www.jped.com.br
ORIGINAL
ARTICLE
Impact
and
seasonality
of
human
rhinovirus
infection
in
hospitalized
patients
for
two
consecutive
years
夽
Jaqueline
Leotte
a,
Hygor
Trombetta
a,
Heloisa
Z.
Faggion
a,
Bernardo
M.
Almeida
b,
Meri
B.
Nogueira
c,
Luine
R.
Vidal
c,
Sonia
M.
Raboni
a,c,∗aUniversidadeFederaldoParaná(UFPR),HospitaldeClínicas,DivisãodeDoenc¸asInfecciosas,Curitiba,PR,Brazil bUniversidadeFederaldoParaná(UFPR),HospitaldeClínicas,DivisãodeEpidemiologiaHospitalar,Curitiba,PR,Brazil cUniversidadeFederaldoParaná(UFPR),HospitaldeClínicas,LaboratóriodeVirologia,Curitiba,PR,Brazil
Received27June2016;accepted29July2016 Availableonline2December2016
KEYWORDS
Humanrhinovirus; Acuterespiratory infections; Respiratoryvirus
Abstract
Objectives: Toreportepidemiologicalfeatures,clinicalcharacteristics,andoutcomesofhuman rhinovirus(HRV)infectionsincomparisonwithothercommunityacquiredrespiratoryvirus(CRV) infectionsinpatientshospitalizedfortwoconsecutiveyears.
Methods: Thiswasacross-sectional study.Clinical,epidemiological,andlaboratorydataof patientshospitalizedwithacuterespiratorysyndromeinatertiarycarehospitalfrom2012to 2013werereviewed.
Results: HRVwasthemostcommonCRVobserved(36%,162/444)andwaspresentinthe major-ityofviralco-detections(69%,88/128),mainlyinassociationwithhumanenterovirus(45%). MostHRV-infectedpatientswereyoungerthan2years(57%).Overall,patientsinfectedwithHRV hadalowerfrequencyofsevereacuterespiratoryinfectionthanthoseinfectedwithotherCRVs (60%and84%,respectively,p=0.006),buthadmorecomorbidities(40%and27%,respectively;
p=0.043).However,intheadjustedanalysisthisassociationwasnotsignificant.Themortality ratewithintheHRVgroupwas3%.DetectionofHRVwasmoreprevalentduringautumnand win-ter,withamoderatelynegativecorrelationbetweenviralinfectionfrequencyandtemperature (r=−0.636,p<0.001)butnocorrelationwithrainfall(r=−0.036,p=0.866).
夽
Pleasecitethisarticleas:LeotteJ,TrombettaH,FaggionHZ,AlmeidaBM,NogueiraMB,VidalLR,etal.Impactandseasonalityofhuman
rhinovirusinfectioninhospitalizedpatientsfortwoconsecutiveyears.JPediatr(RioJ).2017;93:294---300.
∗Correspondingauthor.
E-mail:[email protected](S.M.Raboni). http://dx.doi.org/10.1016/j.jped.2016.07.004
Conclusion: HRVisusuallydetectedinhospitalizedchildrenwithrespiratoryinfectionsandis oftenpresentinviralco-detections.ComorbiditiesarecloselyassociatedwithHRVinfections. Theseinfectionsshowseasonalvariation,withpredominanceduringcolderseasons.
©2016PublishedbyElsevierEditoraLtda.onbehalfofSociedadeBrasileiradePediatria.Thisis anopenaccessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/licenses/ by-nc-nd/4.0/).
PALAVRAS-CHAVE
Rinovírushumano; Infecc¸ões
respiratóriasagudas; Vírusrespiratório
Impactoesazonalidadedainfecc¸ãoporrinovírushumanoempacientesinternados pordoisanosconsecutivos
Resumo
Objetivos: Relatarascaracterísticasepidemiológicas,ascaracterísticasclínicaseosresultados dasinfecc¸õesporrinovírushumano(RVH)emcomparac¸ãoaoutrasinfecc¸õesporvírus respi-ratóriosadquiridosnacomunidade(VRCs)empacientesinternadospordoisanosconsecutivos.
Métodos: Estefoiumestudotransversal.Foramrevisadososdadosclínicos,epidemiológicose laboratoriaisdepacientesinternadoscomsíndromerespiratóriaagudaemumhospitalterciário de2012a2013.
