RevBrasAnestesiol.2016;66(2):215---218
REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
OfficialPublicationoftheBrazilianSocietyofAnesthesiologywww.sba.com.br
CLINICAL
INFORMATION
Anesthetic
management
of
a
large
mediastinal
mass
for
tracheal
stent
placement
Suman
Rajagopalan
a,∗,
Mark
Harbott
a,
Jaime
Ortiz
a,
Venkata
Bandi
baDepartmentofAnesthesiology,BaylorCollegeofMedicine,Houston,UnitedStates
bDepartmentofPulmonologyandMedicine,BaylorCollegeofMedicine,Houston,UnitedStates
Received23December2013;accepted15January2014 Availableonline20February2014
KEYWORDS
Anesthetic management; Mediastinalmass; Laryngealmask airway; Trachealstent
Abstract Theanestheticmanagementofpatientswithlargemediastinalmassescanbe com-plicatedduetothepressureeffectsofthemassontheairwayormajorvessels.Wepresent thesuccessfulanestheticmanagementofa64-year-oldfemalewithalargemediastinalmass thatencroachedonthegreatvesselsandcompressedthetrachea.Atrachealstentwasplaced to relieve thetracheal compression undergeneral anesthesia.Spontaneous ventilationwas maintainedduringtheperioperativeperiodwiththeuseofaclassiclaryngealmaskairway.We discusstheutilityoflaryngealmaskairwayforanestheticmanagementoftrachealstentingin patientswithmediastinalmasses.
© 2014SociedadeBrasileirade Anestesiologia.Publishedby ElsevierEditoraLtda.Allrights reserved.
PALAVRAS-CHAVE
Anestesia; Doenc¸asdo Mediastino; Máscaraslaríngeas;
Stents
Manejoanestésicodegrandemassamediastinalparaacolocac¸ãodestenttraqueal
Resumo Omanejoanestésicodepacientescomgrandesmassassituadasnomediastinopode sercomplicadoporcausadosefeitosdapressãodamassasobreasviasaéreasougrandesvasos. Relatamos omanejoanestésicobem-sucedido deuma pacientede64anoscomumagrande massamediastinalqueinvadiuosgrandesvasosecomprimiuatraqueia.Umstenttraquealfoi colocadoparaaliviaracompressãodatraqueia,sobanestesiageral.Aventilac¸ãoespontânea foi mantidaduranteoperíodo perioperatório comousode umamáscara laríngeaclássica. Discutimosautilidadedamáscaralaríngeaparaomanejodacolocac¸ãodestenttraquealem pacientescommassassituadasnomediastino.
©2014SociedadeBrasileira deAnestesiologia.PublicadoporElsevierEditoraLtda.Todosos direitosreservados.
∗Correspondingauthor.
E-mail:[email protected](S.Rajagopalan).
Introduction
Mediastinaltumorsthatarelargeenoughtocause compres-sionof airway or major vesselspose a significant risk for
216 S.Rajagopalanetal.
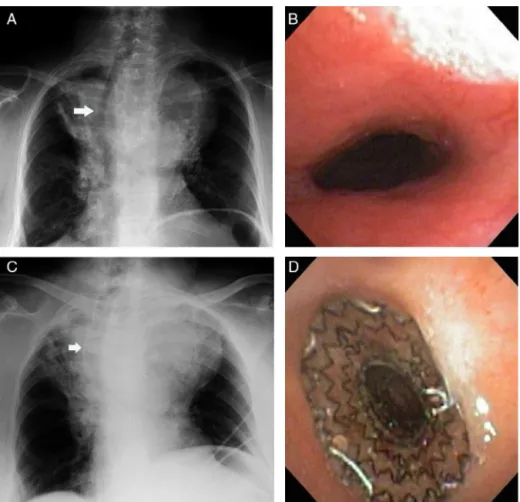
Figure1 (A) ChestX-rayshowing alargemediastinalmasswith markeddeviation ofthetrachea tothe rightwith tracheal compression,(B)bronchoscopicviewofthetracheashowingthenarrowing,(C)chestX-rayafterthestentplacementshowingthe stentinthetrachea,and(D)bronchoscopicviewofthetrachealstent.
cardiopulmonarycomplications.Catastrophichypoxia, vas-cular complications and cardiac arrest can occur during the perioperative periodand have been reported in both theadult1 andpediatricpopulations.2,3Further,theuseof muscle relaxants and positive pressure ventilation during generalanesthesiahas been associatedwith an increased riskof airwaycollapse.4We reportthegeneralanesthetic managementofapatientwhounderwenttrachealstenting foralargemediastinaltumorwhilemaintainingspontaneous ventilationwithalaryngealmaskairway(LMA).
