REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
PublicaçãoOficialdaSociedadeBrasileiradeAnestesiologiawww.sba.com.br
CLINICAL
INFORMATION
Intraventricular
hemorrhage
after
dural
fistula
embolization
Joana
Chaves
Gonc
¸alves
Rodrigues
de
Carvalho
a,
Francisco
Javier
Tercero
Machin
b,
Luis
San
Roman
Manzanera
c,
Jordi
Blasco
Andaluz
c,
Sílvia
Herrero
Nogués
d,
Núria
Peix
Soriano
d,
Victor
Obach
Baurier
e,
Enrique
Jesus
Carrero
Cardenal
b,∗aUnidadeLocaldeSaúdedeMatosinhos---HospitalPedroHispano,DepartamentodeAnestesiologia,Matosinhos,Portugal bUniversidaddeBarcelona,HospitalClínic,DepartamentodeAnestesiología,Barcelona,Spain
cUniversidaddeBarcelona,HospitalClínic,DepartamentodeNeurorradiologíaIntervencionista(CDI),Barcelona,Spain
dUniversidaddeBarcelona,HospitalClínic,SaladeRecuperaciónPostanestésica,Barcelona,Spain eUniversidaddeBarcelona,HospitalClínic,DepartamentodeNeurología,Barcelona,Spain
Received1June2014;accepted7July2014 Availableonline31October2014
KEYWORDS
Intraventricular hemorrhage; Arteriovenous malformation; Duralfistula; Cerebralperfusion; Cerebraloximetry
Abstract
Backgroundandobjectives: Duralarteriovenousfistulasareanomalousshuntsbetweendural arterialandvenouschannelswhosenidusislocatedbetweentheduralleaflets.Forthose cir-cumstances when invasive treatmentis mandatory, endovascular techniqueshavegrown to becomethemainstayofpractice,choiceattributabletotheirreportedsafetyandeffectiveness. Wedescribetheuniqueandrarecaseofaduralarteriovenousfistulatreatedbytransarterial embolizationandcomplicatedbyanintraventricularhemorrhage.Weaimtoemphasizesome centralaspectsoftheperioperativemanagementofthesepatientsinordertohelpimproving thefutureapproachofsimilarcases.
Casereport: A59-year-oldwomanwithapreviouslydiagnosedCognardTypeIVdural arteriove-nousfistulapresentedfortransarterialembolization,performedoutsidetheoperatingroom, undertotalintravenousanesthesia.Theprocedureunderwentwithoutcomplicationsandthe intraoperativeangiographyrevealedcompleteobliterationofthefistula.Intheearly postopera-tiveperiod,thepatientpresentedwithclinicalsignsofraisedintracranialpressureattributable toalaterdiagnosedintraventricularhemorrhage,whichconditionedplacementofaventricular drain,admissiontoanintensivecareunit,cerebralvasospasmandaprolongedhospitalstay. Throughouttheperioperativeperiod,therewerenochangesinthecerebralbrainoximetry. Thepatientwasdischargedwithoutneurologicalsequelae.
∗Correspondingauthor.
E-mail:[email protected](E.J.CarreroCardenal). http://dx.doi.org/10.1016/j.bjane.2014.07.015
200 J.C.deCarvalhoetal.
Conclusion:Intraventricularhemorrhagemaybeaseriouscomplicationaftertheendovascular treatment ofdural arteriovenousfistula. A closepostoperative surveillance andmonitoring allowanearlydiagnosisandtreatmentwhichincreasestheoddsforanimprovedoutcome. ©2014SociedadeBrasileiradeAnestesiologia.PublishedbyElsevierEditoraLtda.Thisisan openaccessarticleundertheCCBY-NC-NDlicense( http://creativecommons.org/licenses/by-nc-nd/4.0/).
