REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
PublicaçãoOficialdaSociedadeBrasileiradeAnestesiologiawww.sba.com.br
SCIENTIFIC
ARTICLE
YouTube
as
an
information
source
of
spinal
anesthesia,
epidural
anesthesia
and
combined
spinal
and
epidural
anesthesia
Serkan
Tulgar
∗,
Onur
Selvi,
Talat
Ercan
Serifsoy,
Ozgur
Senturk,
Zeliha
Ozer
MaltepeUniversityFacultyofMedicine,DepartmentofAnesthesiologyandReanimation,Istanbul,Turkey
Received4March2016;accepted16August2016 Availableonline15September2016
KEYWORDS Youtube; Anesthesia; Spinal; Epidural
Abstract
Introduction:SocialmediaasYouTubehavebecomeapartofdailylifeandmanystudies eval-uatedhealth-relatedYouTubevideos.OuraimwastoevaluatevideosavailableonYouTubefor theconformitytotextbookinformationandtheirsufficiencyasasourceforpatientinformation. Materialandmethod: A search of the YouTube website was performed using the keywords ‘‘spinal anesthesia,epidural anesthesia,combined spinal epiduralanesthesia’’. Firstly,180 videoswereevaluated andthecharacteristicsofthevideowere noted,andthefeaturesof thevideotoowerenotedifthevideowasregardingneuraxialanesthesia.Questionnaire1(Q1) evaluatingthevideoqualityrelatingtoneuraxialanesthesiawasdesignedusingatextbookas referenceandquestionnaire2(Q2)wasdesignedforevaluatingpatientinformation.
Results:Afterexclusions,40videoswereincludedinthestudy.TherewasnodifferenceinQ1 orQ2scoreswhenvideosweregroupedinto4quartersaccordingtotheirappearanceorder, timesinceuploadorviewstolengthrate(p>0.05).Therewasnostatisticaldifferencebetween Q1orQ2scoresforspinal,epiduralorcombinedvideos(p>0.05).Videospreparedbya health-careinstitutehaveahigherscoreinbothQuestionnaires1and2(10.87±4.28vs.5.84±2.90, p=0.044and3.89±5.43vs.1.19±3.35,p=0.01respectively).
Conclusion: Videospreparedby institutes,societies, etc.wereofhighereducationalvalue, butwerestillverylacking.Videosshouldbepreparedinadherencetoavailableandup-to-date guidelinestakingintoconsiderationappropriatestepbystepexplanationofeachprocedure, patientsafetyandfrequentlyaskedquestions.
©2016SociedadeBrasileiradeAnestesiologia.Publishedby ElsevierEditoraLtda.Thisisan openaccessarticleundertheCCBY-NC-NDlicense(
http://creativecommons.org/licenses/by-nc-nd/4.0/).
∗Correspondingauthor.
E-mail:[email protected](S.Tulgar).
http://dx.doi.org/10.1016/j.bjane.2016.08.005
PALAVRAS-CHAVE YouTube;
Anestesia; Raquidiana; Peridural
YouTubecomofontedeinformac¸ãoderaquianestesia,anestesiaperidurale
anestesiacombinadaraquiperidural
Resumo
Introduc¸ão:Asmídiassociaiscomo oYouTubetornaram-seumapartedocotidianoemuitos estudosavaliaramvídeosdoYouTuberelacionadosàsaúde.Nossoobjetivofoiavaliarosvídeos disponíveisnoYouTubeparaidentificaraexistênciadeconformidadecomasinformac¸õesem livrosdidáticosesuasuficiênciacomofontedeinformac¸ãoparaopaciente.
Materialemétodo:UmapesquisanositeYouTubefoirealizadausandoaspalavras-chavespinal anesthesia,epiduralanesthesia,combinedspinal-epiduralanesthesia(raquianestesia, aneste-siaperidural,anestesiacombinadaraquiperidural).Emprimeiro lugar,avaliamos180vídeos eobservandosuascaracterísticaseseeramreferentesàanestesianeuraxial.Oquestionário deavaliac¸ãodaqualidadedovídeo(Q1)relativaàanestesianeuraxialfoicriadousandoum livrodidáticocomoreferênciaeoquestionário2(Q2)foicriadoparaavaliarasinformac¸õesao paciente.
