REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
PublicaçãoOficialdaSociedadeBrasileiradeAnestesiologiawww.sba.com.br
SCIENTIFIC
ARTICLE
Comparison
of
effectiveness
of
intubation
by
way
of
‘‘Gum
Elastic
Bougie’’
and
‘‘Intubating
Laryngeal
Mask
Airway’’
in
endotracheal
intubation
of
patients
with
simulated
cervical
trauma
Esra
Yildiz
Sut,
Solmaz
Gunal,
Mehmet
Akif
Yazar
∗,
Beyazit
Dikmen
DepartmentofAnesthesiology,AnkaraTrainingandResearchHospital,Ankara,Turkey
Received12January2016;accepted29March2016 Availableonline30May2016
KEYWORDS Difficultairway; Cervicaltrauma
Abstract
Purpose:Inthisstudy,weevaluatedtheeffectivenessofintubationsbywayof‘‘GumElastic Bougie’’and‘‘IntubatingLaryngealMaskAirway’’inendotrachealintubationofpatientswith simulatedcervicaltrauma.
Method: 134patientswereincludedinthestudy.Allpatientswereplacedcervicalcollarfor asimulatedcervicaltrauma. Patientswere allocatedrandomlyinto threegroups: GroupNI (n=45)intubationwithMacintoshlaryngoscopy,GroupGEB(n=45)intubationwithGumElastic Bougie,andGroupILMA(n=44)intubationwithIntubatingLaryngealMaskAirway.Thenumber ofintubationattempts,successofintubation,durationofcompletevisualizationofthe lar-ynx,durationofintubation,user’sperformancescore,hemodynamicchangesandtheobserved complicationswererecorded.
Results:SuccessofintubationinthefirstattemptwashighestinGroupGEBwhileitwaslowest inGroupILMA.Regardingtheintubationsuccess,ratesofsuccessfulintubationwere95.6%, 84.4%and65.9%inGroupsGEB,NI,andILMA,respectively.Durationsofvisualizationoflarynx andintubationwereshorterinGroupsNIandGEBthaninGroupILMA.Thisdifferencewas sta-tisticallysignificant(p<0.05)whiletherewasnosignificantdifferencebetweenGroupsNIand GEB.Thenumberofpatientswith‘‘good’’intubationperformancewassignificantlyhigherin GroupGEBwhilethenumberofpatientswith‘‘poor’’intubationperformancewassignificantly higherinGroupILMA(p<0.05).
∗Correspondingauthor.
E-mail:[email protected](M.A.Yazar).
http://dx.doi.org/10.1016/j.bjane.2016.03.001
Conclusions: WeconcludethatGEB,whichischeapandeasilyaccessible,shouldbean advan-tageous choiceincervicaltrauma patients for boththeeaseness ofintubationandpatient morbidityandmortality.
©2016SociedadeBrasileiradeAnestesiologia.Publishedby ElsevierEditoraLtda.Thisisan openaccessarticleundertheCCBY-NC-NDlicense(
http://creativecommons.org/licenses/by-nc-nd/4.0/).
PALAVRAS-CHAVE Viaaéreadifícil; Traumacervical
Comparac¸ãodaeficáciadeintubac¸ãopormeiodeguiaintrodutorBougiedetubo endotraquealemáscaralaríngeaemintubac¸ãotraquealdepacientescomtrauma cervicalsimulado
Resumo
Objetivo: Nesteestudoavaliamosaeficáciadeintubac¸õespormeiodeguiaintrodutorBougie emáscaralaríngeaemintubac¸ãoendotraquealdepacientescomtraumacervicalsimulado.
Método: Foramincluídos no estudo134 pacientes. Colarcervical foicolocado em todosos pacientesparaumtraumacervicalsimulado.Ospacientesforamalocadosaleatoriamenteem trêsgrupos:GrupoNI(n=45)foisubmetidoàintubac¸ãocomlaringoscópioMacintosh;Grupo ITE(n=45)foisubmetidoàintubac¸ãocomguiaintrodutordetuboendotraquealeGrupoML (n=44)foisubmetidoàintubac¸ãocommáscaralaríngea.Númerodetentativasdeintubac¸ão, sucessodeintubac¸ão,tempodevisualizac¸ãocompletadalaringe,tempodeintubac¸ão,escore dedesempenhodousuário,alterac¸õeshemodinâmicasecomplicac¸õesobservadasforam reg-istrados.
Resultados: Osucessodaintubac¸ãonaprimeiratentativafoimaiornoGrupoITEemenorno grupoML.Aindaemrelac¸ãoaosucessodaintubac¸ão,astaxasdesucessoforam95,6%,84,4% e65,9%nosgruposITE,NIeML,respectivamente.Ostemposdevisualizac¸ãodalaringeede intubac¸ãoforammenoresnosgruposNIeITEquenoGrupo ML.Essadiferenc¸afoi estatisti-camente significativa, p<0,05), enquantonão houvediferenc¸a significativaentreosGrupos NIeITE. Onúmerode pacientescombom desempenho naintubac¸ãofoisignificativamente maiornogrupoITE,enquantoonúmerodepacientescommaudesempenhonaintubac¸ãofoi significativamentemaiornogrupoML(p<0,05).
Conclusões: ConcluímosqueoITE,queébaratoefacilmenteacessível,deveserumaopc¸ão vantajosaempacientescomtraumacervical,tantopelafacilidadedeintubac¸ãoquantodevido àtaxademorbidadeemortalidadedospacientes.