PALAVRAS-CHAVE
Hemorragia intraventricular; Malformac¸ão arteriovenosa; Fístuladural; Perfusãocerebral; Oximetriacerebral
Hemorragiaintraventricularapósembolizac¸ãodefístuladural
Resumo
Justificativaeobjetivos: Fístulas arteriovenosas durais (FAVD) são comunicac¸ões anômalas entre oscanais venosose arteriaisda dura-máter cujo centro estálocalizado entre os fo-lhetosdadura-máter.Paraascircunstânciasnasquaisotratamentoinvasivoéobrigatório,as técnicasendovascularessetornaramospilaresdaprática,escolhaatribuívelarelatosdesua seguranc¸aeeficácia.DescrevemosocasoúnicoerarodeumaFAVDtratadaporembolizac¸ão transarterial(ETA)ecomplicadaporumahemorragiaintraventricular(HIV).Nossoobjetivofoi destacaralgunsaspectos centraisdomanejoperioperatório desses pacientespara ajudara melhorarumafuturaabordagemdecasossemelhantes.
Relatodecaso:Pacientedosexofeminino,59anosdeidade,comdiagnósticopréviodeFAVD tipoIV (Cognard), apresentou-separa ETA, realizada fora dasala decirurgia sob anestesia venosatotal.Oprocedimentotranscorreusemcomplicac¸ões,eaangiografiaintraoperatória revelou obliterac¸ão completa da fístula. No período pós-operatório imediato, a paciente apresentousinaisclínicosdeaumentodapressãointracraniana(PIC)atribuíveisaumaHIV pos-teriormentediagnosticada,oquecondicionouacolocac¸ãodeumdrenoventricular,internac¸ão emUnidadedeTerapiaIntensiva(UTI),vasoespasmocerebraleinternac¸ãohospitalar prolon-gada.Durantetodooperíodoperioperatório,nãohouvealterac¸õesnaoximetriacerebral.A pacienterecebeualtasemsequelasneurológicas.
Conclusão:HIVpodeserumacomplicac¸ãograveapósotratamentoendovasculardeFAVD.A observac¸ãoemonitoramentocuidadososnopós-operatóriopermitemodiagnósticoprecocee otratamentoqueaumentaaschancesdeumresultadomelhor.
©2014SociedadeBrasileiradeAnestesiologia.PublicadoporElsevierEditoraLtda.Este ´eum artigoOpen Accesssobumalicenc¸aCCBY-NC-ND( http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Tentofifteenpercentofallintracranialvascular
malforma-tionsare duralfistulas (DVAF)which representanomalous
shunts amongarterial branchesand dural venous sinuses,
meningealorcorticalveins.1---4Dependingontheirpatternof corticaldrainage,someDAVFmaypresentahighriskof
hem-orrhage,andthereforeshouldbepromptlysealed.3Inthe
last20years,endovasculartherapieshavebecomethe
cor-nerstoneoftreatmentforDVAF.3Nevertheless,theyarenot
innocuousandpatients shouldbeclosely andcontinuously
monitoredfortheappearanceofcomplications.
Wereportthecaseofapatientwhodevelopedan
intra-ventricular hemorrhage (IVH) and acute hydrocephalus in
thepostoperativeperiodofaDAVFembolization.
Case
report
Female, 59 years old, 86kg, BMI 32kgm−2, ASA III, with
apersonalhistoryofarterialhypertension,hypothyroidism
andatrialfibrillation.InNovember2013shehadbeen
sub-mittedtoleftatrialappendageclosureafterwhichshewas
ondoubleantiplatelettherapywithclopidogrelandaspirin
forthreemonths.
On March 2014 she was proposed for transarterial
embolization(TAE)of aDAVFlocatedat thetorcula,
clas-sifiedasCognardTypeIV(Fig.1),afterafirstendovascular
procedurethatdidnotachievecompleteobliteration.
At the pre-anesthetic evaluation the patient did not
presentanyfocalizingneurologicalsign.Shewascurrently
medicatedwithdigoxin, atenolol,enalapril and
acetylsal-icylic acid. Both the laboratory data and complementary
examswerenormalforage.