Resultados: ORVHfoi o VRC mais comum observado (36%, 162/444) e esteve presente na maiorpartedascodetecc¸õesvirais(69%,88/128),principalmenteemassociac¸ãoaoenterovírus humano(45%).AmaioriadospacientesinfectadosporRVHpossuíamenosde2anos(57%).De modo geral, ospacientes comRVHapresentaram umamenor frequência deinfecc¸ão respi-ratóriaagudagravequeospacientesinfectadosporoutrosVRCs(60%e84%,respectivamente, p=0,006),porém maiscomorbidades(40%e27%,respectivamente;p=0,043).Contudo,em umaanáliseajustada,essaassociac¸ãonãofoisignificativa.AtaxademortalidadenogrupoRVH foi3%.Adetecc¸ãodeRVHfoimaisprevalenteduranteooutonoeinverno,comumacorrelac¸ão negativamoderadaentreafrequênciadeinfecc¸ãoviraleatemperatura(r=-0,636,p<0,001), porémnenhumacorrelac¸ãocomaprecipitac¸ão(r=-0,036,p=0,866).
Conclusão: ORVHénormalmentedetectadoemcrianc¸asinternadascominfecc¸õesrespiratórias e normalmenteestá presenteem codetecc¸ões virais. Ascomorbidades estãoestreitamente associadasainfecc¸õesporRVH.Essasinfecc¸õesmostramvariac¸ãosazonal,compredominância duranteasestac¸õesmaisfrias.
©2016PublicadoporElsevierEditoraLtda.emnomedeSociedadeBrasileiradePediatria.Este ´
eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http://creativecommons.org/licenses/ by-nc-nd/4.0/).
Introduction
Human rhinoviruses (HRVs) belong to Picornaviridae fam-ily, genus Enterovirus, and are divided in three species (HRV-A,HRV-B,andHRV-C)withabout100serotypeswithin thesespecies.1,2Thedevelopmentofhighly-sensitive molec-ulartechniquesforcharacterizationoftheHRVgenomehas recentlyallowedrecognition oftheHRV-Cspecies.3 There isalreadyevidencethatthisnewspeciesmaybemore vir-ulent andmorestronglyassociated withlower respiratory tractinfectionsthanHRV-AandHRV-B.4
HRVisthemostcommoncauseofupperrespiratorytract infections, being responsible for at least 50% of cases of thecommoncold.Thisleadstoconsiderableeconomic bur-den in terms of medical visits and both school and work absenteeism.2,4HRVshavealsobeenlinkedtolowerairway effects thatresult in significant morbidity andmortality,1 suchasexacerbationsofchronicpulmonarydisease,severe bronchiolitisininfantsandchildren,aswellasfatal pneumo-niainelderlyandimmunocompromisedadults.4,5Ingeneral,
HRVinfectionsoccurduringspringandautumn,6and man-ifestdifferently dependingonwhetherthelowerorupper respiratorytractisinfected.Infectionsoftheupper respira-torytractordinarilyincludesymptomsofthecommoncold, butcanpresentasacuteotitismediaor rhinosinusitis.On the other hand, infections of the lower respiratory tract cancausesevere symptomsandresultinbronchiolitisand pneumonia.4
Methods
Patientselectionanddataacquisition
Patientshospitalizedatanacademictertiarycarecenterin SouthernBrazil fromwhomrespiratory samples were col-lected andsent for investigation, or who werediagnosed withSARIin2012or2013,wereincludedinthestudy. Respi-ratorysamples (nasalswabornasopharyngeal aspirate,or bronchoalveolarlavage)werecollectedindifferentperiods of hospitalization according to medical recommendation. Individualswithmorethanonesamplecollectedduringthe samesymptomaticperiodwereconsideredasasinglecase andonlythefirstresultwasevaluated,sothatthenumber ofrespiratoryviraldetectionswasnotoverestimated.The medicalrecordsandinfluenzanotificationformsofpatients withdetectablerespiratory virus werereviewed, focusing onepidemiology,clinical manifestation, outcome, labora-toryfindings,anddiagnosis ofSARI.SARIwasdefinedasa flu-likesyndromewithsignsofseverity(dyspneaoroxygen saturationbelow95%).