©2016SociedadeBrasileiradeAnestesiologia.PublicadoporElsevierEditoraLtda.Este ´eum artigo OpenAccess sobumalicenc¸aCCBY-NC-ND(
http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Endotrachealintubationisthefirstandthemostimportant invitationtoensuretheairwaysafetyinpatientundergoing generalanesthesia.Endotrachealintubatingindifficult air-wayconditionsismoreimportantforpatient’sairwaysafety. Someofthedifficultairwayconditionsarethelimitationof cervicalspinemovementandthecasesmustbekeptlimited neck movement. Neck movements must be particularly limitedinnecktraumapatients.Itis extremelyimportant toquicklyanduncomplicatedintubatethispatientfortheir vitalfunctions.Sovariousmethodshavebeensuggestedto intubatethispatient.Inthisstudies,weaimedtocompare theeffectivenessofFastrach-LMA(IntubatingLaringealMask Airway---ILMA)hasbeen developedforblindintubationin difficultairwayconditionsandGumElasticBougie(GEB).
Method
Afterlocalethicscommitteeapproval(theregistration pro-tocolnumber3449),thisstudywasperformedprospectively
attheAnkaraTrainingandResearchHospitalbetweenMarch andJune2011.135patientsscheduledforelectivesurgery, between18and65,ASAcriteriaI---II,wereincludedinthe study.Prodecureswereexplainedindetailtoallpatients. Patientswhohadhistoryofdifficultintubation,cervical pos-turaldisorders,undergoingcervicalsurgery,bodymassindex over 30kg·m−2, mallampati score III---IV, thyromental
dis-tancelessthan6cm,riskofgastricaspirationandpregnant wasexcludedformstudy.
Themouthopening,thyromentaldistances,and Mallam-patiscoreswere recordedin thepreoperative assessment performedonedaybeforethesurgery.Thecasesweretaken totheoperatingroomwithoutanypremedicationandwere monitored with regard to Electrocardiogram (ECG), non-invasive blood pressure, pulse oximeter, and EtCO2. The
patientsweresplitintothreegroupsandcervicalcollar (Stif-neckOriginalCollar,LaerdalMedicalCorporation,USA)was employedtoestablishsimulateddifficultintubation.After the removalof the collar, mouth opening was measured. Allthecasesinhaled100% O2 for3min (6L·min−1),
induc-tionwasestablished using1mcg·kg−1 fentanylcitrateand
Figure1 Gumelasticbougie.
0.6mg·kg−1 rocuronium bromide. The categorization into
groups was performed by random selection. Intubations were performed by a single anesthesiologist who had an experienceof more than 3 years.Each patient was cate-gorizedbyCormackLehane classificationwithout applying externalpressure.TheNIgroup(NormalIntubation)(n=45) were intubated with a Macintosh® laryngoscope using a Saviour®endotrachealtube,whiletheGEBgroup(Gum Elas-ticBougie,Fig.1)(n=45)wereintubatedwiththehelpof aMacintosh® laryngoscopeandGEBusingaSaviour® endo-tracheal tube, and the ILMA Group (Intubating Laryngeal MaskAirway,Fig.2)(n=45)wereintubatedwithaFastrach LMA using a Saviour® endotracheal tube. The femaleand malepatientswereintubatedwithacuffof7---7.5mmand 7.5---8.5mm,respectively;theanesthesiamaintenancewas achivedby50%O2(2L·min−1),50%N2O(2L·min−1),and2%
sevoflurane.
The time for laryngoscope or ILMA insertion, total intubation time (time to monitoring of the EtCO2 in
the capnography), number of intubation attempts, and Cormack-Lehane classification were recorded. The inser-tionof the intubation tube into the trachea wasdeemed as ‘‘succesful’’; while failure to insert, insertion taking morethan 60s, or making morethan 2 attempts at intu-bation was recognized as an ‘‘unsuccessful’’ attempt. In unsuccessfulcases,thecervicalarmswereremovedandthe intubationwasperformedusingaMachintoshlaryngoscope. Thecasesrequiringanadditionalmethodwerenoted.The ‘‘operator performance assessment’’ of the anesthesiolo-gistperformingtheintubationwascategorizedas‘‘good’’,
Figure2 IntubatingLaryngealMaskAirway.
Table1 Demographicdataonthegroups.
NI(n=45) GEB(n=45) ILMA(n=44)
Sex(F/M) 27/18 27/18 28/16 Age(mean±SD) 46±2.7 50±2.7 48±2.7 BMI 26.6±2 26.9±2 26.8±2 ASAI/II 35/10 30/15 33/11 SMD(cm)
(mean±SD)
16.18±2.2 16.73±2.0 17.16±2.5
TMD(cm) (mean±SD)
7.42±0.5 7.47±0.6 7.48±1.0
MO(cm) (mean±SD)
5.0±0.63 5.0±0.61 5.0±0.64
Cormack-Lehane Classification
2.24±0.5 2.42±0.5 2.34±0.5
BMI,bodymassindex;SMD,sternomentaldistance;TMD, tiro-mentaldistance;MO,mouthopening(whileinsertedcolar);SD, standarddeviation.