Onthemorningoftheinterventionthepatientpresented
withaGlasgowComaScore(GCS)of15.Afterperformance
ofasummaryneurologicexam thatonceagainshowedno
deficitsshewaspremedicatedwithmidazolam 1mg
intra-venous(iv).Monitoringconsistedofelectrocardiogram(DII
andV5),pulseoximetry,endtidalcarbondioxide,invasive
blood pressure,central venous pressure,peripheral nerve
stimulator, urinary output, Bispectral Index (BIS) (BISTM,
BrainFunction MonitoringSystem, Covidien,Boulder, USA)
and Near-infraredSpectroscopy (NIRS) (INVOS-4100,
Cere-bral Oximeter, Covidien, Mansfield, MA, USA). Basal NIRS
Figure1 TorcularDAVF.Injectionoftherightvertebralartery(A)andrightcarotidartery(B)inalateralview.Theimagesshow thearterialsupplyofthefistulaarisingfrombranchesoftheexternalcarotidartery,occipitalandmiddlemeningealarteriesaswell asfromtheposteriorcerebralandsuperiorcerebellararteries.Thepatientshowedvenoussinusthrombosisasaprobablecause forfistuladevelopment.ThetorcularDAVF,withitscorticalvenousdrainagepattern,wasgradedasCognardTypeIV.
After preoxygenation, anesthesia was induced using a
Targeted Controlled Infusion of propofol and remifentanil
and iv rocuronium (0.6mgkg−1 bolus followed by a
per-fusion). After insertion of a size 4 i-gel® laryngeal mask
for airway control the patient was ventilated in
volume-controlledmodeadjustedfornormocapnia,withamixture
of50%oxygeninairandapositiveend-expiratorypressure
of5cmH2O.
During anesthetic maintenance, perfusions were
adjusted for the goals of BIS between 40---60 and train-of
four 0/4 with post-tetanic count +, as evaluated by the
peripheral nerve stimulator. The concentrations at the
effectorsite variedbetween 1.5---2.0gmL−1 for propofol
and 2.0---2.5ngmL−1 for remifentanil. Rocuronium was
infusedata0.5mgkg−1h−1rate.
The procedure consisted of complete DAVF TAE with
ethylene-vinylalcohol,formulatedasOnyx®,andit
under-went without ischemic or hemorrhagic incidents (Fig. 2).
Throughitalltherewerenoothercomplications,thepatient
washemodynamicallystable andNIRSvaluesdid notvary
morethan5%comparedtobasal.
Paracetamol1gandondansetron4mgiv were
adminis-teredforanalgesiaandpostoperativenauseaandvomiting
prophylaxis, respectively. At the end of surgery
neuro-muscular blockadewasreversed withsugammadex. When
thepatientwasfullyawakeanewneurologicexamination
was executed and no new deficits were noted. She was
thentransferredtothePostanesthesiaCareUnit(PACU)for
overnightmonitoring.
Shortly afteradmission thepatientcomplainedof pain
onthefemoralpuncturesiteandwasmedicatedwith2mg
ofivmethadone.Twoandahalfhourslatershedeveloped
amoderatehemicranealrightheadacheaccompaniedwith
systemic hypertension (maximal systolic arterial pressure
of190mmHg),twovomitingepisodesanddepressedlevel
ofconsciousness(GCS=13,O3V4M6).Repeated5mgiv
ura-pidilboluses(30mgtotal)wereadministeredtocontrolthe
acutehypertension.NIRSvaluesremainedat 62---64(right)
and72---76(left).
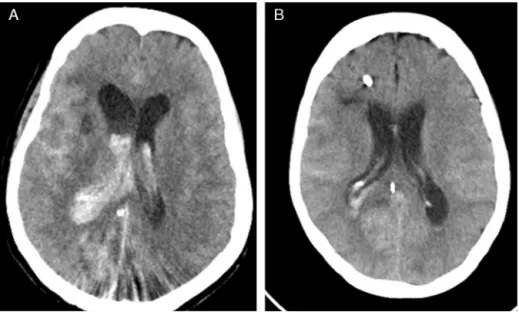
An urgent computed tomography (CT) scan was
per-formed showing an acute hydrocephalus, IVH and diffuse
subarachnoidhemorrhage(Fig.3A).