Duringthestudy,atotalof1002caseswereidentifiedin bothdatabases.Ofthese,fivecaseswereexcludedbecause theresearcherscouldnotaccessthemedicalrecordsanda further242wereexcludedasnosampleshadbeensentfor virusdetection.Thus,755patientswithrespiratorysamples investigatedforrespiratoryvirusdetectionwereincluded. The Institutional Ethics Review Board approved the study (No.#18714013.4.0000.0096).
Respiratoryvirus(RV)detection
RVswere detectedusinga multiplexreverse transcription polymerase chain reaction (RT-PCR) technique. The viral genomewasextractedusingaHighPureViralRNAKit(Roche Inc., Mannheim, Germany) in accordance with the man-ufacturer’s instructions. First strand cDNA synthesis was achieved using random primers and an ImProm-II reverse transcription system (PromegaInc., WI, USA).The result-ing cDNA was then subject to PCR by using a Seeplex® RV15 ACE Detection Kit (Seegene Inc., Korea), in accor-dance with the manufacturer’s protocol. This multiplex
PCR technology enables a simultaneous detection of 15 respiratoryviruses:humanadenovirus(AdV),human metap-neumovirus(MPV),parainfluenzavirus type1, 2,3,and 4 (PIV-1,PIV-2,PIV-3,andPIV-4),influenzaA(FLUA),influenza B (FLUB), respiratory syncytial virus type A and B (RSV-A, RSV-B), human rhinovirus types A/B/C (HRV), human enterovirus(EV),humanbocavirus(BoV),andhuman coro-navirus (CoV) types 229E/NL63 (alpha coronaviruses) and OC43/HKU1(betacoronaviruses).
Statisticalanalysis
DatawerecompiledusingJMP version5.2.1(SASInstitute Inc.,Cary,NC,USA)andanalyzedusingGraphPadPrism ver-sion5.03(GraphPadSoftwareInc.,CA,USA).Parametricand non-parametric tests were usedas appropriate. The non-parametric Spearman correlation coefficient was used to analyzemeteorologicaldata.Variableswithanassociatedp -value<0.05intheunivariateanalysisandthoseconsidered asconfoundingfactors (ageand lengthof hospitalization) weresubjectedtomultivariatelogisticregressiontoidentify independentpredictorsforseveredisease.Allp-valueswere two-tailedandavalueof<0.05wasconsideredsignificant.
Meteorologicaldata
Curitibais locatedinSouthernBrazilandhasatemperate climate.Dataonmonthlymeasuresoftemperatureand rain-fallweresupplied bytheMeteorologicalSystemofParaná (SistemaMeteorológicodoParaná[SIMEPAR]).
Results
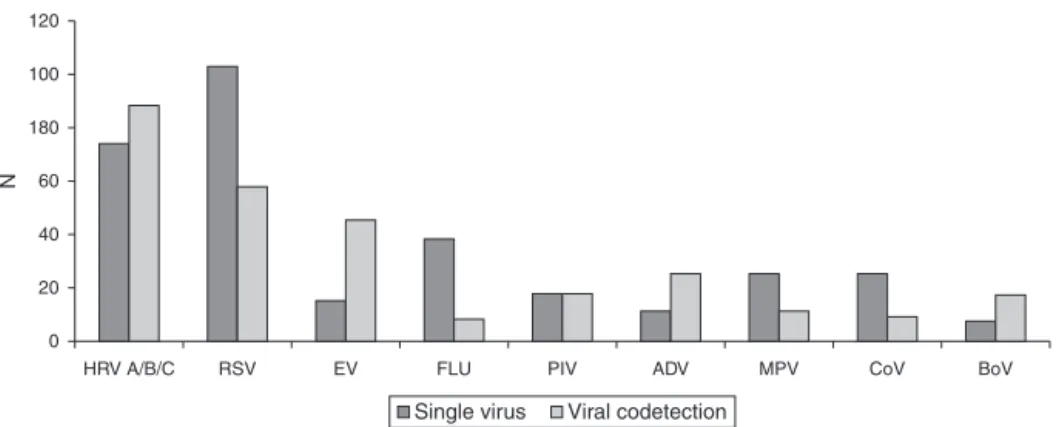
Atotalof444(444/755;59%)sampleswerepositiveforCRV infection,including201(201/444;45%)casesin2012and243 (55%)in 2013.The most frequentlydetectedviruses were HRV(37%)andRSV(36%;Fig.1).Therewere162cases pos-itive for HRVover thestudy period:83 (51%)in 2012 and 79(49%)in2013,with282casesofotherrespiratoryviruses infectionsduringthesameperiod.