Clinical
report
A 64-year-old female with a medical history remarkable for hypertension and asthma was diagnosed with a sar-comatoid carcinoma of the lung. This tumor measuring 9.3cm×9.0cm×11.7cmencroachedontheanterior
medi-astinum. Due to the advanced stage of the cancer, she was considered a poor surgical candidate. She received chemotherapy with adriamycin, ifosfamide and mesna in conjunction with radiotherapy. She remained relatively asymptomatic after therapy for a periodof 5 yearsafter whichshepresented touswithworseningdyspnea,cough andhoarseness of voice of one month duration.The dys-pnea wasworst onlying flat than in the semi-recumbent position.ThechestX-rayrevealedalargemediastinalmass
withmarkeddeviationofthetracheatotherightwith tra-chealcompression(Fig.1A).TheCTscanconfirmedthatthe mediastinalmasshadincreasedinsizeand,nowmeasured 10.3cm×10.4cm×12.7cm.Itencroachedonthegreat
ves-sels andtrachea, causing significant trachealcompression and deviation (Fig. 2). As the predominant symptom was
Figure2 CTscanshowing thelargemediastinalmass mea-suring 10.3cm×10.4cm×12.7cm encroaching on the great
Mediastinalmassfortrachealstentplacement 217
dyspnea due to the obstruction of the trachea, she was scheduled for theplacementof atracheal stentasa pal-liativemeasuretorelievetheairwayobstruction.
On the day of the procedure, a large bore peripheral intravenous line and a right radial arterial access were established.General anesthesiawhile maintaining sponta-neousventilationwithaLMAwasplanned.Rigidfiberoptic bronchoscopesweremadeavailableasaback-up interven-tionin the event of tracheal collapseduring induction of anesthesia. The cardiopulmonary bypassteamwas placed onstand-byinthe eventthatsignificant cardiorespiratory decompensationwastooccurandwe wereunableto res-cue with the rigid bronchoscopes. In the semi-recumbent position,generalanesthesiawasinduced with70% nitrous oxideinoxygenandsevoflurane.Oninductionofanesthesia, nitrous oxide wasdiscontinued and anesthesia was main-tained withsevoflurane in 100% oxygen. Withthe patient breathing spontaneously, bronchoscopy was performed to assess the feasibility of placing a self-expanding metallic trachealstent.Asize5classicLMAwasplacedtomaintain spontaneous respiration. Neuromuscular blocking agents andpositivepressureventilation wereavoided.Therewas largeairleakwiththepassageofbronchoscopesthroughthe LMAandwewereunabletomaintaingoodsevoflurane con-centrationsnecessaryfortheprocedure.Hence,wedecided tosupplementitwithpropofolinfusionatsedativedoseof 25---50mcg/kg/min. With this small dose of propofol, we could maintain spontaneous respiration and achieve ade-quate depth of anesthesia required for stent placement. An 18mm×60mm self-expanding metallic tracheal stent
was deployed through the LMA (Fig. 1D) with immediate improvement in the tidalvolumes. The LMA was success-fullyremovedattheendoftheprocedureandthepatient recoveredinthepostanesthesiacareunituneventfully.
