REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
OfficialPublicationoftheBrazilianSocietyofAnesthesiologywww.sba.com.br
SCIENTIFIC
ARTICLE
Correlation
between
oro
and
hypopharynx
shape
and
position
with
endotracheal
intubation
difficulty
Daher
Rabadi
a,∗,
Ahmad
Abu
Baker
a,
Mohannad
Al-Qudah
baDepartmentofAnesthesiology,JordanUniversityofScience&Technology,Irbid,Jordan bDepartmentofSpecialSurgery,JordanUniversityofScience&Technology,Irbid,Jordan
Received4July2013;accepted15August2013 Availableonline29October2013
KEYWORDS
Intubation; Airway; Pharynx; Classification; Correlation; Value
Abstract
Backgroundandobjective: Predictionofintubationdifficultycansavepatientsfrommajor pre-operativemorbidityormortality.Thepurposeofthispaperistoassessthecorrelationbetween oro---hypopharynxposition,necksize,andlengthwithendotrachealintubationdifficulty.The studyalsoexploredthediagnosticvalueofFriedmanStagingSysteminpredictioncaseswith difficultintubation.
Method: Theconsecutive500ASA(I,II)adultpatientsundergoingelectivesurgerywere evalu-atedfororoandhypopharynxshapeandpositionbymodifiedMallampati,CormackandLehane scoreaswellasFriedmanobstructivesleepapneaclassificationsystems.Neckcircumference andlengthwerealsomeasured.Allcaseswereintubatedbyasingleanesthesiologistwhowas uninformedoftheaboveevaluationandgradedintubationdifficultyinvisualanalogscore. Cor-relationbetweenthesefindingsanddifficultyofintubationwasassessed.Sensitivity,Specificity, PositiveandNegativePredictiveValueswerealsoreported.
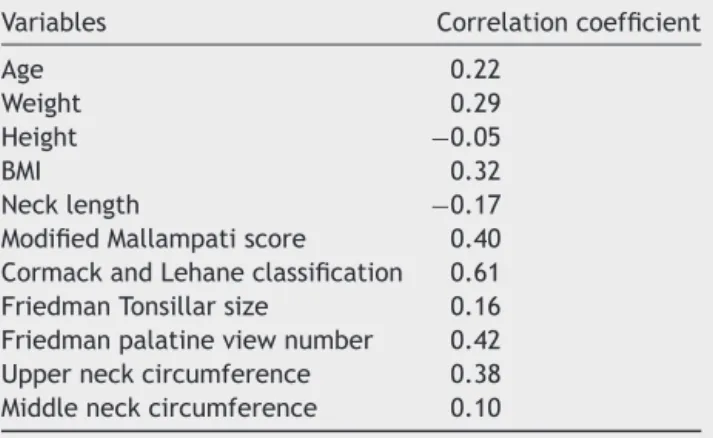
Results:Cormack---Lehane grade had the strongest correlation with difficulty of intubation followed by Friedmanpalate position.Friedmanpalate positionwas themostsensitiveand had higherpositive andnegative predictivevalues thanmodified Mallampaticlassification. Cormack---Lehanegradewasfoundtobethemostspecificwiththehighestnegativepredictive valueamongthefourstudiedclassifications.
Conclusion: Friedmanpalatepositionisamoreuseful,valuableandsensitivetestcompared tothemodifiedMallampatiscreeningtestforpre-anestheticpredictionofdifficultintubation where itsinvolvementinMultivariatemodelmay raisetheaccuracyanddiagnosticvalue of preoperativeassessmentofdifficultairway.
© 2013SociedadeBrasileirade Anestesiologia.Publishedby ElsevierEditoraLtda.Allrights reserved.
∗Correspondingauthor.
E-mail:[email protected](D.Rabadi).
0104-0014/$–seefrontmatter©2013SociedadeBrasileiradeAnestesiologia.PublishedbyElsevierEditoraLtda.Allrightsreserved.