‘‘moderate’’,and‘‘poor’’.Thecomplicationsarisingduring intubation(mucosaldamage,dentaltrauma,lipinjury,torn cuff,hypoxia(SpO2<95%),andesophagealintubation)were
recorded.Subsequent tointubation, presenceof bloodon theEndotrachealTube(ETT)cufforanysignofsorethroat expressedbythepatientafterrecoverywerenoted,aswell. Hemodynamicparametersweremonitored throughout the entireoperationandrecordedbeforeinduction,rightafter induction,andatevery5minfor15min.
Statisticalanalysis
‘‘SPSSforWindows16.0.1’’packageprogramwasusedfor the statisticalanalysis. The studydata wereexpressedas mean,standarddeviation,percentage,andnumericvalues. Theintergroupcomparisonsofthemeasureddatawere per-formed by the Mann---Whitney U test and the intragroup comparisons were carried out by the Wilcoxon test. The comparisons of the countable data were performed by the Chi-square test; p<0.05 was recognized as statis-ticallysignificant.
Results
Table 2 Distribution of intubation attempts between groups.
NI (n=45)
GEB (n=45)
ILMA (n=44)
p
1Attempt 30(66%) 42(93%) 20(45%) 0.00 2Attempt 14(31.1%) 2(4.4%) 20(45%) 0.00 3Attempt 1(2.2%) 1(2.2%) 4(9.1%) 0.00
Table3 Intubationsuccessofthegroups.
NI (n=45)
GEB (n=45)
ILMA (n=44)
p
Successful intubation (n)
38(84.4%) 43(95.6%) 29(65.9%) 0.001
Unsuccessful intubation (n)
7(15.6%) 2(4.4%) 15(34.1%) 0.001
Note:Exceeding60sfordurationofintubationandattempting morethantwicefornumberofintubationhavebeenaccepted as‘‘unsuccessfulIntubation’’.
Table4 Laryngealvisualizationtimeandintubationtime betweengroups.
NI(n=45) GEB(n=45) ILMA(n=44)
Laryngeal visualization time(s) (mean±SD)
14.4±0.7 12.6±1.0 43.7±0.8a,b
Intubationtime (s)
(mean±SD)
41.0±1.1 36.0±0.6 92.0±1.0a,b
The duration of insertion of ILMA into the mouth has been acceptedaslaryngealvisualizationtimeintheILMAgroup.
a ILMAgroupvs.NIgroup:p<0.05. b ILMAgroupvs.GEBgroup:p<0.05.
procedurewasdeemedunsuccessful in2of 44patientsin theGEBgroupandin5of44patientsintheNIgroupbecause theintubationtimewasmorethan60s.IntheILMAgroup, thistimewasprolongedin21of40patients.Therefore,the success rate for intubation was 95.6% (n=43) in the GEB group,84.4%intheNI group(n=38),and65.9% (n=29)in theILMAgroup(Caseswithmorethan2attemptsat intuba-tionorthosewithanintubationtimehigherthan60swere deemedunsuccessful).Theintergroupdifferencewasfound tobestatisticallysignificant(p<0.05).Theintubation suc-cess rates of the groups are shown in Table 3. Regarding thevisualizationoflarynxandintubationtime,NIandGEB groupsdemonstratedshortertimesthantheILMAgroup.This differencewasstatistically significant (p<0.05), however, therewasnosignificantdifferencebetweentheNIandGEB groups in this regard. Laryngeal visualization and intuba-tiontime relativetogroups are shown inTable 4. By the anesthesiologist,theintubationperformanceswere catego-rized as‘‘good’’, ‘‘moderate’’,and‘‘poor’’. Accordingly, the‘‘good’’ performanceratewas86%(n=39)in theGEB group,66%(n=30)intheNIgroup,and47%(n=21)inthe
Table 5 The operator performance rates relative to groups.
NI(n=45) GEB(n=45) ILMA(n=44)
Good(n) 30(66%)c 39(86%)a,b 21(47%)
Moderate(n) 8(17%) 4(8%) 10(22%)
Poor(n) 7(15%) 2(4%) 13(29%)b,c
a NIgroupvs.GEBgroup:p<0.05. b GEBgroupvs.ILMAgroup:p<0.05. c NEgroupvs.ILMAgroup:p<0.05.
ILMAgroup.The‘‘good’’performanceratewassignificantly higherintheGEBgroup(p<0.05).
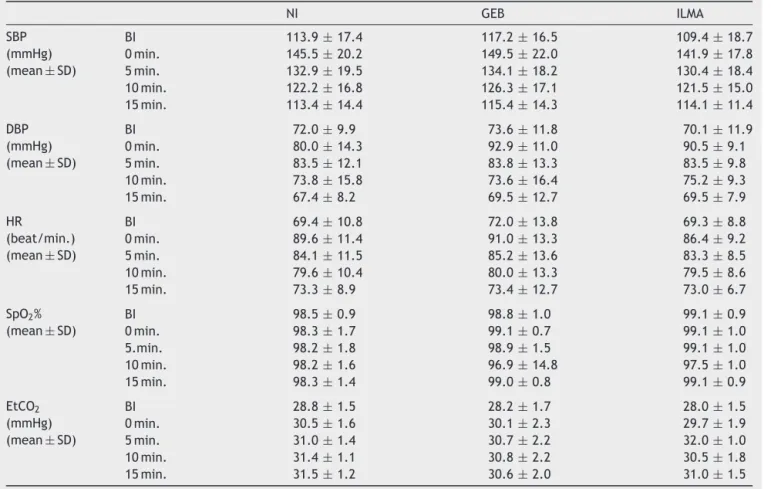
‘‘Poor’’ performance ratewas29% (n=13) inthe ILMA groupwhichwassignificantlyhigherthanthoseintheNIand GEBgroups(p<0.05).Theoperatorperformancerates rela-tivetogroupsareshowninTable5.Therewasnostatistically significantdifferencebetweenthethreegroupswithregard toSBP,DBP,HR,SpO2 andEtCO2 valuesbeforeintubation,
rightafterintubation,andat 5,10,and15min after intu-bation.Thedatainvolvingthesehemodynamicparameters areshowninTable6.Intermsofintubationcomplications suchashypoxia,laryngospasm,orlipinjury,onepatientin eachofILMAandNIgroupsdevelopedhypoxia,onepatient intheNIgroupdevelopedlipinjury,whileanotherexhibited laryngospasm.Itwasnecessarytoremovethecervicalcollar in2patientsineachofNIandGEBgroups,andin8patients intheILMAgroup.