Resultados: Apósexclusões, 40 vídeosforam incluídos noestudo.Não houvediferenc¸a nos escoresdeQ1ouQ2quandoosvídeosforamagrupadosemquatrocategoriasdeacordocom aordemdeaparecimento,tempodeuploadoutaxadetempodevisualizac¸ão(p>0,05).Não houvediferenc¸aestatísticaentreosescoresdeQ1ouQ2paraosvídeosraquianestesia,peridural oucombinada(p>0,05).Osvídeospreparadosporuminstitutodesaúdeobtiveramescoresmais elevadosemambosQ1eQ2(10,87±4,28vs.5,84±2,90,p=0,044e3,89±5,43vs.1,19±3,35, p=0,01,respectivamente).
Conclusão:Osvídeoselaboradosporinstitutos,sociedadesetc.apresentaramumvalor educa-tivomaior, masaindamuito incompleto.Osvídeosdevemserpreparados em conformidade comas diretrizesatualizadas edisponíveis, comexplicac¸õesadequadas e detalhadassobre cadaprocedimento,seguranc¸adopacienteeperguntasmaisfrequentes.
©2016SociedadeBrasileiradeAnestesiologia.PublicadoporElsevierEditoraLtda.Este ´eum artigoOpen Accesssobumalicenc¸aCCBY-NC-ND(
http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Social media and video-sharing websites such asYouTube havebecomeapartofdailylifeandthenumberof health-related videos increases daily. YouTube is reported tobe the number one source of information on health-related topics,afterthepatient’sphysician.1---3Itisknownthat fol-lowingpatient-physicianmeetings,patientsseekadditional information.4
Socialmedia arefrequently usedby healthcare profes-sionalstofollowinnovationandadvancementintheirown field,seeotherpractices,evaluateandsendcommentsto videoownersandinteractwiththeirpeers.5---10Medical stu-dents are also turning to social media, especially video sharing websites such as YouTube, for medical education relatedmaterials.11---13
Unfortunately, many studies have demonstrated that the reliability, intelligibility and compliance to standards of many medical videos are not overseen or approved asappropriateor accurateby professionals in their field. Many studies have, therefore, investigated the reliabil-ity of internet sources health-related information14---19 as there is a significant risk that patients or their relatives mayfindmissing,falseorirrelevantinformationwhenthey researchahealth-relatedtopiconline.Convincingpersons exposed to this information pollution that their source is wrong information and thereafter providing accurate informationis more difficult than giving information toa
person whohas not been exposed to misinformation. On the other hand, small amount of inaccurate information acquired by healthcare professionals may lead to larger problems.
In patients who are due to undergo elective surgical procedures, it is verycommon for patients to seek infor-mation fromtheInternet or differentsources, evenafter theyhavebeen giveninformationby theirsurgeonand/or anesthesiologist.8,20 It is only natural that patients seek more and more informationona procedure theyare due toundergo.
Spinal anesthesia, epidural anesthesia and combined spinalepiduralanesthesiaarecommonlyusedmethodsfor regional anesthesia. Considering the popularity of video sharing websites such asYouTube, and the viewnumbers of related videos,there is a high likelihood that patients wouldseekaudiovisualinformationregardingthese proce-durestoo.Also,animportantstepofdevelopmentofskills in medicalstudents involvesobservation ofprocedureson manikinsorpatients,beforetheskillisperformedandafter it has been learnt from a textbook or via a professional healthcareinstructor.21,22
Table1 Selectionprocess(numberofvideos).
Searchkeyword Accepted Rejected
Spinalanesthesia(60) Spinal(23) Didnotmeetinclusioncriteria(12) Epidural(1) Notspinalbutrelatedanesthesia(6) Combined(2) Notrelatedanesthesia(6)
Duplication(10)
Epiduralanesthesia(60) Epidural(9) Didnotmeetinclusioncriteria(19) Combined(2) Duplication(16)
Notepiduralbutrelatedanesthesia(2) Notrelatedanesthesia(12)
Combined(60) Combined(3) Didnotmeetinclusioncriteria(9) Duplication(34)
Notneuraxialbutrelatedanesthesia(3) Notrelatedanesthesia(11)
totextbookinformationandtheirsufficiencyasasourcefor patientinformation.