PALAVRAS-CHAVE
Intubac¸ão; Viasaéreas; Faringe; Classificac¸ão; Correlac¸ão; Valor
Correlac¸ãoentreosformatosdaorofaringeehipofaringeeposicionamentoem intubac¸ãoendotraquealdifícil
Resumo
Justificativaeobjetivo:Aprevisãodeintubac¸ãodifícilnoperíodopré-operatóriopodesalvar pacientesdemorbidadeemortalidadegraves.Oobjetivodesteestudofoiavaliaracorrelac¸ão entreintubac¸ão endotraquealdifícilea posic¸ão oro-hipofaríngea,circunferência e compri-mentodopescoc¸o.OestudotambémavaliouovalordiagnósticodoSistemadeClassificac¸ãode Friedmanparaprevercasosdeintubac¸ãodifícil.
Método: Avaliamosconsecutivamenteoformatooro-hipofaríngeoeaposic¸ãode500pacientes adultos (ASAI-II)submetidos àcirurgia eletiva, usandooescorede Mallampatimodificado, escoredeCormackeLehane,bemcomoosistemadeclassificac¸ãodeFriedmanparaapneia obstrutivadosono.Acircunferênciaecomprimentodopescoc¸otambémforammensurados. Todososcasosforamintubadosporumúnicoanestesiologistaquedesconheciaoestudoe clas-sificouaintubac¸ãodifícilemescalavisualanalógica.Acorrelac¸ãoentreosachadoseintubac¸ão difícilfoiavaliada.Sensibilidade,especificidadeevalorespreditivospositivosenegativos tam-bémforamregistrados.
Resultados: Aclassificac¸ãoem grausdeCormackeLehaneapresentou umacorrelac¸ãomais forte comintubac¸ão difícil,seguidapela posic¸ão palatalde Friedman.A posic¸ãopalatalde Friedmanfoiamaissensíveleapresentouvalorespreditivos positivosenegativosmaisaltos queaescaladeMallampatimodificada.Descobrimos queograudeCormackeLehanefoio maisespecífico eapresentouomaiorvalorpreditivo negativoentreasquatro classificac¸ões estudadas.
Conclusão:Aposic¸ãopalataldeFriedmanéumtestemaisútil,valiosoesensívelcomparado aotestemodificadodetriagemdeMallampatiparapreverintubac¸ãodifícilpré-anestesiaeo seuenvolvimentonomodelomultivariadopodeaumentaraprecisãoeovalordiagnósticoda avaliac¸ãopré-operatóriadeviaaéreadifícil.
©2013SociedadeBrasileiradeAnestesiologia.PublicadoporElsevierEditoraLtda.Todosos direitosreservados.
Introduction
Successfulintubationandsecuringairwayrequiresleveling theoropharynxcavityin linewiththe pharyngeolaryngeal structures.This isdone toallow goodvisualization ofthe vocalcordsandsupraglotticarea.
Several studies have focused on one or more
patient-relatedfactorsandproposedanatomicalstructuregrading classifications to predict difficult tracheal intubation.
Amongthese,the modifiedMallampati scoreand the
Cor-mack and Lehane classification are commonly used by
anesthesiologisttoevaluateairwaydifficulty.
Results of studies evaluating the correlation between
theseclassifications and the ease tointubate are contro-versial.In arecent meta-analysis,Lundstrøm etal.found thatthemodifiedMallampatiscoreisinadequateasa stand-alonetestofadifficultlaryngoscopyortrachealintubation.
Theirrecommendationwasthedevelopmentof
multivari-atemodeltopredictdifficultintubationindailyanesthetic practice.1 Shigaetal.conducteda meta-analysisstudy to systematically determine the diagnostic accuracy of bed-sidetestsforpredictingdifficultintubationinpatientswith noairwaypathology.The conclusionofthisstudywasthat the current available screening tests for difficult intuba-tionhadonlypoortomoderatediscriminativepowerwhen used alone. Combinations of tests add some incremental diagnostic value in comparison to the value of each test alone.2
Theresultsofthesestudiescouldbehardtointerpretby themethodsusedintheirconduction,since,theriskfactors studied were analyzed by many investigators or the intu-bationwasperformedbymorethanoneanesthesiologists. Also,thedegree ofintubationdifficultywasassessedasa cutpointdifficult ornotusingdirectlaryngoscopyviewor miscellaneousmultifactorialindices.