ThetotalnumberofcomplicationsintheILMAgroupwas 15(34%), while it was3 (6%)and 6 (13%)in the GEBand NIgroups,respectively.Thedifferencebetweenthegroups wasstatisticallysignificant (p<0.05).Therewasno signif-icantdifferencebetweenthegroups relativetofrequency ofsorethroat.Theintraoperativecomplicationand postop-erativesorethroatvaluesrelativetothegroupsareshown inTable7.
Discussion
Inthisstudy,wecomparedthesuccess ratesofintubation withGEBand ILMAinpatients difficulttointubatedue to cervical limitation. GEB wasobserved to be more advan-tageous with regard to ease of intubation, as well as in patient morbidity and mortality. Patients with a cervical traumaareregardedasdifficultintubationcases.Thereare ongoingstudiesfordeterminingthebestintubationmethod inpatientssuspectedofhavingcervicaltrauma.1Moreover,
variousmethodsarebeinginvestigatedsuchasawakeblind nasal, oral, or fiberoptic intubation2; direct laryngoscopy
withheadandneckstabilization3;cricothyrotomy,indirect
laryngoscopywithBullardlaryngoscopy,4andblindoral
intu-bationwithAugustineguide5andCombitube.6
Table6 Thehemodynamicparametersofgroups.
NI GEB ILMA
SBP (mmHg) (mean±SD)
BI 113.9±17.4 117.2±16.5 109.4±18.7
0min. 145.5±20.2 149.5±22.0 141.9±17.8 5min. 132.9±19.5 134.1±18.2 130.4±18.4 10min. 122.2±16.8 126.3±17.1 121.5±15.0 15min. 113.4±14.4 115.4±14.3 114.1±11.4
DBP (mmHg) (mean±SD)
BI 72.0±9.9 73.6±11.8 70.1±11.9
0min. 80.0±14.3 92.9±11.0 90.5±9.1
5min. 83.5±12.1 83.8±13.3 83.5±9.8
10min. 73.8±15.8 73.6±16.4 75.2±9.3
15min. 67.4±8.2 69.5±12.7 69.5±7.9
HR
(beat/min.) (mean±SD)
BI 69.4±10.8 72.0±13.8 69.3±8.8
0min. 89.6±11.4 91.0±13.3 86.4±9.2
5min. 84.1±11.5 85.2±13.6 83.3±8.5
10min. 79.6±10.4 80.0±13.3 79.5±8.6
15min. 73.3±8.9 73.4±12.7 73.0±6.7
SpO2%
(mean±SD)
BI 98.5±0.9 98.8±1.0 99.1±0.9
0min. 98.3±1.7 99.1±0.7 99.1±1.0
5.min. 98.2±1.8 98.9±1.5 99.1±1.0
10min. 98.2±1.6 96.9±14.8 97.5±1.0
15min. 98.3±1.4 99.0±0.8 99.1±0.9
EtCO2
(mmHg) (mean±SD)
BI 28.8±1.5 28.2±1.7 28.0±1.5
0min. 30.5±1.6 30.1±2.3 29.7±1.9
5min. 31.0±1.4 30.7±2.2 32.0±1.0
10min. 31.4±1.1 30.8±2.2 30.5±1.8
15min. 31.5±1.2 30.6±2.0 31.0±1.5
SBP,systolicbloodpressure;DBP,diastolicbloodpressure;HR,heartrate;SpO2,oxygensaturation;EtCO2,end-tidalcarbondioxide;BI,
beforeintubation.
Table7 Theintraoperativecomplicationandpostoperativesorethroatvaluesrelativetothegroups.
NI(n=45) GEB(n=45) ILMA(n=44) p
Intraoperativecomplications(+/−)(n,%) 6(13)/39(86) 3(6)/42(93) 15(34)/29(65) 0.02a
Postoperativesorethroat(+/−)(n,%) 29(64)/16(35) 33(73)/12(26) 22(50)/22(50) 0.07
(+/−),complicationpresent/complicationabsent.
aILMAgroupvs.GEBandNIgroup:p<0.05.