To evaluate the epidemiological profile and clinical impact HRV infections, data from HRV infected patients
120
100
180
60
N
40
20
0
HRV A/B/C RSV EV FLU PIV ADV MPV CoV BoV
Single virus Viral codetection
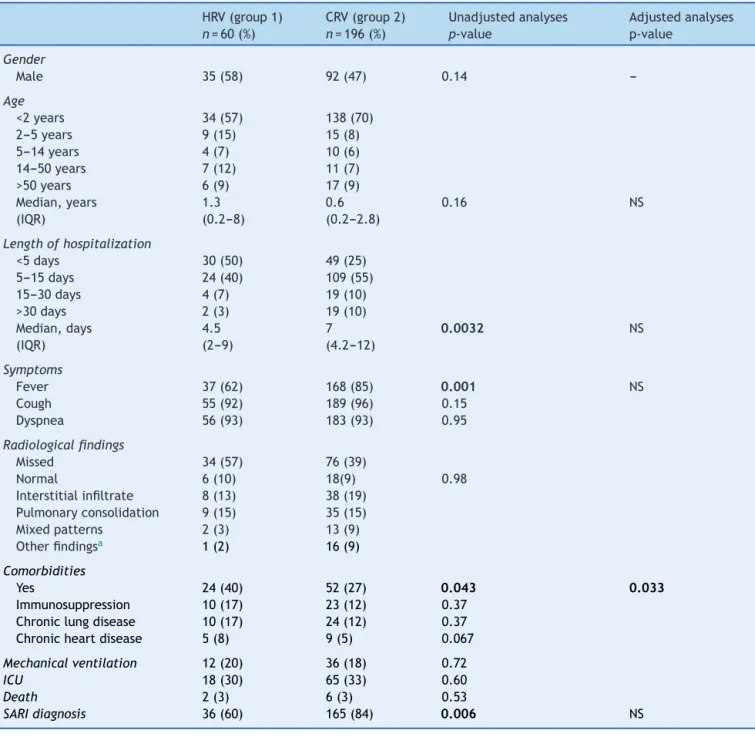
Table1 ComparisonoftheclinicalandepidemiologicalprofileofpatientshospitalizedwithHRV-vs.otherCRV-monoinfections, 2012---2013.
HRV(group1) CRV(group2) Unadjustedanalyses Adjustedanalyses
n=60(%) n=196(%) p-value p-value
Gender
Male 35(58) 92(47) 0.14
---Age
<2years 34(57) 138(70)
2---5years 9(15) 15(8)
5---14years 4(7) 10(6)
14---50years 7(12) 11(7)
>50years 6(9) 17(9)
Median,years 1.3 0.6 0.16 NS
(IQR) (0.2---8) (0.2---2.8)
Lengthofhospitalization
<5days 30(50) 49(25)
5---15days 24(40) 109(55)
15---30days 4(7) 19(10)
>30days 2(3) 19(10)
Median,days 4.5 7 0.0032 NS
(IQR) (2---9) (4.2---12)
Symptoms
Fever 37(62) 168(85) 0.001 NS
Cough 55(92) 189(96) 0.15
Dyspnea 56(93) 183(93) 0.95
Radiologicalfindings
Missed 34(57) 76(39)
Normal 6(10) 18(9) 0.98
Interstitialinfiltrate 8(13) 38(19)
Pulmonaryconsolidation 9(15) 35(15)
Mixedpatterns 2(3) 13(9)
Otherfindingsa 1(2) 16(9)
Comorbidities
Yes 24(40) 52(27) 0.043 0.033
Immunosuppression 10(17) 23(12) 0.37
Chroniclungdisease 10(17) 24(12) 0.37
Chronicheartdisease 5(8) 9(5) 0.067
Mechanicalventilation 12(20) 36(18) 0.72
ICU 18(30) 65(33) 0.60
Death 2(3) 6(3) 0.53
SARIdiagnosis 36(60) 165(84) 0.006 NS
HRV,humanrhinovirus;CRV,community-acquiredrespiratoryvirus;IQR,interquartilerange,ICU,intensivecareunit;SARI,severeacute
respiratoryinfections;NS,notsignificant,OR,oddsratio.