Material
and
method
AsearchoftheYouTube(http://www.youtube.com)website wasperformed on 15.12.2015 usingthe keywords ‘‘spinal anesthesia, epidural anesthesia, combinedspinal epidural anesthesia’’. Alltimes, allcountriesand Englishlanguage waschosenastheYouTubefilterwithresultstoappearfrom mostrelevanttoleastrelevant.Thefirst60resultsforeach searchresultwerenoted.
The firstevaluatorevaluated180videos andnotedthe dateofupload,numberofviews,lengthofvideo,language, relevancetosearchterm,thecharacteristics ofthevideo and if the video was regarding neuraxial anesthesia, the featuresofthevideo.
Allauthors reachedconsensusfor thestudydesign and exclusioncriteriabeforecommencementofthisstudy. Fol-lowingfirstevaluation,videoslongerthan15min,videosnot related toneuraxial anesthesia, videos not in the English languageandrepeatvideoswereexcludedfromthestudy.
Afterinitialevaluationandexclusionswereperformed, five reviewers evaluated the video quality and adequacy asaninformationsourceforpatients.This evaluationwas performed using twoquestionnaires designed by authors. Reviewers werealsoaskedtoclassify eachvideo asbeing either;formedicaleducation,forhealthcareprofessionals, for patient information, product advertisement, institute promotion,confusing,other.Theaimofthevideowas deter-mined as the option at least three reviewers chose. If a classificationwasnotchosenbyatleastthreeofthe review-ers,thenre-classificationwasperformeduntilatleastthree reviewersagreedontheclassification.
Questionnaireevaluatingthevideo(Q1)qualityrelating toneuraxial anesthesia wasdesigned using a textbook as reference.23---25Afocusgroupmeetingwasperformedwhere allauthorsreachedconsensusonthequestionsforQ1.The second questionnaire (Q2) was designed, using the same method,basedonaquestionandanswerpageonthe Amer-icanSocietyofRegionalAnesthesia’swebsite,availableat:
https://www.asra.com/page/41/regional-anesthesia-for-surgery. The questionnaires contained10 and 5questions each,respectively.Everyevaluationcriterionwasscoredas none,averageandgoodonthebasisofcertainaspects.
Arubricwasavailableforallraters.ForQ1none,average andgoodreceived0,1or2pointsandforQ2theyreceived 0, 2 or 4 points, respectively. Some items contained two questions.Inthiscase,theraterswereinstructedtochoose none:ifbothquestionswerenotanswered,average:ifone wasfully and two were partially/inadequately answered, good:ifbothquestionswereadequatelyanswered. There-fore,eachvideoreceivedascorerangingfrom0---20points. Scoringwasperformedusingarubricthateachreviewerhad accesstoandwasdesigned byoneof theauthors.Videos wereacceptedasbeingverybad(0---4points),bad-average (5---8points),average(9---12points),good(13---16points)or verygood(17---20points).
Statisticalanalysis
InterRaterReliability(IRR) wascalculatedfor each video using Fleiss’ Kappa for rating score calculator avail-ableathttps://www.statstodo.com/CohenKappaPgm.php. Descriptive evaluation was performed for each video. Kappa<0--- noagreement,0.0---0.20 ---insignificant agree-ment, 0.21---0.40 --- moderate agreement, 0.41---0.60 ---mostpartagreement,0.61---0.80---significantlyagreement, 0.81---1.00---excellentagreement.
AllotherstatisticalevaluationwasperformedusingSPSS 16.0(SPSS,Chicago,IL,USA).Utestwasusedfor compar-isonofmediansbetweentwogroups.Morethanonegroup wascomparedusingANOVA.Normaldistributionwas eval-uatedwithShapiro---Wilktest.Thepost-hoc-Tukeytestwas usedforcomparisonofgroupswithnormaldistributionand Tamhanetestwasusedforcomparisonofgroupsthatwere notdistributednormally.