Shewastakentotheemergencyoperatingroomwherea
ventriculardrainagesystemwasplaced(Fig.3B)andlater wasadmittedtotheintensivecareunit(ICU)sedated,
intu-batedandventilated.Extubationhappenedwithinthefirst
24h postadmissionand shewasdischarged tothegeneral
wardonthe3rdday.
On thefollowing daysa generalizedand asymptomatic
cerebralvasospasmwasdiagnosedby transcranialDoppler
(TCD)butitslowlyrespondedtotherapywiththe
calcium-channel blocker agent nimodipine. The control CT scan
showed IVH resolution but due to persistent dilation of
theventricularsystemthepatientwasscheduledfor
ven-triculoperitonealshuntinsertiononthe22ndpostoperative
day.Intheconvalescenceperiodfromthissecondsurgery,
considering the patient’s clinical and neurological
stabil-ityaswell asherarrhythmia history, antiplatelet therapy
withaspirinwasre-started.Sincetherecoveryunderwent
withoutfurtherincidentsthepatientwasdischargedhome
withnoneurologicdeficitsonemonthaftertheendovascular embolization.
Discussion
DAVF may represent a major source of neurological
mor-bidity and mortality as a result of the occurrence of
adverse clinical events like seizures, hemorrhage or steal
phenomena.5Theincidenceofthesecomplicationsiseven
higherforDAVFwhohave corticalvenous drainage,6asin
thecaseofourpatient.
Overthe past20 years,DAVFsurgeryhasbecome
202 J.C.deCarvalhoetal.
Figure2 Injectionsoftherightvertebralartery(A)andrightcarotid(B)(lateralview),showingtotalfistulaocclusionwiththe Onyx®cast.
practicable.3 In reality DAVF embolization with Onyx®, a
nonadhesive embolic agent composed by ethylene-vinyl
alcohol dissolved in dimethyl-sulfoxide, has grown to
become one of the major approaches to DAVF, which is
intimately linked to its remarkable cure rates and low
morbidity.3,5,6 In fact, there are not many complications
reported after these techniques. Maimon et al. describe
a morbidity of 6% (1/17 patients) related to a transient
trochlear nerve palsy and on a retrospective studied by
Rangel-Castillaetal.,theauthorsdescribeacomplication
rate of 9.7% (7 of 72 patients), of which only one
corre-spondedtoaintraparenchymalhemorrhage.5,6
After a systematic review of the international
litera-ture using the PubMed database, we were not able to
findanyarticle describing the occurrence ofan IVH after
DAVFembolization,whichcorroboratestherelevanceofthis
report.
Individuals medicated with the antiplatelet agent
clo-pidogrel exhibitawidevariability inresponsethat ranges
from hypo-to-hyper responsiveness. When individuals are
submitted to neurointerventional procedures, clopidogrel
hyperresponsivenessseemstobeassociatedwithbleeding
butthedefinitiveclinicalimplicationsofthesedataarestill
underevaluation.7,8Although itisnotknownforhowlong
this‘hyper’responsecanlast,thefactthatourpatienthad
stoppedtheclopidogrelmorethanamonthbeforethe
pro-cedureleadsustobelievethatthiswasnotthemainfactor
behindtheIVH,eventhoughitcouldhaveplayedarolein
itsetiology.