Boldvaluesareinstatisticallysignificant.
a Pleuraleffusion,atelectasis.
werecomparedwiththosewithotherCRVinfections,groups 1and2,respectively)(Table1).Forthisanalysis,onlycases withsingleinfectionswereincluded,excludingnosocomial infections,sincegiventhatpatientswithnosocomial infec-tions were already in the hospital,it would be expected thattheywouldhavesomeunderlyingillness,whichcould overestimatetheseverityofinfections.MostHRVinfected patientswereyoungerthan2years(57%),53%wereyounger than1year, and37%were youngerthan6monthsof age. Thegroupsshowednostatisticallysignificantdifferencein
medianage.Genderwasunequallydistributedbetweenthe groups.
butwithout significantdifference. Concerningthe diagno-sisof SARI,therewerefewerpatients diagnosedwiththis syndrome in the HRV group (60%, p=0.006) than in the otherCRVgroup.Inthemultivariateanalysisofthe relation-shipbetweenclinicalcharacteristicssignificantlydifferent between the HRV- and other CRV-groups, only the higher prevalenceofpreviouscomorbiditiesintheHRVgroupwas significant.Patientswithnocomorbiditieswere1.6(95%CI: 1.04---2.34)timesmorelikelytobeinfectedCRVsotherthan HRV,incomparisontopatientswithcomorbidities.
Despite the fact that most of chest X-rays of HRV infected cases were missed (53%), radiologic alterations weredescribedin83%oftheperformedexams.Mostofthe findingsobservedwereinterstitialinfiltrate(33%)and pul-monaryconsolidation(28%),withnosignificant difference betweenbothgroups.
Severediseasewasdefinedasthatrequiringmechanical ventilatorysupport,orintensivecareunit(ICU)admission, or death during hospitalization; no significant difference wasfoundbetweenthegroups.TwoHRVinfectedpatients diedduringhospitalization,bothfromrespiratoryinfection complications.
HRVhadthehighestratesofcoinfection(69%)ofthe128 sampleswithmorethanoneCRVdetected.Thevirusesmost co-detectedwithHRVwereEV(40/88;45%)andRSV(29/88; 33%),asshowninFig.1.In52%ofcases,theco-detection involvedHRVplus anothervirus,andin 16%ofcases,HRV wasassociatedwithtwoormoreviruses.In65cases,HRV wastheonlyvirusdetected.
A comparison of the clinical characteristics of mono-infected HRV patients with co-infected HRV patients was performed,andnorelationbetweenviralco-detectionand disease severity (p=0.717) was found. The clinical fea-turessignificantly associated with HRV co-detectionwere as follows: age 6---48 months (OR=3.2; 95% CI: 1.3---8.1), lengthofhospitalizationmorethan30days(OR=9.7;95%CI: 2.5---36.8),andnoSARIdiagnosis(OR=4.0;95%CI:1.7---9.3). Asco-infectionwithHRValonewasnotrelatedwithsevere disease, a second analysis was performed comparing dis-easeseveritybetweenHRVco-infectedpatientsandpatients infectedwithotherCRVs.Neitherthepresencenorabsence of HRV co-detection wasassociated with disease severity (p=0.196).
Cases of HRV infection occurred throughout the study period(Fig.2).ThemonthsofMaytoAugustdemonstrated
the highest number of HRV infections during 2012, peak-ing in August (17 cases; 10%).In 2013, the seasonality of HRV infectionwasfromMarchtoMay,peakingin May (19 cases; 12%). Comparing the monthly distribution of HRV cases with average temperature (◦C) and rainfall (mm),
a negative correlation between the number of HRV cases and the average temperature (rs=−0.636, p<0.001) was demonstrated,buttherewasnosignificantcorrelationwith rainfall(rs=−0.036,p=0.866).