Results
12.5
10.0
Questionnaire 1 Questionnaire 2 7.5
5.0
2.5
0.0
Others Institute Uploader
Score of videos (mean)
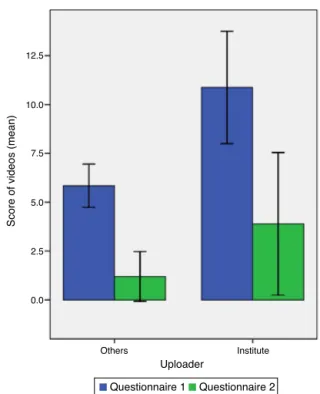
Figure1 Distributionofquestionnaire results accordingto videouploader.
showninTable1.Timesincevideouploadrangedfrom0---98 months with an average of 39.6±23.2m. Average video lengthwas280±180s(90---900s).
Videoswereclassifiedasaimedatmedicaleducationor healthprofessionalsin24,aimedforpatientinformationin 5, web site promotion in 2, institute promotion in 1 and confusingin5videos.
AveragescoreofvideosfromQuestionnaire1which mea-suredproceduralqualitywas7.14±3.88 (0.6---15.4).Eight videoswereclassifiedaccording toQuestionnaire1scores asbeingverybad,19videosasbad-average, sixvideosas average and7 videoswere classified asaverage-good.No videowasclassifiedasbeingverygood.Only2of13videos classifiedasaverageoraverage-goodwereuploadedbyan officialorganization,suchashospital,instituteorsociety.
Whenvideoswereevaluatedaccordingtopatient infor-mationwithQuestionnaire 2, average scorewas found to be1.93±4.13(0---15.9).Onevideo wasclassifiedasbeing verybad,3videosasaverageand2videosasaverage-good. Seventeen videos received no pointsfrom any reviewers. Allvideosclassifiedasbeingaverageoraverage-goodwere reportedasbeingpatientinformationvideosbythe review-ersandallhadbeenpreparedbyanacademicinstituteor hospital.Videosweregroupedasbeinguploadedbya health-careinstituteornotandQuestionnaire1andQuestionnaire 2resultswerecompared.Videospreparedbyahealthcare institutehaveahigherscoreinbothQuestionnaire1and2 (10.87±4.28vs.5.84±2.90,p=0.044and 3.89±5.43vs. 1.19±3.35,p=0.01respectively). Fig. 1 shows the ques-tionnaireresultsaccordingtouploadingsource.
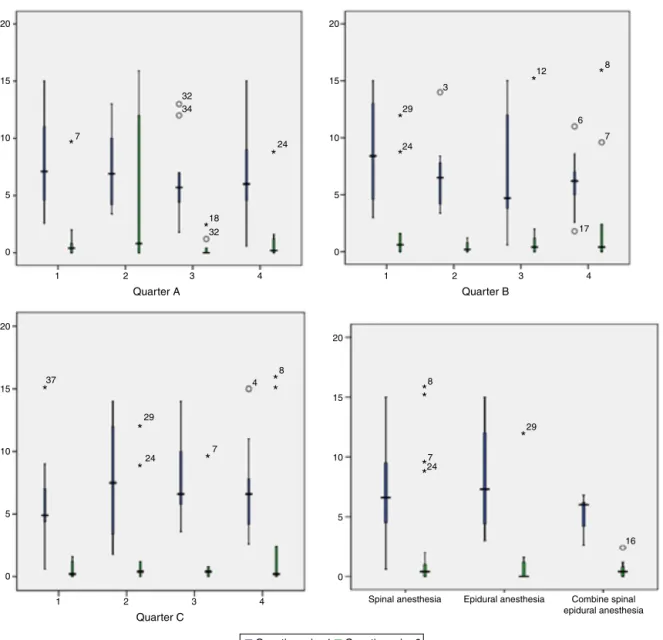
TherewasnodifferenceinQ1orQ2scoreswhenvideos weregroupedinto4quartersaccordingtotheirappearance order,timesinceuploadorviewstolengthrate(p>0.05).
TherewasnostatisticaldifferencebetweenQ1orQ2scores forspinal,epiduralorcombinedvideos(p>0.05)(Fig.2).