Cerebral hyperperfusion syndrome (CHS), defined as
an excessiveincrease in cerebral blood flow (CBF) into a
previously hypoperfusedareaplus neurologicalsymptoms,
is a potentially life-threatening complication.It iscaused
by exhaustion of the cerebral autoregulation mechanisms
(Normal Perfusion Pressure Breakthrough theory, NPPB)9
anditcanpresentwithfocalneurologicdeficits,headache,
confusion,seizuresorintracerebralhemorrhage.10Although
it hasbeen widely reportedafter carotidendarterectomy
(CEA)11,12andstenting,13itseemstobelesscommon follow-inginterventionsforarteriovenousmalformations(AVMs).14
NIRSisanon-invasiveandobjectivetechnologythat
con-tinuously monitors regionaloxygen saturation (rSO2). Itis
an early predictive marker for critical perfusion changes
during endovascular neuroradiologic interventions.15 Both
Pennekamp et al. and Ogasawara et al. described the
use of this technology as a mean to predict cerebral
hyperperfusion, defined asa ≥100% increase in CBF from
baseline value assessed with single-photon emission CT,
afterCEA.11,12Eventhoughtherearenotclearlydefined
cut-offrSO2 valuesfor cerebralhyperperfusion, theseauthors
showed that an increase as small as three to five
per-centage points with respect to basal values may detect
cerebralhyperperfusionpost-CEAwithahighsensitivityand
specificity (100% and 86.4%, respectively).11,12 Both these
parameters increase to 100% with cut-off points of 10%
variation.12 Whether theconclusions of thesegroup
stud-iescanbeextrapolatedforneurointerventionalprocedures
stillneedstobeestablished.Despitethislackofevidence,
the stability of rSO2 values made usconsider phenomena
other than CHS as the cause behind the patient’s
symp-toms.
The urgent CT scanidentifiedboth theIVH and
hydro-cephalusandgaveus adefinitivediagnosis. The fact that
thebleedingwasrestrictedtotheventriculardrainage sys-temconfirmedourargumentsagainsttheCHS.Youngetal.16
showedthatincreasedCBFfollowingcerebralAVMresection
occursthroughouttheentirebrain,notjustinregionsthat
share the vascular supply withthe malformation.In that
case,rSO2valueswouldhavetohaveincreasedandthatdid
nothappen.NIRStechnologydoes notreflectaglobal
oxy-gensaturation.17 Iftheprobeisplacedintheforehead,as
inourpatient,itismainlymonitoringboththefrontaland
parietalcerebralcortexandthustheterritoriesirrigatedby theanteriorandmiddlecerebralarteries.Thiscouldexplain
whythe rSO2 didnot increaseafter theIVH. Because the
arterialbranchessupplyingtheDAVFarosefromthe
poste-riorcerebralcirculation,we cannotexcludethattheNIRS
monitor could be relatively ‘‘blind’’ to specific perfusion
changes at theseterritories. On the other hand, the fact
thattherSO2valuesdidnotdecreasealsosuggeststhatthe
raisedintracranialpressure(ICP), manifestedasvomiting,
headacheanddiminishedlevelofconsciousness,was
com-pensatedbythesystemicarterialhypertensionanddidnot
leadtoalowercerebralperfusionpressure.
The development of vasospasm, as a response to the
occurrenceofIVHandSAH,isanindicativethatthepatient’s
cerebrovascular reactivity remained unaltered. This fact
arguesagainstthemainprincipleunderlyingtheNPPB
the-oryoftheCHS.9,18
After reviewing the case with the radiology team, it
seemsmorelikelythatthehemorrhagewasprovokedbyone
oftwocauses:iatrogenyrelatedtoamicroperforationwhile retrievingthemicrocatheterusedforarterialcannulationor
hyperpressureinsidetheDAVFafterocclusionofitsvenous
drainage,maybesecondary toanarterialbranchthatmay
haveinadvertentlypersistedopen.
Asstatedearlier,endovasculartechniqueshaveincreased
inpopularitypartlyduetotheirhighsafetyprofile.
Never-theless,whenanomalouseventsoccurtheymaybesevere
and add morbidity, as we can infer from our patient’s
prolonged clinical course. This confirms that in the early
postoperative period after AVM embolization individuals
haveanincreasedriskofneurologicalcomplications.
