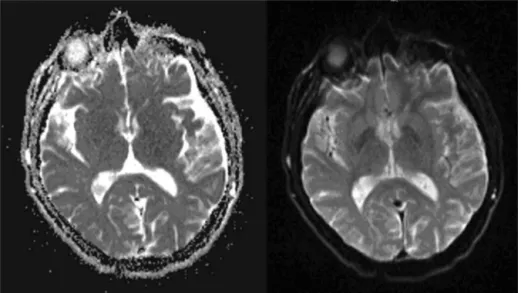
Figure1 Cranialcomputedtomographyanddiffusionmagneticresonanceimaging.
Figure2 Thoracic/lumbarmagneticresonanceimaging.
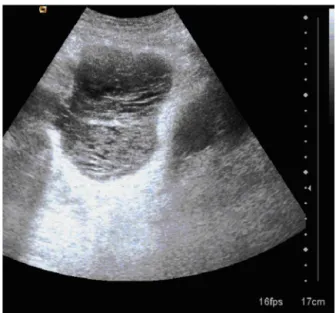
patient underwent emergency ultrasonography (US). The abdominalUSrevealedincreaseddensitythatmightreflect massiveinflammation,edemaorbleedinginbilateral perire-nalregionsintheretroperitoneumandhematomabeneath the bladder (Fig. 3). The Bromage score was return to1 inthe right footonthe 24thhour andin theleftfoot on the26thhour.Abdominaldistensionofthepatientincreased andnogas-stooldischargewasobservedonthe postopera-tive3rdday.Creatininelevelincreasedto2.3mg.dL−1from 0.9mg.dL−1andbloodureanitrogen(BUN)levelincreased to70mg.dL−1from23mg.dL−1.PlaneabdominalX-ray per-formed in the standing position onthe postoperative 4th daywasnormal.AbdominalUSGrevealedprogressioninthe inflammation/edema/hematoma in the perirenal region. Treatment was started for pyelonephritis; antibiotherapy was arranged. His body temperature did not decrease on the postoperative 6th day monitoring and elevation of BUN-creatinine concentrations persisted incrementally.
Renalscintigraphyperformedonthepostoperative7thday revealedbilateralleakagefrombothrenalcalyces.Bilateral nephrostomytubeswereplacedbytheDepartmentof Inter-ventionalRadiologyandhematomabeneaththebladderwas aspirated. On the postoperative 8th day, BUN/creatinine concentrations decreased to 15/1.3mg.dL−1. As the con-trastsubstancepassagedisappearedduringthefollow-ups, nephrostomy tubes were removed. The patient was dis-chargedfromthehospitalonthepostoperative14thday.
Discussion
Retroperitonealhematomamimicsepiduralanesthesiacomplications 551
Figure3 TheabdominalUSG.
thought likelydevelopment of epidural hematoma at the time of event or, secondly, of drug toxicity; because, clinically, both sudden motor loss and alteration in con-scious developed concurrently. Postoperative paraplegia mayresultfromspinalhematoma,intracordinjection,drug toxicity,orcompressionorimpairedperfusiondueto epidu-ral air.6---9 In addition, surgery-related decrease in spinal
cord perfusion,10,11 preexisting spinal metastasis,7,12
tho-racicdischerniation,13andtemporaryanteriorspinalartery
syndrome14mayalsocauseparaplegia.Inthepresentcase,
since the diagnosis could not be established via cranial computed tomography performed for early diagnosis, we eliminatedthepre-diagnosisofepiduralvascular compres-sion/ischemiadepending onthe thoracicand lumbar MRI, whichwereperformedtoruleoutischemiaandhematoma. We then considered systemictoxicity dueto drug tox-icity.Systemictoxicityoflocalanesthetics wasunlikelyto causeparaplegia becauseepiduralinfusionwasdecreased atleast10hbeforeparaplegiawasfound.Furthermore,the centralnervesymptomssuchasconfusionwerecausedby hypotensionduetopostoperativehemorrhage.
Thediagnosiswasestablishedafterintraabdominal pres-sure was measured 25mmHg via a urinary catheter and ultrasoundrevealedretroperitoneumhematoma.Wethink that same of pregnancy evidence supporting the mecha-nism.Increasedintraabdominalpressure duringpregnancy increases blood volume in the epidural venous plexus by compressingtheinferiorvenacava,decreasescerebrospinal fluidvolume,decreasesepiduralvolume,increases epidu-ralpressure, andtherebydecreasestheneed for epidural doseby30%.15 Wethoughtthatretroperitonealhematoma
occurred in the present case after radical prostatec-tomy caused sensorial/motor blockade by increasing the intraabdominalpressureandbyincreasingbloodvolumein
the epidural venous plexus, decreasing epidural volume, increasing epidural pressure, and thereby decreasing the needforepiduraldose.
In the present case report, it was demonstrated that paraplegia developed in patients after epidural infu-sion might be caused by potentiated local anesthetic effectdue to retroperitoneal hematoma and/or elevated intra-abdominalpressure. Andearly interventionprevents developmentofirreversibleneurologicaldamage.
Conflicts
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.Ortiz de laTabla GonzálezR, Martínez Navas A. Neurologic complicationsofcentralneuraxialblocks.RevEspAnestesiol Reanim.2011;58:434---43.
2.ReynoldsF.Damage to theconus medullarisfollowing spinal anaesthesia.Anaesthesia.2001;56:238---47.
3.AuroyY,NarchiP,MessiahA,etal.Seriouscomplicationsrelated toregionalanesthesia:resultsofaprospectivesurveyinFrance. Anesthesiology.1997;87:479---86.
4.Myers RR, Heckman HM. Effects of local anesthesia on nerve blood flow: studies using lidocaine with and without epinephrine.Anesthesiology.1989;71:757---62.
5.RiglerML,DrasnerK,KrejcieTC,etal.Caudaequinasyndrome after continuous spinal anesthesia. Anesth Analg. 1991;72: 275---81.
6.TrybaM.Epiduralregionalanesthesiaandlowmolecular hep-arin: Pro. Anasthesiol Intensivmed Notfallmed Schmerzther. 1993;28:179---81.
7.deMedicisE,deLeon-CasasolaOA.Reversibleparaplegia asso-ciatedwithlumbarepiduralanalgesiaand thoracicvertebral metastasis.AnesthAnalg.2001;92:1316---8.
8.Moen V, Dahlgren N, Irestedt L. Severe neurological complications after central neuraxial blockades in Sweden 1990---1999.Anesthesiology.2004;101:950---9.
9.MayallMF,CalderI.Spinalcordinjuryfollowinganattempted thoracicepidural.Anaesthesia.1999;54:990---4.
10.ShortHD.Paraplegiaassociatedwiththeuseofoxidized cellu-loseinposterolateralthoracotomyincisions.AnnThoracSurg. 1990;50:288---9.
11.Mato M, Perez A, Otero J, et al. Paraplegia after left tho-racotomyina patientcarryinganepidural catheter.RevEsp AnestesiolReanim.2001;48:89---92.
12.HirlekarG.Paraplegiaafterepiduralanalgesiaassociatedwith anextraduralspinaltumor.Anaesthesia.1980;35:363---4.
13.MatsuuraJA,MakhoulRG,PosnerMP,etal.Intraduralherniation ofathoracicdisccausingparaplegiacoincidentwithepidural anesthesia.AnesthAnalg.1997;84:922---3.
14.CrystalZ,KatzY. Postoperativeepiduralanalgesiaand possi-bletransient anterior spinal arterysyndrome.Pain Practice. 2001;1:372---3.