Theprotectionofthecervicalspinefollowingtraumais anessentialpartofpatientmanagement.Advancedtrauma lifesupportrequiresthecontinuouscervicalimmobilization ofpatientsbyasemi-rigidcervicalcollar.Thecollarshould notberemoveduntilrulingoutsignificantnecktrauma.In suchpatientsrequiring intubation,fiberoptic intubationis thebestchoice.However,intubationisoftenanemergency procedure that is carried out under stressful conditions far fromideal. It is difficult toapply direct laryngoscopy in patients with cervical collar, and generally it cannot beperformed. The use of semi-rigid collarsincreasesthe Cormack---Lehanegrade 3and 4laryngoscopicviewduring directlaryngoscopy,whilereducingthemouthopening.7To
ensureoptimalviewindirectlaryngoscopy,manualin-line stabilizationisanalternativetechnique.Insuchcases,the collarshouldberemovedwithminimalcervicalmovement byanexperiencedtraumateamandtheneckofthepatient shouldbekeptinin-linepositiononafirmground.Afterthe intubation,thecollarshouldbeplacedagain.
Avidan et al.8 compared the success rates of
ventila-tionandintubationusingdirectlaryngoscopyandtheILMA appliedonmanikin and patientsby inexperienced health-care workers who received a basic training before the intubation. The success rate of ILMA insertion was 100%, while the success rate of intubation using direct laryn-goscopy was84%,andthesuccess rateofintubationusing ILMAwas98%inmanikins.Ontheotherhand, thesuccess ratesofILMAinsertion,intubationusingdirectlaryngoscopy, and intubation using ILMA were 100%, 35%, and 43% in patients, respectively. Adequate ventilation wasachieved in78%ofpatientsinwhomafacemaskwasusedandin98% ofpatients inwhomILMAwasused.Thus,theyconcluded that ILMA could be useful in emergency oxygenation and ventilation, while also adding that their results were not supporting the use of ILMAby inexperienced personnel in advancedairwaymanagement.Waltletal.9evaluatedthe
successfulatfirstattemptin100%,intubationwithILMAwas succesfulin92.5%,intubationtimewithILMAatfirstattempt was39s(31---57),andintubationtimewithlaryngoscopywas 21s(16---34).ILMAwasfoundtocauselessextensionduring intubation ascompared todirect laryngoscopyand direct laryngoscopy wasobserved to provide rapid intubation in theabsenceofdifficultintubationconditions,however,ILMA wasprovidingfasterandsaferintubationindifficult intuba-tioncases.
Nileshwar et al.10 evaluated the efficacy of Bullard
laryngoscopy vs. ILMA in patients withsimulated cervical immobilization andILMA was observed toprovide intuba-tionfasterthantheBL.Theintubationsuccessratewas90% intheBLgroupand74%intheILMAgroup;however,the dif-ferencewasnotstatisticallysignificant. Nakazawaetal.11
tested blind intubation withILMA in patients who under-wentcervicalspinesurgery.ILMAwassuccessfullyinserted in 100%, patients with a Halo bandagerequired a second attempt,successrateatfirstattemptwas60%inintubation withILMA,andtheprocedurefailedin10%ofthepatients. TheyreportedthatachievementofILMAinsertionand intu-bationwithILMAdidnotcauseheadandneckmovements, and theyassociated failureof blind intubation withusing impropermasksizes.Komatsuetal.12evaluatedintubation
withILMAinpatientsofcervicalspinesurgerywitharigid collar and in normal surgery patients with nocollar. Col-lar usewasobservedtonarrow themouth opening,while increasingtheMallampatiscore.Overallintubationsuccess ratewas96%inpatientswithcollarand18%ofthepatients requiredmorethan2attempts.Intubationtimewas60sin patientswithcollarand50sinpatientswithnocollar.They reportedthat incases usingimmobilized rigidcollar, par-ticularlyinthosewhere fiberopticapproachisimpossible, intubationwithILMAmightbeasafeoptionfortheairway management.
InthestudyofBilginetal.,13totalintubationsuccessrate
was87%,thesuccessrateatfirstintubationattemptwas47% andthesuccessrateatsecondintubationattemptwas77% intheILMAgroup.TheILMAinsertiontimewas26.8sandthe totalintubationtimewithILMAwas70s.TheyreportedILMA asauseful deviceinthemanagementofdifficultairways. Beinetal.14 conducteda studyonpatientsanticipatedto
showdifficultairwaymanagement.IntheILMAgroup, suc-cessful intubation rate at firstand second attempts were 70%and90%,respectively.Intubationcouldnotbeachieved in5%ofthepatients,whiletheILMAinsertiontimewas28s andtheILMAintubationtimewas70s.TheynotedILMAas anadvantageousdeviceinthemanagementofdifficult air-ways,aswell.Inanotherstudy,themedianblindintubation timewithILMAwas87s,totalsuccessratewas94%,while theratesofsuccessatfirstandsecondattemptswere67% and86%,respectively.15
In the present study, the results concerning the total success rates for ILMAinsertion, success rates relativeto number of attempts, ILMA insertion time,and intubation time with ILMA were comparable to the values reported in theliterature. The differences maybe associatedwith thestudy design,definitionofsuccess, anddetermination of the times. The significantly ‘‘poor’’ operator perfor-mancein ILMApatients isbelieved tobe arisingfromthe inadequacy ofILMA incases withcervical mobility limita-tion. In this study, success at first and second intubation
attemptswere95.6%and97.7%,whilethesuccessratewas 99.5% in theGEB group. Laryngeal visualization time was 12.6s and the intubation time was 36.0s. Regarding the operatorperformance,GEBapplicationwasgoodin86%and poorin4%.