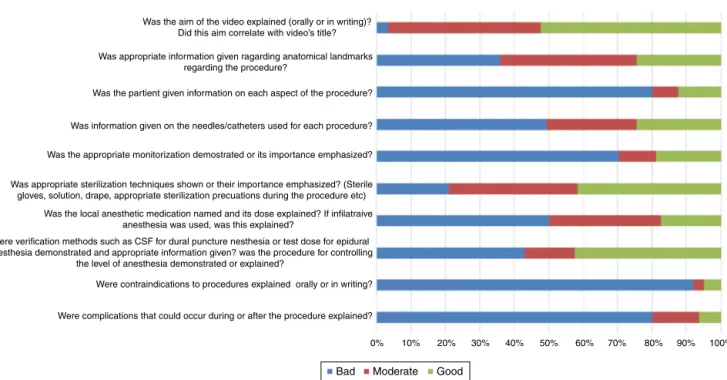
Results of evaluation of Q1 and Q2 are given in Figs. 3 and4. When Q1 wasevaluated, 80% ofvideos did notincludestep-by-stepinstructions,50%didnotintroduce materials (needle,catheter etc.)tobe used,70% didnot includepatientmonitorization,50%didnotgiveinformation onthedrugsusedordescribetheadministrationof infiltra-tiveanesthesia,over90%didnotmentioncontraindications and80%didnotmentioncomplications.Allvideosgenerally includedthevideo’saimandvideocontentandtitlewerein concordance.60%ofvideospartiallyorfullydescribedthe appropriateanatomicalstructuresandcloseto80%stressed theimportanceofsterilization.
WhenQ2wasanalyzed,over80%ofvideosdidnotanswer any of the questions. Only around 5% of videos could be classifiedasbeinggoodaccordingtoQ2.
When videos were evaluated according to sterilization techniques,13usedbetadine,1usedbetadineandisopropyl alcohol,1usedbetadineandspirit,6usedisopropylalcohol, and2 usedchlorhexidinefor procedure areasterilization. Seven-teen videos did not mention the agent used. Ster-iledrapewasusedin3ofisopropylalcohol,1ofbetadine and 1 or chlorhexidine videos. Videos usingchlorhexidine weredatedfrom2014---2015,videosusingisopropylalcohol fromafter 2012 andall videos usinga sterile drapewere fromafter2012.Videosusingbetadinewereobservedtobe newlyuploadedvideos.Neuraxialanesthesiawasperformed inthesittingpositionin26,sidepositionin10andwasnot mentionedin4videos.
When IRR was evaluated, kappa score was between 0.61---0.80in7videos(significantagreement),0.41---0.60in 31videos(mostpartagreement)and0.21---0.40in2 (moder-ateagreement)videos.ThehighestandlowestKappascore was0.69±0.07and0.37±0.09respectively.IRR was gen-erallyhighforallvideos.
Discussion
The results of our study have shown that while there is numerous videos on spinal, epidural and combines anes-thesia on video sharing website YouTube, more than half ofthesevideosarelowqualitywithrelation toprocedure technique, and nearly completely inadequate for patient informationpurposes.
20
15
10
5
0
1 7
18 32 32 34
24 24
29 3
12
6
7
17
8
7 7
4 8
29
24 37
*
*
* *
*
* *
* * *
*
* *
* *
*
* *24
29
16 8
2 3
Quarter A
4
20
15
10
5
0
1 2 3
Quarter B
4
20
15
10
5
0
1 2 3
Quarter C
4
20
15
10
5
0
Spinal anesthesia Epidural anesthesia Combine spinal epidural anesthesia
Questionnaire 1 Questionnaire 2
Figure2 Distributionofsearchresultsequence(QuarterA),loadingtime(QuarterB)andviews/videolength(QuarterC)according toneuraxialanesthesiatype.
uploaded videos were found to better adhere to asepsis techniques.
Therearemanyrecentlypublishedstudiescomparingthe useisopropylalcoholand/orchlorhexidinevs.betadinefor skin preparation.26---29 Thesestudies have alsoreportedan increaseintheuseofisopropylalcoholand/orchlorhexidine inrecentyears.