Tonsils,softpalateandbaseoftonguearemajor compo-nentsintheoroandhypopharynx.Theirprominenceorlaxity mayaffecttheoropharynxsizeanddeeperstructures visu-alization.Alsoshortandfatneckhadbeenassociatedwith difficultventilationandintubation.Infact,thesestructures are commonly cited ascauses of obstructive sleep apnea (OSA) syndrome. Friedmanet al. had validated a staging systemusingthesizeofthetonsilandthepositionofsoft palateandbaseoftonguetopredictsubjectiveand objec-tiveimprovementafterOSAtreatment.3,4Moreover,Liistro etal.studiedtheassociationbetweenMallampatiscoreand OSA.Theyfoundsignificantcorrelationbetweenthe Mallam-patiscore andapnea/hypopnea indexand concludedthat a high Mallampati score represents a predisposing factor for OSA syndrome.5 To our best knowledge, the correla-tionbetweenFriedmanStagingSystemandthedifficultyof intubationhasnotbeenstudiedbefore.
Method
TheconsecutiveASA(I,II)adultpatientsundergoingelective surgerybetweenApril andJuly 2012wereenrolledin this study.Pregnant,facialtraumaorfacialabnormality,cervical spinedisorders,upperairwayobstructedpathologyaswell aspatientswithknownhistoryofdifficult intubationwere excluded.
At preoperative assessment area,allpatients had gen-eralmedicalexaminationandassessment for pharynxand neck size by single trainedinvestigator. The pharynx size was assessed using modified Mallampati as well as Fried-manpalatepositionandtonsillarsizescoringsystem.3The necklengthwasmeasuredbetweentwobonypoints: mas-toid process and ipsilateral suprasternal notch. The neck circumferencewasmeasuredattwolevels:Upper-neck(the levelofhyoidbone)andMid-neck(thelevelofcricothyroid membrane).
Allpatientswereintubatedbythefirstauthor,whowas blindedto theabove measurements, ina standard induc-tionprotocolincludingmusclerelaxationwithdifferentsizes curvedbladeMacintoshlaryngoscope.Thedifficultyof intu-bation was scaled using visual analog score (VAS) ranging from0to10with10beingverydifficultintubation.Attime ofintubationCormackandLehanelaryngoscopicgrading sys-temwasdocumented.
For the purpose of calculating sensitivity, specificity, andpositiveandnegativepredictivevalues,weconsidered patientswithmorethanfourVASasdifficultintubatedcases. Hospital ethical committee had approvedour research protocoland asignedconsentformwasobtainedfromall patients.
Pearsoncorrelationcoefficientwasusedforthe statisti-calanalysis.Categoricaldatawereanalyzedbychisquare testorFisher’sexacttest,asappropriate.Apvalueof<0.05 wasacceptedasstatisticallysignificant.
Results
500 consecutive patients were included in this study. Patients’characteristicsandsummaryofthetestedresults are reported in Table 1. Table 2 presents the Pearson correlation coefficient between the difficulty of intuba-tion and different studied risk factors. Cormack---Lehane grade had the strongest association followed by Fried-man palate position and modified Mallampati score. Mid neck circumference had the weakest correlation. Fried-manpalatepositionwasthemostsensitiveandhadhigher positiveandnegativepredictivevaluesthanmodified Mal-lampaticlassification,whereasCormackandLehanescoring was the most specific with the highest predictive val-ues among the four studied classifications as shown in Table3.
Discussion
Modernchangesinanesthesiamedications,equipmentand monitors have allowed safe anesthesia practice and out-come; however,unexpected difficult intubatedcaseswith serious reported complications are still challenges in the dailyanesthesiaexperience.
Table1 Patientsdemographicsandcharacteristics.
Age
Average41.43
Standerdeviation(14.75) Gender:
Male:223 Female:277 Weight(kg)
Average79
Standerdeviation(17) Bodymassindex
Average28
Standerdeviation(6) Typeofsurgery
Generalsurgery:230 Orthopedic:109 Gynecology:68 Otolaryngology:59 Urology:34
DegreeofIntubationdifficulty: Average:2.7
Standerdeviation(1.2) Friedmanpalateposition
Average:2.2
Standerdeviation(0.6) Friedmantonsillarsize
Average:1.6
Standerdeviation(0.9) ModifiedMallampatiscore
Average:2
Standerdeviation(0.7)
CormackandLehaneclassification Average:1.8
Standerdeviation(0.7) Upperneckcircumference(cm)
Average:43
Standerdeviation(2.8) Middleneckcircumference(cm)
Average:41
Standerdeviation(2) Necklength(cm)
Average:16.7
Standerdeviation(1.6)
Table2 Correlationcoefficientbetweendifferentstudied variablesanddifficultyofintubation.