GumElasticBougie(GEB)iscommonly usedin practice inthe UK. Theapplication of GEBin difficult oral intuba-tionhasbeen increasingoverthepast years.Whileit was used in 45% of difficult intubation cases in 1984, it was determined to be the first choice in 100% of such cases in1996;CardiffdescribesGEBasthemethodof choicein cases of difficult intubation.16 When the visualization of
theglottisis notgoodduringlaryngoscopy, GEBis recom-mended.Incasesofunanticipateddifficultintubation,use of GEBis claimedtoaccelerate the intubation process.17
VariousstudieshavenotedtheefficacyofGEBinthe man-agementofcasespresentingwithdifficultintubation.3,18,19
PatientsofCormack---Lehanegrade3havebeenreportedto haveaGEBsuccessrateof94---100%.17,19---21
Noguchietal.22 comparedtheuse ofGEBandstyletin
patientsreceivingcricoidpressure.Theyusedthemodified laryngealclassificationofCook.TheendotrachealGEB inser-tiontimeinpatientsanticipatedtopresenteasyintubation was12sandtheintubationtimewas31s.Inpatients antic-ipatedtopresent adifficult intubation, endotrachealGEB insertiontime was15s and the intubation timewas33s. Theynotedthatcricoidpressurewouldcomplicatethe tra-cheal intubation, while adding that GEB use wasan easy methodtoincreasethesuccessrateoftrachealintubation. InthestudyofKomatsuetal.,23endotrachealinsertiontime
of GEB was 21s and the intubation time was 49s. Endo-tacheal GEB insertion was successful at first and second attemptsin73%and89.6%,respectively.Intubationwas suc-cessfulatfirstandsecondattempts in83.3%and95.8%of thepatients,respectively.OverallsuccessrateofGEBwas 89.6%.Messaetal.24investigatedthesimplicityandsuccess
ofintubationwithGEBinthemanagementofdifficult air-way.The successrateofintubationwithGEBwas94%and theintubationtimewas20.4s.Theyreportedahighsuccess ratefor GEB use in the managementof difficult airways. Inthepresent study,ourresultsconcerningGEBusewere comparabletotheonesreportedintheliterature.
Repeated attempts at intubation, aiming to maintain the airway safety may lead to higher complication rates includinghypoxia,pulmonaryaspiration,andhemodynamic sideeffects.25 Repeatedintubation attempts, particularly
inpatientswithdifficultairway,mayalsoresultinlaryngeal perforationorpharyngealstricture.26Therefore,intubating
thepatientwithlessmanipulationandinshortertimeshould reducethecomplicationratestominimallevels.
Prolongedlaryngoscopyandintubationmaycausemany complications such as hypoxia and increased secretion. Particularly in the presence of indications complicating theintubationprocedure, each anesthesiologistshouldbe awareofthefactthatriskofprolongedorfailedintubation ishigh.
of the endotracheal tube, and removal of the ILMA. GEB requiresshortertimesbecauseGEBmanipulationissimpler thanILMAandML,leadingtoeasierlaryngealvisualization andendotrachealintubation.Inthepresentstudy,although wefoundshorterintubationtimesintheGEBgroupthanin theNIgroup,thedifferencewasnotstatisticallysignificant. Patientswitha cervical collar requiremore manipulation duringtheinsertionofILMAwhichhasanegativeeffecton thetimeandsuccessoftheintubationprocess.Owingtoits specialdesign,GEBrequireslessmanipulation.
Laryngoscopy andendotracheal intubation trigger sym-pathetic response by the mechanical stimulation of the larynxandtrachea,leadingtoincreasesintheplasma cat-echolamine levels which may in turn cause tachycardia, hypertension,arrhytmia,ormyocardialischemia.27Factors
such as age, weight, and body mass index are known to influencethesuccessofandhemodynamicresponsestothe intubationprocess.
The ILMA may exert a pressure over the oropharygeal structures and cervical spine, leading to back slides in thecervicalvertebraeresultinginincreasedhemodynamic responseduetoraisedlevelsofstimulation.28Moreover,the
epiglotticelevatorof theILMA maystimulate periepiglot-ticstructures andarouse astrong hemodynamic response by affecting the supralaryngeal region known to be rich ofnociceptivereceptors.29 Inaddition,whileremovingthe
ILMA after intubation, the back and forth movement of the intubation tube may create a strong friction, leading toincreasedhemodynamicresponse,aswell.
Kiharaetal.30categorized75normotensiveand75
hyper-tensive patients into3 groups consisted of 25 patients in a randomized fashion; performed intubation using direct laryngoscopy, ‘‘lightwand’’, and ILMA; and recorded the hemodynamic data before and after induction, as well as before and after intubation. Although there was no differencebetween the groups in normotensive patients, hypertensive patients demonstrated a reduced hemody-namic response in the ILMA group. HR was observed to increase after the intubation as compared to baseline valuein all groups,however, therewasnosignificant dif-ference between the groups. The authors associated the reducedhemodynamicresponsewithlowerdegreeof recep-tor stimulation in that region. In the study of Baskett etal.31conductedon500patients,hemodynamicdatawere
recordedafterinductionduringILMAinsertion,intubation, and ILMA removal. Mean HR and BP increased following theinsertion of the ILMA, anddemonstrated a significant increaseaftertheintubation,however,nosignificantchange wasobservedduringtheremoval.