Severalstudieshaveactuallyfoundthatboththequality ofmedicalproceduresandtheireducationalvaluearelow invideosfoundonYouTube.1,3,8,30Somestudies,apartfrom notingthelowqualityofvideos,havealsostronglysuggested that some videos contain misinformation that could lead tonegativeoutcomes.31---34Severalreportshavestatedthat videosuploadedbyhealthprofessionalsor academic insti-tuteshavehigherqualitywhencomparedtothoseuploaded byindividuals,andthatthesevideoscouldbebeneficialfor theviewingofpatients.2,35,36Inourstudywefoundthe qual-ityofvideosgenerallylowandtheirusefulnessforpatient informationextremelyinsufficient.Manyvideoswerefound
tobeloaded multiple times. Videosprepared byregional anesthesiasocieties,academicinstitutesorhospitalswere foundtohavehighereducationalqualityandbettervaluefor patientinformationandthesevideosscoredhigherinboth questionnaires.However,wefoundnocorrelationbetween views/monthand thequalityofvideos.Some studiesthat evaluatedonlinevideosfortheirvalueindeveloping medi-cal skills also found that the quality of video correlated withtheaimofthevideoandwhetheritwasuploadedby aninstitution.Videosuploadedbyprofessionalinstitutions wereofhighereducationalqualitythanthoseuploadedby individuals.7,18,37,3860%ofvideosincludedinourstudywere evaluatedasbeingaimedat medicaleducationor health-careprofessionals.Consideringthatmanyvideosareinfact uploadedforeducationalpurposesandnotforpatient infor-mation,acloseadherencetoappropriateguidelineswillbe usefulforincreasingthequalityofthesevideos.
Was the aim of the video explained (orally or in writing)? Did this aim correlate with video’s title?
Was appropriate information given ragarding anatomical landmarks regarding the procedure?
Was the partient given information on each aspect of the procedure?
Was information given on the needles/catheters used for each procedure?
Was the appropriate monitorization demostrated or its importance emphasized?
Was appropriate sterilization techniques shown or their importance emphasized? (Sterile gloves, solution, drape, appropriate sterilization precuations during the procedure etc)
Was the local anesthetic medication named and its dose explained? If infilatraive anesthesia was used, was this explained?
Were verification methods such as CSF for dural puncture nesthesia or test dose for epidural anesthesia demonstrated and appropriate information given? was the procedure for controlling
the level of anesthesia demonstrated or explained?
Were contraindications to procedures explained orally or in writing?
Were complications that could occur during or after the procedure explained?
0%
Bad Moderate Good
10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
Figure3 Questionnaireforproceduralevaluatinganddistributionofanswers.
How is regional anesthesia different from general anesthesia?
If i choose regional anesthesia, does that mean i am awake during the surgery?
What are different types of blocks performed for regional anesthesia?
May i request what type of anesthesia i will receive?
What types of surgical procedures would be amenable for regional anesthesia?
75% 80% 85% 90% 95%
Bad Moderate Good
100%
Figure4 Questionnaireforpatientinformationand distribu-tionofanswers.
demonstrating anatomical points was high. However, no attention was shown to complications, contraindications, thedemonstrationof theimportanceof appropriate mon-itorizationandtheprovisionofstep-by-stepinformationto thepatient.Appropriatemonitorizationwasdemonstration invery few numberof videos.Some videosdemonstrated immediateadministrationof medicationafterentranceof spinalspace,beforeawaitingtheflowofcerebrospinalfluid. Inafewvideos,nocarewastakenforappropriate steriliza-tionprocedures.Webelievethatsuchvideosareharmfulif theyareusedforeducationalorskilldevelopmentpurposes. There were very few videos classified as very high qual-ity,furtherdemonstratingtheneedforstandardizationand higherqualityvideosespeciallyforeducationalpurposes.
Therewasnocorrelation between thequalityof video andupload time,views/video length ratioor thetype of neuraxial anesthesia in the video. Previous studies have evaluated correlation between the number of views and videoquality.2,13,17Wedidnotfinditlogicaltouseviewsas anindicatorofquality,astherewillbeadifferenceinviews
foroldervideosvs.newerones.Instead,wepreferredtouse views/months sinceupload asan indicator. Views/months sinceuploaddidnotcorrelatewithvideoquality.