Discussion
Sincethe implementationof systematic investigation into respiratoryviruses inhospitalizedpatients withSARI,HRV has been found with high frequency, either alone or co-detectedwithotherrespiratoryviruses.Sincesomeofthese infections may have a poor prognosis, includingdeath, it is critical to know and better characterize this infection tobepreparedforitsearlydiagnosis, appropriateclinical management,andpreventionofnosocomialspread.
ThehighfrequencyofHRVfoundinclinicalsamplesfrom patientswithSARIwassimilartothatreportedbyKimetal.7 in atertiary hospitalin Korea. Heetal.8 analyzed a hos-pitalized pediatric population and found a prevalence of 48%,whileWalkerandIson9foundaprevalenceof14%ina hospitalizedadultpopulation.Thisdifferencebetweenage groupswasobservedinthisstudy,emphasizingthegreater vulnerabilityofchildrentothisinfection,probablyas con-sequenceofamoreintenseinflammatoryprocesstriggered byprimaryinfectionorbyfavorableanatomicalconditions oftherespiratorytractinyoungerchildren.
RSV wasthe first pathogen identified tobe associated with the severe respiratory disease in children. However, sincethe developmentof molecular techniques todetect HRV,thisvirushasbeenthefocusofthemostrecent stud-iesinthisfield.Nowadays,HRVinfectionshavebeenlinked withexacerbationsofchroniclungdiseasesandfatal pneu-moniainpatientsattheextremesofageorwithpre-existing comorbidities.4,5 The importance of one study that eval-uated the characteristics of HRV infections in a tertiary hospitalis basedonthesenewconcerns.Marcone etal.10 reportedahighernumberofHRVinfectionsinhospitalized children in Argentina when compared with pediatric out-patientswithacuterespiratoryinfection,demonstratinga
Jan/2012Feb/2012Mar/2012Apr/2012May/2012Jun/2012Jul/2012Aug/2012Sept/2012Oct/2012Nov/2012Dec/2012Jan/2013Feb/2013Mar/2013Apr/2013May/2013Jun/2013Jul/2013Aug/2013Sept/2013Oct/2013Nov/2013Dec/2013
40 35
25
15 30
20
10
N/T
emper
a
ture ºC
Rainf
all/mm
3
5
0
–5
400
350
250
150 300
200
100
50
0
HRV Other RV Temperature Rainfall
scenario that contributedtothe increased concernabout HRVinfectioninthehospitalsetting.
Previous studies have reported that the HRV infection rate in hospitals varies from 21% to 41%.8,11,12 However, thisvariationisprobablyaccountedfor bythedifferences in age and clinical characteristics of patients analyzed in each study.Althoughthisstudy included allage groups, a predominanceofpediatric patientsinfectedwithHRVwas observed,mostlyyoungerthan1yearold.Inaddition,the HRV-positive group had a greater proportion of patients withpre-existingcomorbidities thanthe groupwithother identified CRVs.6,7,11---14 Among the comorbidities observed inthisstudy,chroniclungdiseaseswerefrequentintheHRV group, a correlation that has already been demonstrated in another similar study,14 which corroborates the close association of HRV infectionand exacerbationsof chronic lungdiseases,suchaschronicobstructivepulmonarydisease (COPD),asthma,andcysticfibrosis.4
Of 444 samples positive for CRVs, 128 samples (29%) had at least two co-detected viruses, in keeping with the expected 10---31% encountered in hospitalized individuals.7,8,15 The viruses most frequently co-detected withHRV were EV (45%), RSV (33%), andAdV (18%); con-sistentwithpreviouslyreportedpatterns.14,15However,the highfrequencyofEVandHRVco-detectionmaybeasaresult ofusingthe5′NRTregionoftheviralgenometoidentifyboth
pathogens,whichmayhaveloweredthespecificityofthe RT-PCRtest.16 Amoreappropriatemeanstodiscernbetween thesespecieswouldbetocarryouttheRT-PCRfollowedby nucleotidesequencingofamplicons.17Thehighlevelofdual infectioninvolving HRVandRSVisoftenexplainedbothby the coexistence of theseviruses throughout the year and theirsimilarseasonalvariation,15butthishypothesisisnot unanimous.12
IncontrasttofindingsreportedbyGokaetal.,15thisstudy didnotshow an association betweendisease severityand viralco-detections.Furthermore,HRVwasnotfoundtohave aprotectiveinfluenceincaseswhereitwasinvolvedin co-detection,astherewasnosignificantdifferenceindisease severity when comparingthe groups withor without HRV co-detection.Likewise,incontradictiontothepresent find-ings,Asneretal.18observedanincreaseddiseaseseverityin childreninfectedwithHRValone.Amongtheprobable fac-torsassociatedwiththesecontrastingfindings,thefollowing maybecited:(i)analysisindifferentgroupsofpatients (out-patientandhospitalized),(ii)assessingasmallnumberof patients,and(iii)adoptionofdifferentseveritycriteria.