Inthe presentstudy,hemodynamic parametersshowed anincreaseat 0minascomparedtopreintubation values, while nodifferencewas determinedbetween the groups. Theintragroupincreaseswere notstatisticallysignificant; therefore,these raisedvalues werethoughttobenormal responsestointubation.Albeitnotstatistical;SBP,DBP,and HRwereclinicallylowerat0minintheILMAgroup,which wasassociatedwiththepresenceoflessstimulationinthat region,sinceitisknownthatanadvantageofintubationwith ILMAisthatitdoesnotstimulatethebaseoftongue, epiglot-tis, and pharyngeal receptors. Therefore, cardiovascular responsetoendotrachealintubationwithILMAisexpected tobelow.32
In this study, no significant difference was observed betweenthegroupswithregardtopreintubationand postin-tubationlevelsofSpO2vs.EtCO2.Onlyonepatientineach
of ILMA and NI groups developed hypoxia. Although intu-bation times were significantly longer in the ILMA group as compared to NI and GEB groups, the unchanged SpO2
vs. EtCO2 values were explained with the absence of
a significantly prolonged intubation time. The reason is the entire FRC (approximately 2300mL) comprises O2 in
patientsreceiving100%oxygenfor2minasastandard pro-cedure for preoxygenationwhich delayshypoxia following apnea 4---5min.33 Both the changes in the hemodynamic
parametersandourresults concerningtheSpO2 vs.EtCO2
levels were consistent with those reported in the litera-ture.
Manycomplicationsmayariseduringintubationsuchas traumatothelip,dentalandmucosalinjuries,and desatura-tion.Also,pharyngealstructuresmaybedamagedinblind intubation with ILMA. In the literature, there are studies reportingdevelopmentofedemaintheepiglottisfollowing blindintubation.34Moreover,thereisastudyreportingthe
deathofapatientduetoesopharyngealperforationbecause ofblindintubation.35 Itisnoteasytoevaluate
postopera-tivesorethroatincidenceofILMA,36however,somestudies
recognizethatthisincidenceisupto67%.37However,some
studieshave foundnosignificantdifferencebetweenILMA anddirectlaryngoscopywithregard topostoperative sore throat.38
Bilginetal.13observedhigherratesofpostoperativesore
throatintheILMAgroupandexplainedthiswiththe neces-sity toapplymoremanipulation.In theirstudy,Nileshwar etal.10comparedILMAandBL,andfoundnosignificant
dif-ference between the twogroups in terms of sore throat. Moreover, there was no significant intergroup difference withregardtointubation-relatedtrauma.Theyfoundblood onthe ETTin 2of 3cases whichrequired a third intuba-tion attempt in the BL group, while there was blood on theETTinallthepatientsthatrequiredathirdintubation attemptintheILMAgroup.Theyassociatedthisfindingwith higherincidenceofsofttissuetraumainpatientsneedinga thirdintubationattempt.
Inthe present study,2 patients in each ofNI and GEB groups,and8patientsintheILMAgroupcouldbeintubated aftertheremovalofthecervicalcollar;onepatientineach of ILMAand NI groups developedhypoxia, while in theNI group, 1 patienthad lip injury and one patientexhibited laryngospasm.ThecomplicationsintheILMAgroupshowed significant differences as compared to the NI and GEB groups, whichwasafindingconsistentwiththestudies of Baskettetal.31andChoyceetal.32Postoperativesorethroat
isoftenassociatedwiththenumberofmanipulations.25 In
thepresentstudy,therewasnosignificantdifferencewith regardtopostoperativesorethroat.
Conclusion
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.Hastings RH, Marks JD. Airway management for trauma patientswithpotentialcervicalspine injuries.Anesth Analg. 1991;73:471---82.
2.MeschinoA, Devitt JH,Koch JP, et al. Thesafety of awake tracheal intubation in cervical spine injury. Can J Anaesth. 1992;39:114---7.
3.NolanJP, WilsonME.Orotrachealintubation inpatientswith potentialcervicalspineinjuries.Anindicationforthegum elas-ticbougie.Anaesthesia.1993;48:630---3.
4.HastingsRH,VigilAC,HannaR,etal.Cervicalspinemovement during laryngoscopy with the Bullard. Macintosh, and Miller laryngoscopes.Anesthesiology.1995;82:859---69.
5.Fitzgerald RD, Krafft P, Skrbensky G, et al. Excursions of the cervical spine during tracheal intubation: blind oral intubation compared with direct laryngoscopy. Anaesthesia. 1994;49:111---5.
6.FrassM,FrenzerR,RauschaF,etal.Evaluationofesophageal trachealcombitubeincardiopulmonaryresuscitation.CritCare Med.1987;15:609---11.
7.ArslanZI, YildizT, Baykara ZN,etal. Tracheal intubation in patientswithrigidcollarimmobilisationofthecervicalspine:a comparisonofAirtraqandLMACTrachTMdevices.Anaesthesia. 2009;64:1332---6.
8.AvidanMS,HarveyA,ChitkaraN,etal.Theintubatinglaryngeal maskairwaycomparedwithdirectlaryngoscopy.BrJAnesth. 1999;83:615---7.
9.WaltlB,MelischekM,SchuschnigC,etal.Trachealintubation andcervicalspineexcursion:directlaryngoscopyvs.intubating laryngealmask.Anaesthesia.2001;56:221---6.
10.Nileshwar A, Thudamaladinne A. Comparison of intubating laryngealmaskairwayandBullardlaryngoscopefororo-tracheal intubationinadultpatientswithsimulatedlimitationofcervical movements.BrJAnesth.2007;99:292---6.
