r e v b r a s o r t o p . 2017;52(5):625–627
SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Case
Report
Chronic
recurrent
multifocal
osteomyelitis:
a
case
report
夽
Adayellen
Cristina
Salomé
Oliveira
a,
Andrew
Raimundo
Fernandes
da
Costa
a,∗,
Ana
Maria
Magalhães
Valle
Cundari
a,
Vinícius
Bicalho
Rodrigues
baUniversidadedeItaúna,Itaúna,MG,Brazil
bCasadeCaridadeManoelGonc¸alvesdeSousaMoreira,Itaúna,MG,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received5July2016 Accepted25August2016
Availableonline4September2017
Keywords:
Osteomyelitis/pathology Osteomyelitis/diagnosis Diagnosticimaging
a
b
s
t
r
a
c
t
Chronicrecurrentmultifocalosteomyelitis(CRMO)isarareidiopathicinflammatory dis-easethataffectsmainlychildrenandyoungadults.Theclinicalsignsandsymptomsare nonspecific,hinderinganddelayingdiagnosis.Radiologicalandhistopathologicaltestsare essentialforitsdefinition.AcaseofCRMOisreported,demonstratingtheimportanceof clinical,laboratory,andradiologicaldatafordiagnosis.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
Osteomielite
crônica
multifocal
recorrente:
relato
de
caso
Palavras-chave:
Osteomielite/patologia Osteomielite/diagnóstico Diagnósticoporimagem
r
e
s
u
m
o
Osteomielitecrônicamultifocalrecorrente(OCMR)éumadoenc¸ainflamatóriaidiopática raraqueacometeprincipalmentecrianc¸aseadultosjovens.Ossintomasesinaisclínicos sãoinespecíficos,dificultameretardamodiagnóstico.Osexamesradiológicose histopa-tológicossãoindispensáveisparasuadefinic¸ão.Nesterelato,osautoresapresentamum casodeOCMRquedemonstraaimportânciadosdadosclínicos,laboratoriaiseradiológicos paraodiagnóstico.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevierEditora Ltda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
夽
PaperdevelopedatUniversidadedeItaúna,Itaúna,MG,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](A.R.Costa).
http://dx.doi.org/10.1016/j.rboe.2017.08.017
626
rev bras ortop.2017;52(5):625–627Introduction
Chronicrecurrentmultifocalosteomyelitis (CRMO)isarare idiopathic inflammatorydisease,the diagnosis ofwhich is made by exclusion, affecting mainly children and young adults.Theearlyidentificationofthispathologyavoids unnec-essary examinationsand prolonged antibiotictherapy. The clinicalsignsandsymptomsofthediseasearenonspecificand hinderthediagnosisbasedonclinicalpresentationonly.Thus, radiological and histopathologicalexams are indispensable foritsdefinition.
Theobjectiveofthisreportis,therefore,topresentacase ofCRMO,and todemonstratethe diagnosticimportanceof clinical,laboratoryand,mainly,imagingtests.
Case
report
A 44-year-old female patient, who suffered a car accident 12 years before, with no fractures; but had a laceration on the right thigh. After four years, she presented with continuouspainintheleftleg,withnocturnalworsening. Pre-viouslyhealthy,shedeniedafamilyhistoryofmusculoskeletal
conditions, drug reactions, previous surgical history and febrileconditionsaftertheaccident.
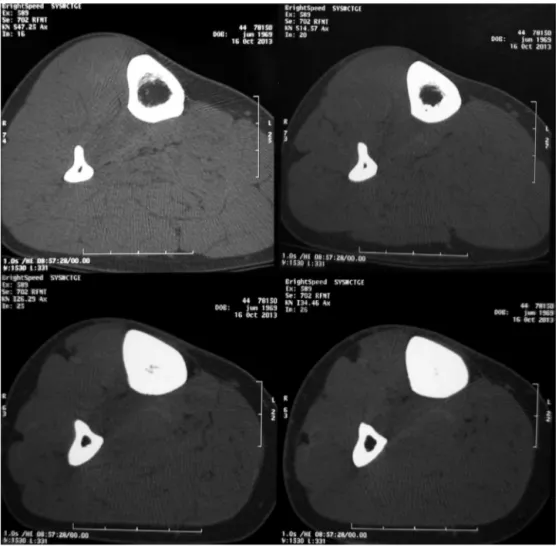
OnSeptember2005,shesoughtmedicalcareand under-went computed tomography (CT) (Fig. 1), which showed corticalthickeninginthelefttibialshaftwithareasofbone resorption. She underwent surgical treatment, progressing withtibialfracture threedaysafterthe procedure,the rea-sonofwhich,accordingtothepatient,wastheremovalofa largebonefragmentduringthesurgicalprocedure.Treatment followed withcastimmobilizationanduseofnon-steroidal anti-inflammatorydrugs(NSAIDs).