Variables Correlationcoefficient
Age 0.22
Weight 0.29
Height −0.05
BMI 0.32
Necklength −0.17
Table3 Sensitivity,specificity,positiveandnegativepredictivevaluesofthefourstudiedclassificationsystems.
ClassificationSystem Sensitivity Specificity Positivepredictive value
Negative predictivevalue
Association withdifficult intubation(p)
ModifiedMallampatiscore3and4 0.47 0.91 0.57 0.86 <0.0001
CormackandLehanescore3and4 0.34 0.95 0.67 0.95 <0.0001
Friedman’stonsillarsize3and4 0.37 0.89 0.47 0.83 <0.0001
Friedman’spalateposition3and4 0.59 0.87 0.60 0.87 <0.0001
In a recent audit of the four royal colleges of
anes-thesiasocieties,themortalityrateassociatedwithairway
managementwasoneper22,000generalanesthetics,brain
damageonein 180,000anesthetics, intensive care
admis-siononein 29,000, andemergencysurgical airway onein
50,000 general anesthetics.6 Rose and Cohen studied the
methods,riskfactorsandoutcomesofairwaymanagement in18,205patients.Mortalityindifficultintubatedcaseswas notcommonbutincludeddesaturationandhypertensionon induction,esophagealintubation,anddentalinjury.These patientsalsohadahigherrateofunexpectedintensivecare unitadmissionandlongerlengthsofhospitalstay.7
Becauseofthesepotentialseriouscomplications associ-atedwithfailedintubation,researchershadtriedtoidentify preoperativefactors thatcouldpredict difficult intubated cases.Mallampatiandco-workersin1985proposedagrading systembased ontheability tovisualize pharyngeal struc-turesandcorrelate thiswithtrachealintubationdifficulty in210patients.Thedegreeofdifficultyinvisualizingthese structureswasanaccuratepredictorofdirectlaryngoscopy difficulty withsensitivity of 50% andspecificity of 100%.8 However,subsequentlargerstudieshave shownonly mod-est degrees of accuracy using the original and even the modified versions of the test.9 Additionally, the accuracy of these tests was found to vary with gender and ethnic variations.10---12 Becauseitisunlikelythatasingle anatomi-calparametercouldaccuratelypredictintubationdifficulty, severalmultivariatemodelsweredeveloped.Thesemodels included different anatomical measurements at different levelintheairway,neckandjawmovement, age,gender, pathologyin upper airway andsome other factors. These models provide more sensitive and specific date for pre-diction of unanticipated difficult tracheal intubation.13---16 AlthoughmodifiedMallampatiandFreidmanpalateposition scalesareverysimilar,amajordifferencebetweenthemis theconditionofthetongue.Intheclassicandall Mallam-patimodifications, the oropharynxis examined while the tongueisprotrudedwhereasinFreidmanclassificationitis not.Infact,duringdirectlaryngoscopyandintubation,the tonguepositioninthepharynxismorelikelytobeinthe non-protruded location. The results of study showed stronger correlationbetweenFreidmanclassificationandintubation difficultythanmodifiedMallampatiscale.
Inmostpublishedstudies,difficultlaryngoscopyhasbeen definedasaviewofthelarynxcorrespondingtograde3or4 intheclassificationbyCormackandLehaneorbyadapting theAmericanSocietyofAnesthesiologistsdefinition.17 This approachcausesthedivisionofstudiedpatientsintofixed and limited outcome subgroups. In this study, continuous scale(VAS)hasbeenusedtoassessdifficultyofintubation
andwasgradedbyanexperiencedanesthesiologistwhowas blindedtopatients’studiedriskfactors.