Ourstudy has some limitations. We did notsearch for videosusingkeywords suchas‘‘spinalblock’’,‘‘neuraxial anesthesia’’, and ‘‘combined spinoepidural’’. These key-wordsmayhaverevealedfurthervideos.Weonlyincluded Englishlanguagevideosanddidnotincludevideosinother languages.Thisstudycouldhavebeendesignedsothatnon healthcare related individuals could evaluate each video accordingtoitspatientinformationqualityandmedical stu-dents for its educational value. All evaluators of Q1 and Q2 were healthcare professionals which may have led to a bias due to high expectations regarding video quality. Unfortunately thereareno previously validated question-nairesthatwecouldhaveusedforthisstudy.We,therefore, producedourownquestioner,whichwe hopecanbeused in future studies. Ourstudy evaluates the quality of pre-viously uploaded videos. Future uploads may change our findings.Also,we chosetoevaluatethefirst60videosfor oursearchterms.Thiswasadecisionbasedonlogical num-beraYouTubeuserwouldsearchfor,notonanystatistical calculation. Althoughthismaybeconsidered alimitation, thismethodhasbeenusedinsimilarstudiespreviously.1We wouldliketohaveincludedvideoanalyticssuchasaverage viewduration,traffic sourcesanddevicestoouranalysis. However,thisinformationisnotavailableviaYouTube’s web-site.
Conclusion
purposes.Videosshouldbepreparedinadherenceto avail-able and up-to-date guidelines taking into consideration appropriate step-by-step explanation of each procedure, patient safety and frequently asked questions. Although lacking in many aspects, we recommend that videos pro-duced by institutes should be viewed for educational or informationalpurposes,untilhigherqualityvideosare pro-duced.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.HoM,Stothers L,Lazare D,et al.Evaluation ofeducational contentofYouTubevideosrelatingtoneurogenicbladderand intermittentcatheterization.CanUrolAssocJ.2015;9:320---54.
2.Hassona Y, Taimeh D, Marahleh A, et al. YouTube as a sourceofinformationonmouth(oral)cancer.OralDis.2015,
http://dx.doi.org/10.1111/odi.12434.
3.Nason K, Donnelly A, Duncan HF. YouTube as a patient-informationsourceforrootcanaltreatment.IntEndodJ.2015,
http://dx.doi.org/10.1111/iej.12575.
4.GuptaHV, LeeRW,Raina SK,etal. AnalysisofYouTube asa sourceofinformationforperipheralneuropathy.MuscleNerve. 2016;53:27---31.
5.TaylorT.TF-6theuseofsocial mediainemergencymedical residenteducation.AnnEmergMed.2014;64:S146.
6.ArnbjörnssonE,EinarA.Theuseofsocialmediainmedical edu-cation:aliteraturereview.CreativeEduc.2014;05:2057---61.
7.RabeeR,NajimM,SherwaniY,etal.YouTubeinmedical educa-tion:astudent’sperspective.MedEducOnline.2015;20:29507.
8.FischerJ,GeurtsJ,ValderrabanoV,etal.Educationalquality ofYouTubevideosonkneearthrocentesis.JClinRheumatol. 2013;19:373---6.
9.SalemJ,BorgmannH,MurphyDG.Integratingsocialmediainto urologichealthcare:whatcanwelearnfromotherdisciplines? CurrUrolRep.2016;17:13.
10.Alotaibi NM, Badhiwala JH, Nassiri F, et al. The current useofsocial mediain neurosurgery.WorldNeurosurg. 2015,
http://dx.doi.org/10.1016/j.wneu.2015.11.011.
11.YıldırımB, BasaranO, AlatasOD,etal.Chesttube insertion techniques on YouTube:is social media a reliable source of learningmedicalskills?AmJEmergMed.2015;33:1709---10.
12.DuncanI,Yarwood-RossL,HaighC.YouTubeasasourceof clin-icalskillseducation.NurseEducToday.2013;33:1576---80.
13.MurugiahK,VallakatiA, RajputK,etal.YouTubeasasource ofinformationoncardiopulmonaryresuscitation.Resuscitation. 2011;82:332---4.
14.Sacchetti P, Zvara P, Plante MK. The internet and patient education---resourcesandtheirreliability:focusonaselect uro-logictopic.Urology.1999;53:1117---20.
15.HaymesAT.Thequalityofrhinoplastyhealthinformationonthe internet.AnnPlastSurg.2016;76:143---9.