Fever was less frequent in patients infected with HRV compared to other CRVs.19,20 Chest X-ray findings were normal in 17%, showed interstitial infiltrate in 33%, and demonstratedpulmonaryconsolidationin28%ofcases,with nosignificant differencebetween the HRVand other CRV groups.ThesepatternsaresimilartothosereportedbyFica etal.11 in hospitalizedadultsinChile. Therewere signifi-cantlyfewercasesofSARIdiagnosedinthepatientsinfected withHRVthanotherCRVs.Overall,14%(110/770)ofpatients withSARIwereinfectedwithHRV.Thisconcurswitha pre-viousstudy.20
ReportsabouttheseasonalityofHRVinfection,including a study from Argentina,10 which is in close geographi-cal proximity of Southern Brazil, show that it circulates mainly in autumn and spring.7,8,19 Although HRV occurred
in almost allmonths of the study period,different peaks wereobservedin2012and2013,andneitherpeakincluded spring.In2013,thehighestprevalenceofHRVinfectionwas inautumn,followedbywinter,andviceversain2012.The analysisofmeteorologicaldatafoundanegativecorrelation betweenthenumberofHRVcasesandtheaverage temper-ature,butnosignificantcorrelationwithrainfall.However, inordertomoreaccuratelyestablishtheseasonalityofHRV infections,theanalysisshouldincludeadditionalyears.
Thisresearchhadsomelimitations:(i)itwasa retrospec-tivestudyandsomemedicalrecordswereincomplete;(ii) HRVspecieswerenotidentified,whichwouldhaveyielded importantdatasincethegenotypesreportedlyhave differ-entvirulence;(iii) this analysis wascarriedout only with hospitalizedpatients, which may have overestimated the impactofHRVinfection;and(iv)itwasnotpossibleto evalu-atethefrequencyofnosocomialHRVinfection,datacritical toguidepreventivemeasuresinthemostaffectedsettings. However,thisisthefirstreportaboutHRVinfectionsinthe regionand a criticalanalysis of the data is important to obtaingreaterawarenessofthedynamicsofdispersionand impactoftheserespiratoryvirusesinthecommunity.
In conclusion, HRV has a high prevalence in the hos-pitalized children and was present in cases of severe disease,including death. However,a dependent relation-ship between the presence of HRV in viral co-detections andseverityofdiseasewasnotobservedinthisstudy. Con-flicts in the literature demand a closer analysis of cases of co-detectioninvolving HRV withreview of the data to determinetheimpactofthis,sincethelackof standardiza-tionbetweenstudiesprobablycontributestothedivergent data.HRVinfectioniscloselyassociatedwithcomorbidities, mainlychroniclungdiseases,andisanimportantfactorin exacerbationsoftheseunderlyinglungdiseases.Thecolder seasonsweretheperiodwithhigherfrequencyofHRV infec-tionsinSouthernBrazil,andthereforemustbeaperiodto warncliniciansaboutyoungagechildrenaffectedby respi-ratoryinfections,especiallythosewithcomorbiditiessuch aschroniclungdisease.Patientswiththisprofileshouldhave respiratorysamplescollectedtoidentifypossibleviral infec-tion,and ifHRV is detected, the medicalstaff shouldbe readyforadequatemanagement,takingintoconsideration thepossiblepooroutcomes.
Funding
SMRissponsoredbyaCNPqfellowship.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.PalmenbergAC,RatheJA,LiggettSB.Analysisofthecomplete genomesequencesofhumanrhinovirus.JAllergyClinImmunol. 2010;125:1190---201.