Howcanwefurtherimprovetheneurologicoutcomeof
thesepatients?Inouropinion,thiscanbedoneby
establish-ingthehighest possible standardsofcare. Admissiontoa
unitwhereaclosefollow-upcanbecarriedonbyaproperly
trainedmedicalandnursingstaffiscrucial.Unlike
unevent-ful unruptured aneurysm embolization,19 complications
after DAVF endovascular treatment may appear several
hourspostprocedure.Forthatreasonandforassuring
bet-tersurveillanceofcerebralfunction,webelievethatthese
patients should stay overnight in high dependency units,
suchasthePACUinourhospital.
A continuous and detailed clinical examination may
swiftlydetect a newneurologicdeficit, a depressedlevel
of consciousness or a change in the GCS, allowing a
promptdiagnosticortherapeuticinterventionthatcan
ulti-mately result in an improved prognosis.20 In some cases,
neuromonitorslikeNIRSandTCD areabletodetect
cere-braldisturbanceseven beforesymptomsbecome evident,
identifying individuals at risk for ischemia21 or cerebral
hyperperfusion22 after neurovascular techniques. In our
case,theneurologicalsymptomswerethekey.NIRShelped
ustoguidethediagnosisandtheTCDdetectedalateand
asymptomaticvasospasm.
Notleastimportantismonitoringthepatient’svitalsigns,
mainly arterial blood pressure. While we could not find
dataspecificallyfocusingonDAVF, Basalietal. showedin
theirretrospectivestudythatpostoperativeelevated
arte-rialpressureisacorrelateforintracerebralbleedingafter
craniotomy.23 On theother hand, aggressivehypertension
treatmentdecreases the risk ofhyperperfusion and
intra-cerebralhemorrhagefollowingcarotidarterystenting.13In
ouropinion thisis also validafter DAVFembolization and
sohypertensioncontrol wasacommonconcern toallthe
elementsinvolvedinourcase.Nevertheless,wethinkthat
the hypertension that our patient developed, more than
acontributivefactortothehemorrhage, wasa secondary
manifestationofraisedICP.
AfterIVHitiscommonforpatientstopresentwith
clin-icalfindings of obstructive hydrocephalus, like depressed
level of consciousness and vomiting, symptoms that our
patient experienced. Even though there are reports of
delayed and transient hydrocephalus that resolves
spon-taneously, when the clinical course is acute, like in our
case, cerebrospinal fluid drainage should be promptly
performed.24
Whenatthegeneralwardofafterhospitaldischargeit
isimportanttokeep aclosesurveillanceof these
individ-uals.Thisistruebecausenon-occludedAVMsorfistulaswith
retrogradecorticaldrainage,liketheoneweherepresent,
areatahighriskforearlyrebleeding.Whenthishappens,
consequencesaremoredevastatingthanatafirstepisode.4
Insummary,anIVHmaybeaseriouscomplicationafter
theendovasculartreatmentofaDAVF.Aclosepostoperative
surveillanceandmonitoringallowforanearlydiagnosisand
204 J.C.deCarvalhoetal.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgments
The authors thank Dr. Robert D. Ecker for providing the
article ‘‘Hyperperfusionsyndromeafterstent/coiling of a
rupturedcarotidbifurcationaneurysm’’(referencenumber
10).
References
1.Ghobrial GM, Marchan E, Nair AK, et al. Dural arteriove-nous fistulas: a review of the literatureand a presentation ofasingleinstitution’sexperience.WorldNeurosurg.2013;80: 94---102.
2.NatarajanSK,GhodkeB,KimLJ,etal.Multimodalitytreatment ofintracranialduralarteriovenousfistulasintheonyxera:a singlecenterexperience.WorldNeurosurg.2010;73:365---79. 3.GandhiD,ChenJ,PearlM,etal.Intracranialdural
arteriove-nous fistulas:classification, imagingfindings,and treatment. AmJNeuroradiol.2012;33:1007---13.