Sensitivityandspecificityaredependentparameterswith negative correlation. When the sensitivity increases, the specificity usuallydecreases andvice versa. The preanes-theticevaluationoftheairwayshouldbemainlyaimedat identifyingasmanypatientswithdifficultintubationto min-imizetheriskofunanticipateddifficult/failedintubation.14 Fromthisperspective,thesensitivityofatestmaybeamore valuableparameterforpredictiondifficultintubationthan itsspecificity.
Although Cormackand Lehane score were found tobe the most specific and had the highest positive and nega-tivepredictivevalues,itsclinicalsignificanceinpredicting pre-anesthetic difficult intubatedcasesmay belatesince this classificationis evaluatedwhile the patienthasbeen paralyzed.
In this prospective single blinded study, identification of the correlation between anatomical size and shape of thepharynxaswellasthe necklengthandcircumference withthedifficultyof intubationhasbeen considered.The studyshowedtheFriedmanclassificationtobesuperiorto modifiedMallampatiscaleinpredictingdifficultyofairway intubation. However, more studies with larger number of patientsareneededtoproperlyevaluatethevalueofthis classificationintheanesthesiologyfield.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.Lundstrøm LH, Vester-Andersen M, Møller AM, et al. Danish AnaesthesiaDatabasePoorprognosticvalueofthemodified Mal-lampatiscore:ameta-analysisinvolving177088patients.BrJ Anaesth.2011;107:659---67.
2.ShigaT,WajimaZ,InoueT, etal.Predictingdifficult intuba-tioninapparentlynormalpatients:ameta-analysisofbedside screeningtestperformance.Anesthesiology.2005;103:429---37.
3.FriedmanM,IbrahimH,JosephNJ.Stagingofobstructivesleep apnea/hypopneasyndrome:aguidetoappropriatetreatment. Laryngoscope.2004;114:454---9.
4.Friedman M, Ibrahim H, Bass L. Clinical staging for sleep-disordered breathing. Otolaryngol Head Neck Surg. 2002;127:13---21.
5.LiistroG, Rombaux P,Belge C, etal. High Mallampatiscore andnasalobstructionareassociatedriskfactorsforobstructive sleepapnoea.EurRespirJ.2003;21:248---52.
theFourthNationalAuditProjectoftheRoyalCollegeof Anaes-thetistsandtheDifficultAirwaySociety.Part1:anaesthesia.Br JAnaesth.2011;106:617---31.
7.RoseDK,CohenMM.Theairway:problemsandpredictionsin 18,500patients.CanJAnaesth.1994;41:372---83.
8.Mallampati SR, GattSP, GuginoLD, et al. A clinical signto predictdifficulttrachealintubation:aprospectivestudy.Can AnaesthSocJ.1985;32:429---34.
9.LeeA,FanLT,GinT,etal.Asystematicreview(meta-analysis) oftheaccuracyoftheMallampatiteststopredictthedifficult airway.AnesthAnalg.2006;102:1867---78.
10.PilkingtonS,CarliF,DakinMJ,et al.Increasein Mallampati scoreduringpregnancy.BrJAnaesth.1995;74:638---42.
11.WongSH,HungCT.Prevalenceandpredictionofdifficult intuba-tioninChinesewomen.AnaesthIntensiveCare.1999;27:49---52.
12.ButlerPJ, Dhara SS. Prediction ofdifficult laryngoscopy: an assessmentofthethyromentaldistanceand Mallampati pre-dictivetests.AnaesthIntensiveCare.1992;20:139---42.
13.Reed MJ,DunnMJ,McKeown DW.Cananairway assessment scorepredictdifficultyatintubationintheemergency depart-ment?EmergMedJ.2005;22:99---102.
14.Naguib M,Scamman FL, O’SullivanC, et al. Predictive per-formance of three multivariate difficult tracheal intubation models: adouble-blind, case-controlledstudy.AnesthAnalg. 2006;102:818---24.
15.WilsonME,SpiegelhalterD,RobertsonJA,etal.Predicting dif-ficultintubation.BrJAnaesth.1988;61:211---6.
16.ArnéJ,DescoinsP,FusciardiJ,etal.Preoperativeassessment for difficult intubation in general and ENT surgery: predic-tivevalueofaclinicalmultivariateriskindex.Br JAnaesth. 1998;80:140---6.