Discussion
Mediastinalmassesareknowntobeassociatedwith signifi-cantmorbidityandmortalityduetotheanatomicalrelation of the mass with important structures within the thorax. Thecardiorespiratorycompromiseresultingfromthemass collapsing on the trachea, cardiac chambers, pulmonary veins or the superior vena cava could have devastating outcomes.Patientspresentingwithsymptomsof dyspnea, cough, hoarseness, stridor, postural symptoms, superior vena cava syndrome or evidence of tracheal compression ofmorethan50%asassessedbyCTscans,areatahigher riskforcardiopulmonarycollapse.4Thepresenceof pericar-dialeffusionwasfoundtobeanindependentriskfactorfor complications.2Anindividualizedanestheticplanshouldbe formulatedfor eachpatientpresentingwithamediastinal massbasedontheclinicalandradiological features. Gen-eral anesthesia is best avoided in such high-risk patients when possible. If general anesthesia is absolutely neces-sary, maintaining spontaneous respiration would preserve the normal transpulmonary pressuregradient that aidsin keepingtheairwaydistendedandpatent,thus preventing airwaycollapse.5
Patientswithintrathoracictumorsarefrequentlyseenin theperioperativeperiodforavarietyofprocedures requir-inganesthesia. Theuse ofmetallicself-expandablestents
as a palliative measure for relieving airway obstruction due to compression by tumors has increased significantly in the recent past. Anesthesia for tracheal stent place-menthasbeenwelldescribedbyBrodsky.6Trachealstents arepreferablyplaced under general anesthesiaasit pro-vides an immobile patient with good visualization of the airway for stent placement. Airway management can be achieved with an endotracheal tube, rigid bronchoscopy withjetventilationoraLMA.7,8Sarkissetal.describethe successfuluseoftheLMAinpatientspresentingfor interven-tionalpulmonology.9Evenpatientswithmassivemediastinal masses have undergone successful procedures with LMA placement.10
Inourcase,thepatientwasnotonlysymptomatic,but alsodemonstrated tracheal narrowing starting just below thelarynxontheCTscan. Duringtheanestheticplanning ofourpatient,thepossibilityof cardiorespiratory decom-pensation could not be underestimated. Our patient had subglotticcompressionofthetracheaandthestent place-mentthroughanendotrachealtubeorarigidbronchoscope would have been difficult.7 Hence, a LMA was preferred fortheplacementoftrachealstentfromthesurgicalstand point.The largeinternal diameteroftheLMA allowseasy passageof the stent loader withthe stent without inter-ruptionof ventilation.A classic LMAwas chosenas ithas aperture bars instead of theepiglottic elevator bars that alloweasypassageofbronchoscopeandstents.Ourmajor concernwiththe use of LMA in this patientwasthat the airway was not secure and there wasstill the possibility of tracheal compression by the tumor which could result insignificantdifficultywithventilation.Intheeventof air-waycollapse,theplanwastostenttheairwayopenwitha rigidbronchoscope.Thecardiopulmonarybypassteamwas onstandby asa last resort in case of emergentsituation althoughitwouldhavebeendifficulttogainfemoralaccess andgoonpumpinatimelymanner.11
Conclusion
Inconclusion,LMAcouldbeusedtoprovidesufficient anes-theticdepthfortrachealstentplacementinpatientswith massive mediastinal mass while maintaining spontaneous ventilation. However in these patients, a backup plan to rescue the airwayshould be made available in the event ofairwaycompromise.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.NeumanGG,WeingartenAE,AbramowitzRM,etal.The anes-theticmanagementofthepatientwithananteriormediastinal mass.Anesthesiology.1984;60:144---7.
2.BechardP,LétourneauL, LacasseY, etal.Perioperative car-diorespiratorycomplicationsinadultswithmediastinalmass: incidenceandriskfactors.Anesthesiology.2004;100:826---34. 3.StrickerPA,GurnaneyHG,LitmanRS.Anestheticmanagement
218 S.Rajagopalanetal.
4.ErdosG,TzanovaI.Perioperativeanaestheticmanagementof mediastinalmassinadults.EurJAnaesthesiol.2009;26:627---32. 5.BlankRS,deSouzaDG.Anestheticmanagementofpatientswith ananteriormediastinalmass:continuingprofessional develop-ment.CanJAnaesth.2011;58:860---7,853---9.
6.BrodskyJB.Anesthesiaforpulmonarystentinsertion.CurrOpin Anaesthesiol.2003;16:65---7.
7.Okada S, Ishimori S, Yamagata S, et al. Placement of self-expandable metallic stents with a laryngeal mask and a fiberoptic flexible bronchoscope for obstructive tracheo-bronchiallesions.JThoracCardiovascSurg.2002;124:1032---4. 8.Obeidat S, Badin S, KhawajaI. A newtechnique of deploy-ing dynamic y stent using flexible bronchoscope, video
laryngoscope,andlaryngealmaskairway.JBroncholInterv Pul-monol.2010;17:171---3.
9.SarkissM.Anesthesiaforbronchoscopyandinterventional pul-monology:frommoderatesedationtojetventilation.CurrOpin PulmMed.2011;17:274---8.