4.DuffauH,LopesM,Janosevic V,etal.Earlyrebleedingfrom intracranialduralarteriovenousfistulas:reportof20casesand reviewoftheliterature.JNeurosurg.1999;90:78---84. 5.MaimonS,Nossek E,StraussI,etal. Transarterialtreatment
withonyxofintracranialduralarteriovenousfistulawith corti-caldrainagein17patients.AmJNeuroradiol.2011;32:2180---4. 6.Rangel-CastillaL, BarberSM,Klucznik R,etal. Midand long term outcomes of dural arteriovenous fistula endovascular managementwithOnyx.Experienceofasingletertiarycenter. JNeurointervSurg.2014:607---13.
7.Serebruany VL, SteinhublSR, Berger PB,et al.Variability in platelet responsivenesstoclopidogrelamong544individuals. JAmCollCardiol.2005;45:246---51.
8.GohC,ChurilovL,MitchellP,etal.Clopidogrelhyper-response andbleedingriskinneurointerventionalprocedures.AmJ Neu-roradiol.2013;34:721---6.
9.Spetzler RF, WilsonCB, Weinstein P,et al.Normal perfusion pressurebreakthroughtheory.ClinNeurosurg.1978;25:651---72. 10.EckerRD,MurrayRD,SederDB.Hyperperfusionsyndromeafter stent/coilingofarupturedcarotidbifurcationaneurysm. Neu-rocritCare.2013;18:54---8.
11.PennekampCWA,ImminkRV,RuijterHM,etal.Near-infrared spectroscopy can predict the onset of cerebral hyperperfu-sionsyndromeaftercarotidendarterectomy.CerebrovascDis. 2012;34:314---21.
12.Ogasawara K, Konno H, Yukawa H, et al. Transcranial regionalcerebraloxygensaturationmonitoringduringcarotid endarterectomyasapredictorofpostoperativehyperperfusion. Neurosurgery.2003;53:309---15.
13.Abou-CheblA,YadavJS,ReginelliJP,etal.Intracranial hem-orrhageandhyperperfusionsyndromefollowingcarotidartery stenting:risk factors,prevention, and treatment.J AmColl Cardiol.2004;43:1596---601.
14.PicardL,DaCostaE,AnxionnatR,etal.Acutespontaneous hem-orrhageafterembolizationofbrainarteriovenousmalformation withN-butylcyanoacrylate.JNeuroradiol.2001;28:147---65. 15.RummelC,ZublerC,SchrothG,etal.Monitoringcerebral
oxy-genation during balloon occlusionwithmultichannel NIRS. J CerebBloodFlowMetab.2014;34:347---56.
16.Young WL, Kader A, Ornstein E, et al. Cerebral hyper-emia after arteriovenous malformation resection is related to ‘‘breakthrough’’ complications but notto feeding artery pressure.TheColumbiaUniversityArteriovenousMalformation StudyProject.Neurosurgery.1996;38:1085---93.
17.GhoshA,ElwellC,SmithM.Cerebralnear-infraredspectroscopy inadults:aworkinprogress.AnesthAnalg.2012;115:1373---83. 18.Alexander MD, Connolly ES, Meyers PM. Revisiting nor-malperfusion pressure breakthrough in light of hemorrhage induced-vasospasm.WorldJRadiol.2010;2:230---2.
19.BurrowsAM,RabinsteinAA,CloftHJ,etal.Areroutine inten-sivecare admissionsneededafterendovasculartreatmentof unrupturedaneurysms?AmJNeuroradiol.2013;34:2199---201. 20.FabregasN,BruderN. Recoveryandneurologicalevaluation.
BestPractResClinAnaesthesiol.2007;21:431---47.
21.MarshallSA,NyquistP,ZiaiWC.TheroleoftranscranialDoppler ultrasonographyinthediagnosisandmanagementofvasospasm afteraneurysmalsubarachnoidhemorrhage.NeurosurgClinN Am.2010;21:291---303.
22.Pennekamp CW, Moll FL, De Borst GJ. Role of transcranial Dopplerincerebralhyperperfusionsyndrome.JCardiovascSurg (Torino).2012;53:765---71.
23.BasaliA, MaschaEJ,KalfasI.Relationbetween perioperative hypertension and intracranial hemorrhage after craniotomy. Anesthesiology.2000;93:48---54.