2.GernJE. TheABCsofrhinoviruses,wheezing, andasthma.J Virol.2010;84:7418---26.
4.Jacobs SE,LamsonDM, St. George K, WalshTJ. Human rhi-noviruses.ClinMicrobiolRev.2013;26:135---62.
5.JacksonDJ,GangnonRE,EvansMD,RobergKA,AndersonEL, PappasTE,etal.Wheezingrhinovirusillnessesinearlylife pre-dictasthmadevelopmentinhigh-riskchildren.AmJRespirCrit CareMed.2008;178:667---72.
6.LitwinCM,BosleyJG.Seasonalityandprevalenceofrespiratory pathogensdetectedbymultiplexPCRatatertiarycaremedical center.ArchVirol.2014;159:65---72.
7.KimJK, JeonJS,KimJW, RheemI.Epidemiology of respira-toryviralinfectionusingmultiplexrt-PCRinCheonan, Korea (2006---2010).JMicrobiolBiotechnol.2013;23:267---73.
8.HeY,LinGY,WangQ,CaiXY,ZhangYH,LinCX,etal.A3-year prospectivestudyoftheepidemiologyofacuterespiratoryviral infectionsinhospitalizedchildreninShenzhen,China.Influenza OtherRespirViruses.2014;8:443---51.
9.WalkerE,IsonMG.Respiratoryviralinfectionsamong hospital-izedadults:experienceofasingletertiaryhealthcarehospital. InfluenzaOtherRespirViruses.2014;8:282---92.
10.MarconeDN,CulassoA,CarballalG,CamposR,EchavarríaM. Genetic diversity and clinical impact of human rhinoviruses inhospitalizedandoutpatientchildrenwithacuterespiratory infection,Argentina.JClinVirol.2014;61:558---64.
11.FicaA,DabanchJ,AndradeW,BustosP,CarvajalI,CeroniC, etal. Clinicalrelevance ofrhinovirusinfectionsamong adult hospitalizedpatients.BrazJInfectDis.2015;19:118---24.
12.GreerRM,McErleanP,ArdenKE,FauxCE,NitscheA,Lambert SB,et al.Dorhinoviruses reducetheprobabilityof viral co-detectionduringacuterespiratorytractinfections?JClinVirol. 2009;45:10---5.
13.PretoriusMA,MadhiSA,CohenC,NaidooD,GroomeM,Moyes J,etal.Respiratoryviralcoinfectionsidentifiedbya10-plex real-timereverse-transcriptionpolymerasechainreactionassay inpatientshospitalizedwithsevereacuterespiratoryillness ---SouthAfrica,2009---2010.JInfectDis.2012;206:S159---65.
14.Rahamat-LangendoenJC,Riezebos-BrilmanA,HakE,Schölvinck EH,Niesters HG. The significance of rhinovirusdetection in hospitalizedchildren:clinical,epidemiologicalandvirological features.ClinMicrobiolInfect.2013;19:E435---42.
15.GokaEA,VallelyPJ,MuttonKJ,KlapperPE.Single,dualand multiplerespiratoryvirusinfectionsandriskofhospitalization andmortality.EpidemiolInfect.2015;143:37---47.
16.GharabaghiF,HawanA, Drews SJ,RichardsonSE.Evaluation ofmultiplecommercialmolecularandconventionaldiagnostic assaysforthedetectionofrespiratoryvirusesinchildren.Clin MicrobiolInfect.2011;17:1900---6.
17.SilvaER,WatanabeAS,CarraroE,PerosaAH,GranatoCF,Bellei NC.RhinovirusdetectionusingdifferentPCR-basedstrategies. BrazJMicrobiol.2012;43:739---43.
18.AsnerSA,RoseW,PetrichA,RichardsonS,TranDJ.Isvirus coin-fectionapredictorofseverityinchildrenwithviralrespiratory infections?ClinMicrobiolInfect.2015;21:e1---6.
19.AponteFE, Taboada B, EspinozaMA, Arias-Ortiz MA, Monge-Martínez J, Rodríguez-Vázquez R, et al. Rhinovirus is an importantpathogeninupperandlowerrespiratorytract infec-tionsinMexicanchildren.VirolJ.2015;12:31.