11.NakazawaK,TanakaN,IshikawaS,etal.UsingtheIntubating LaryngealMaskAirway(LMAFastrachTM)forBlindEndotracheal Intubation in Patients Undergoing Cervical Spine Operation. AnesthAnalg.1999;89:1319---21.
12.KomatsuR,NagataO,KamataK,etal.Theintubatinglaryngeal maskairwayallowstrachealintubationwhenthecervicalspine isimmobilizedbyarigidcollar.Anaesthesia.2004;93:655---9.
13.Bilgin H, Bozkurt M. Tracheal intubation using the ILMA, C-TrachTMorMcCoylaryngoscopeinpatientswithsimulated cervicalspineinjury.Anaesthesia.2006;61:685---91.
14.Bein B, Worthmann F, Scholz F,et al. A comparison of the intubatinglaryngeal mask airway and the Bonfils intubation fibrescopeinpatientswithpredicteddifficultairways. Anaes-thesia.2004;59:668---74.
15.LangeronO, SemjenF,BourgainJL,etal.Comparisonofthe intubatinglaryngealmaskairwaywiththefiberopticintubation in anticipated difficult airway management. Anesthesiology. 2001;94:968---72.
16.Turley A, Latto IP. Cardiff airway management audit. In: ProceedingsofDifficultAirwaySocietyAnnualMeeting.1996.
17.GataurePS,VaughanRS,LattoIP.Simulateddifficultintubation. Comparisonofthegumelasticbougieandthestylet. Anaesthe-sia.1996;51:935---8.
18.KiddJF,DysonA,LattoIP.Successfuldifficultintubation.Useof thegumelasticbougie.Anaesthesia.1988;43:437---8.
19.NolanJP,WilsonME.Anevaluationofthegumelasticbougie. Intubation times and incidence of sore throat. Anaesthesia. 1992;47:878---81.
20.Marfin AG, Pandit JJ, Hames KC, et al. Use of the bougie in simulated difficult intubation. Comparison of sin-gleusebougiewithmultiple-usebougie.Anaesthesia.2003;58: 852---5.
21.HarveyK,DaviesR,EvansA,etal.Acomparisonoftheuseof TrachlightandEschmannmultiple-useintroducerinsimulated difficultintubation.EurJAnaesthesiol.2007;24:76---81.
22.NoguchiT,KogaK,ShigaY,etal.Thegumelasticbougieases trachealintubationwhileapplyingcricoidpressurecompared toastylet.CanJAnesth.2003;50:712---7.
23.Komatsu R,Kamata K,Hoshi I,etal. Airwayscope and gum elasticbougiewithMacintoshlaryngoscopefortracheal intu-bationinpatientswithsimulatedrestrictedneckmobility.BrJ Anaesth.2008;101:863---9.
24.Messa MJ, Kupas DF, Dunham DL. Comparison of bougıe-assıstedıntubatıonwıthtraditionalendotrachealintubationin a sımulated diffıcult airway. Prehosp Emerg Care. 2011;15: 30---3.
25.Mort TC.Emergency trachealintubation:complications asso-ciated withrepeated laryngoscopic attempts. Anesth Analg. 2004;99:607---13.
26.KoscielnyS, GottschallR.Perforation ofthe hypopharynxas ararelifethreateningcomplicationofendotrachealintubation. Anaesthesist.2006;55:45---52.
27.Collins VJ. Principles of anesthesia; endotracheal anesthe-sia complications. 3rd ed. Philedelphia: Lea-Febirger; 1993. p.571---5.
28.Keller C,Brimacombe J,Keller K. Pressures exertedagainst thecervicalvertebraebythestandardandintubatinglaryngeal maskairway.AnesthAnalg.1999;89:1296---300.
29.HamayaY,DohiS.Differencesincardiovascularresponseto air-waystimulationatdifferentsitesandblockadeoftheresponses bylidocaine.Anesthesiology.2000;93:95---103.
30.KiharaS, Brimacombe J, Yaguchi Y. Hemodynamic responses amongthreetrachealintubationdevicesinnormotensiveand hypertensivepatients.AnesthAnalg.2003;96:890---5.
31.BaskettPJF,ParrMJA,NolanP.Theintubatinglaryngealmask. Anaesthesia.1998;53:1174---9.
32.Choyce A, Avidan MS, Harvey A, et al. The cardiovascular responsetoinsertionoftheintubatinglaryngealmaskairway. Anaesthesia.2002;57:330---3.
33.Airwaymanagement.MorganGE,MikhailMS,MurrayMJ,editors. Clinical anesthesiology. 4th ed. International Edition: Lange MedicalBooks;2006.p.504.
34.Takenaka I,Aoyama K, NagaokaE, et al. Malpositionofthe epiglottisaftertrachealintubationviatheintubatinglaryngeal mask.BrJAnesth.1999;83:962---3.
35.BranthwaiteMA.Anunexpectedcomplicationoftheintubating larygealmask.Anaesthesia.1999;54:166---7.
36.CaponasG.Intubatinglaryngealmaskairway(review).Anaesth IntensiveCare.2002;30:551---69.
37.ShungJ,AvidanMS,IngR,etal.Awakeintubationofthedifficult airwaywiththeintubatinglaryngealmaskairway.Anaesthesia. 1999;53:645---9.