OnOctober2013,thepatientsoughtmedicalcarebecause had pain inthe right leg forthree months, similar to the previous onein theleft leg. Imagingand histopathological examswereperformed.Radiographsoftherightlegshowed diffuse corticaland medullary sclerosis at the tibial shaft. ThesechangeswereconfirmedinaCT,whichalsorevealed aminimalareaofboneneoformationwithcortical thicken-ingattheproximalendofthefibula.Surgicalbiopsyshowed anonsepticlesion,andthemedullarycanalwasrecanalized. MDP-Tc99m bonescintigraphydemonstratedhypercaptation
oftheradiopharmaceuticalagentinthemiddlethirdofthe rightleg,withoutdenotingboneinvolvementduetoan infec-tiousprocessorindicatinganyotherasymptomaticfocus.
Fig.1–Axialcomputedtomographyimagesofthemiddlethirdofthelegbonesshaftshowperiostealandendostealbone
rev bras ortop.2017;52(5):625–627
627
TheanalysisoftheexamsallowedthediagnosisofCRMO. Thus,thepatientreceivedNSAIDtherapy,andhasnot pre-sentedanyrecurrenceofpain.
Discussion
CRMO is an idiopathic inflammatory bone disorder seen mainlyinchildrenandadolescents1;however,ithasalready
beendescribedinolderpatientsupto55years.2,3Thisisarare
variantofosteomyelitis,correspondingto2–5%ofthecases.4
Patientsusuallypresentwithinsidiousonsetofheat,pain,and soft-tissueedema,restrictedtooneormorebones.5Thelower
limbsarethemostaffected,5withmetaphysesorequivalent
sitesbeingthemostcommonlocations.6
Itsdiagnosisismadebyexclusion,and themaincauses tobeexcludedareneoplasmsandinfections.7,8Itisbasedon
thefollowingcriteria:(a)bonelesionswithimagessuggesting subacuteorchronicosteomyelitis;(b)unusuallocationwhen comparedtoinfectious,multifocalosteomyelitis;(c)absence ofabscess,fistulaorsequestra;(d)absenceofanetiological agent;(e)nonspecifichistopathologicaland laboratorytests consistentwithsubacuteorchronicosteomyelitis;(f)typical episodesofprolongedandrecurrentepisodesofpain,and(g) occasionalskinmanifestations,suchaspalmoplantar pustu-losis,acne,psoriasisvulgarisandpyodermagangrenosum.9,10
Thepatientpresentedwithalltheabovecriteria,exceptfor cutaneousmanifestations.
Image exams reveal nonspecificalterations that require histopathologicalexams tobetterdefinethe disease.These testsruleoutthepossibilityofneoplasticorinfectiouslesions, whiletheimagesareusefulforassessingtheextentofthe dis-ease,reveallyticareasandperiostealreaction,whichevolveto hyperostosisandsclerosis,exactlywhatthepatient’simages showed(Fig.1).
Treatment involves specially NSAIDsthat aimat symp-tomaticrelief.Antibioticsareconsideredineffective.Thecase patientwastreatedwithNSAIDsandhadgoodprogress,with norecurrenceofpain.
CRMOprogressionisunpredictable.Althoughmostcases resolve spontaneously in months to years, there are
reports of symptomatic patients for up to 25 years after diagnosis.
KnowledgeoftheappearanceofCRMOlesionsandtheir typicalchangesisimportantforanearlydiagnosis,leadingto areductioninthenumberandnecessityofbiopsies,surgeries andantibiotictherapy.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.KhannaG,SatoTS,FergusonP.Imagingofchronicrecurrent multifocalosteomyelitis.Radiographics.2009;29(4): 1159–77.
2.MarinoC,McDonaldE,MegnaD,BrennesselD,ReddyKS,Jain PC.Chronicrecurrentmultifocalosteomyelitisinadult women.NYStateJMed.1992;92(8):360–2.
3.Bj0rksténB,BoquistL.Histopathologicalaspectsofchronic recurrentmultifocalosteomyelitis.JBoneJointSurgBr. 1980;62(3):376–80.
4.GirschickHJ,KrauspeR,TschammlerA,HuppertzHI.Chronic recurrentosteomyelitiswithclavicularinvolvementin children:diagnosticvalueofdifferentimagingtechniques andtherapywithnon-steroidalanti-inflammatorydrugs.Eur JPediatr.1998;157(1):28–33.
5.PaimLB,LiphausBL,RochaAC,CastellanosAL,SilvaCA. Chronicrecurrentmultifocalosteomyelitisofthemandible: reportofthreecases.JPediatr(RioJ).2003;79(5):467–70.
6.MandellGA,ContrerasSJ,ConardK,HarckeHT,MaasKW. Bonescintigraphyinthedetectionofchronicrecurrent multifocalosteomyelitis.JNuclMed.1998;39(10):1778–83.
7.SmithJ,YuppaF,WatsonRC.Primarytumorsandtumor-like lesionsoftheclavicle.SkeletalRadiol.1988;17(4):235–46.
8.StantonRP,Lopez-SosaFH,DoidgeR.Chronicrecurrent multifocalosteomyelitis.OrthopRev.1993;22(2):229–33.
9.SadeghiE,KadivarMR,GhadimiMoghadamAK,PooladfarGR, SadeghiN.Chronicrecurrentmultifocalosteomyelitis:acase report.IranRedCrescentMedJ.2011;13(1):47–51.