16.LeeK,HotiK,HughesJD,etal.Consumeruseof‘‘DrGoogle’’: asurveyonhealthinformation-seekingbehaviorsand naviga-tionalneeds.JMedInternetRes.2015;17:e288.
17.RösslerB,LahnerD,SchebestaK,etal. Medicalinformation on theinternet: quality assessmentof lumbarpuncture and neuroaxialblocktechniquesonYouTube.ClinNeurolNeurosurg. 2012;114:655---8.
18.Camm CF, Sunderland N, Camm AJ. A quality assessment of cardiac auscultation material on YouTube. Clin Cardiol. 2013;36:77---81.
19.Gupta N, Sandhu G, Aggarwal A, et al. Quality assessment ofYouTube videosasasourceofinformationonColonoscopy. Abdomen.2015;2,http://dx.doi.org/10.14800/abdomen.953. 20.BrooksFM,LawrenceH,JonesA,etal.YouTubeTMasasource
ofpatientinformationforlumbardiscectomy.AnnRCollSurg Engl.2014;96:144---6.
21.VozenilekJ,HuffJS,ReznekM,etal.Seeone,doone,teach one:advancedtechnologyinmedicaleducation. AcadEmerg Med.2004;11:1149---54.
22.ZahiriHR,ParkAE,PughCM,etal.‘‘Seeone,doone,teach one’’:inadequacies ofcurrent methodsto trainsurgeons in herniarepair.SurgEndosc.2015;29:2867---72.
23.TurnbullJH,AleshiP.Spinalandepiduralanesthesia.Basic clin-icalanesthesia.NewYork:Springer;2015.p.211---31.
24.BrownDL.Spinal,epidural,andcaudalanesthesia.Miller’s anes-thesia.Elsevier;2010.p.1611---38.
25.DrasnerK,LarsonMD.Spinalandepiduralanesthesia.Basicsof anesthesia.Elsevier;2011.p.252---83.
26.Campbell JP, Plaat F,Checketts MR, et al.Safety guideline: skin antisepsis for central neuraxial blockade. Anaesthesia. 2014;69:1279---86.
27.CheckettsMR.Wash&go-butwithwhat?Skinantiseptic solu-tionsforcentralneuraxialblock.Anaesthesia.2012;67:819---22.
28.DarouicheRO,WallMJ,ItaniKMF,etal.Chlorhexidine---alcohol versus povidone---iodine for surgical-site antisepsis. N Engl J Med.2010;362:18---26.
29.Saha S. Antiseptic solutions for central neuraxial blockade: whichconcentrationofchlorhexidinetouse?Br JHospMed. 2014;75:298.
30.StauntonPF,BakerJF,GreenJ,etal.Onlinecurves:aquality analysisofscoliosisvideosonYouTube.Spine.2015;40:1857---61.
31.SorensenJA,PuszMD,BrietzkeSE.YouTubeasaninformation sourceforpediatricadenotonsillectomyandeartubesurgery. IntJPediatrOtorhinolaryngol.2014;78:65---70.
32.ButlerDP,PerryF,ShahZ,etal.Thequalityofvideoinformation onburnfirstaidavailableonYouTube.Burns.2013;39:856---9.
33.StellefsonM,ChaneyB,OchipaK,etal.YouTubeasasource ofchronicobstructivepulmonarydiseasepatienteducation:a socialmediacontentanalysis.ChronRespirDis.2014;11:61---71.
34.HansenC,InterranteJD,AilesEC,etal.AssessmentofYouTube videosasasourceofinformationonmedicationusein preg-nancy.PharmacoepidemiolDrugSaf.2016;25:35---44.
35.Günes¸ T, Serinken M, Alur ˙I, et al. YouTube as a source of information on varicose veins. Phlebology. 2015,
http://dx.doi.org/10.1177/0268355515596894.
36.Gonzalez-EstradaA,Cuervo-PardoL,GhoshB,etal.Popularon YouTube:acriticalappraisaloftheeducationalqualityof infor-mationregardingasthma.AllergyAsthmaProc.2015;36:121---6.
37.Lee JS, Seo HS, Hong TH. YouTube as a potential training methodforlaparoscopiccholecystectomy.AnnSurgTreatRes. 2015;89:92---7.