REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
PublicaçãoOficialdaSociedadeBrasileiradeAnestesiologiawww.sba.com.br
REVIEW
ARTICLE
Evaluation
and
perioperative
management
of
patients
with
diabetes
mellitus.
A
challenge
for
the
anesthesiologist
夽
João
Paulo
Jordão
Pontes
a,∗,
Florentino
Fernandes
Mendes
b,
Mateus
Meira
Vasconcelos
a,
Nubia
Rodrigues
Batista
aaHospitalSantaGenoveva,CentrodeEnsinoeTreinamento,Uberlândia,MG,Brazil
bUniversidadeFederaldeCiênciasdaSaúdedePortoAlegre(UFCSPA),PortoAlegre,RS,Brazil
Received6September2016;accepted12April2017
KEYWORDS
Diabetesmellitus; Anesthesia; Perioperativecare; Hypoglycemicagents; Insulin;
Glycosylated hemoglobin
Abstract Diabetesmellitus(DM)ischaracterizedbyalterationincarbohydratemetabolism,
leading to hyperglycemia and increased perioperative morbidity and mortality. It evolves withdiverseandprogressivephysiologicalchanges,andtheanestheticmanagementrequires attentionregardingthisdisease interferenceinmultipleorgansystemsandtheirrespective complications.Patient’shistory,physicalexamination,andcomplementaryexamsare impor-tantinthe preoperativemanagement, particularlyglycosylated hemoglobin(HbA1c),which hasastrongpredictivevalueforcomplicationsassociatedwithdiabetes.Thegoalofsurgical planningistoreducethefastingtimeandmaintainthepatient’sroutine.PatientswithType 1DMmustreceiveinsulin(evenduringthepreoperativefast)tomeet thebasal physiologi-caldemandsandavoidketoacidosis.WhereaspatientswithType2DMtreatedwithmultiple injectableand/ororaldrugs aresusceptibletodevelopahyperglycemichyperosmolarstate (HHS).Therefore, themanagementofhypoglycemic agentsanddifferenttypes ofinsulin is fundamental,aswellasdeterminingthesurgicalscheduleand,consequently,thenumberof lostmealsfordoseadjustmentanddrugsuspension.Currentevidencesuggeststhesafetarget tomaintainglycemiccontrolinsurgicalpatients,butdoesnotconcludewhetheritshouldbe obtainedwitheithermoderateorsevereglycemiccontrol.
©2017SociedadeBrasileiradeAnestesiologia.Publishedby ElsevierEditoraLtda.Thisisan openaccessarticleundertheCCBY-NC-NDlicense( http://creativecommons.org/licenses/by-nc-nd/4.0/).
夽 Center:ComplexoHospitalarSantaGenoveva,Uberlândia,MG,Brazil.
∗Correspondingauthor.
E-mail:[email protected](J.P.Pontes).
https://doi.org/10.1016/j.bjane.2017.06.002
PALAVRAS-CHAVE
Diabetesmelito; Anestesia; Cuidados perioperatórios; Hipoglicemiantes; Insulina;
Hemoglobina glicosilada
Avaliac¸ãoemanejoperioperatóriodepacientescomdiabetesmelito.Umdesafio
paraoanestesiologista
Resumo O diabetes melito (DM) é caracterizado por alterac¸ão no metabolismo de
car-boidratosquelevaàhiperglicemiaeaoaumentodamorbimortalidadeperioperatória.Cursa comalterac¸õesfisiológicasdiversaseprogressivase,paraomanejoanestésico,deve-se aten-tar para a interferência dessa doenc¸a nos múltiplos sistemas orgânicos e suas respectivas complicac¸ões.Anamnese,examefísicoeexamescomplementaressãoimportantesnomanejo pré-operatório,com destaquepara ahemoglobina glicosilada(HbA1c),que tem forte valor preditivoparacomplicac¸õesassociadasaodiabetes.Oplanejamentocirúrgicotemcomo obje-tivosareduc¸ãodotempodejejumeamanutenc¸ãodarotinadopaciente.Pacientesportadores deDMTipo1precisamreceber,mesmoemjejumperioperatório,insulinaparasupriras deman-dasfisiológicasbasaiseevitarcetoacidose.JáospacientesportadoresdeDMTipo2,tratados commúltiplosfármacosinjetáveise/ouorais,sãosuscetíveisaodesenvolvimentodeumestado hiperosmolarhiperglicêmico(EHH).Assim,omanejodoshipoglicemiantesedosdiferentestipos deinsulinaéfundamental,alémdadeterminac¸ãodohoráriocirúrgicoe,consequentemente, donúmeroderefeic¸õesperdidasparaadequac¸ãodedosesoususpensãodosmedicamentos.As evidênciasatuaissugeremoalvodemanutenc¸ãodaglicemiaseguroparaospacientescirúrgicos, semconcluirsedeveserobtidocomcontroleglicêmicointensivooumoderado.
©2017SociedadeBrasileiradeAnestesiologia.PublicadoporElsevierEditoraLtda.Este ´eum artigoOpen Accesssobumalicenc¸aCCBY-NC-ND( http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Insurgicalpatients,thepresenceofdiabetesmellitus(DM)
orhyperglycemiaisassociatedwithincreasedmorbidityand
mortality, with a perioperative mortality rate up to 50%
higherthaninthenon-diabeticpopulation.1Thereare
mul-tiplereasonsfortheseadverseoutcomes,suchasfailureto
identifydiabeticorhyperglycemicpatients;multiple
comor-biditiesincludingmicro and macrovascularcomplications;
complex polypharmacy and insulin prescription errors;
increasedperioperativeandpostoperativeinfections;
asso-ciatedepisodesofhypoglycemiaandhyperglycemia1;alack
of(or inadequate)institutionalprotocols formanagement
of diabetic or hyperglycemic inpatients; and inadequate
knowledge of diabetes and hyperglycemia management
amongststaffprovidingcare.2
Material
and
methods
We searched multiple databases, including Medline via
PubMed (January 1966 to August 2016), The Cochrane
Library and Lilacs (from 1982 to August 2016). After a
bibliographicalsurvey,thearticleswithbetter
methodologi-caldesign wereselected.Wealsousethe evidence-based
updatesfromtheUpToDateandMedscape domains.There
wasnolanguagerestriction.
SearcheswereperformedbetweenMayandAugust2016.
ThefollowingstrategieswereusedforsearchesinPubMed:
1. ‘‘Diabetes Mellitus’’ [All Fields] AND ‘‘Anesthesia’’
[All Fields], ‘‘Diabetes Mellitus’’ [All Fields] AND
‘‘Perioperative Period’’ [All Fields], ‘‘Glycemic
Con-trol’’[AllFields]AND‘‘PerioperativeCare’’[AllFields],
‘‘Glycemic Control’’ [All Fields] AND ‘‘Anesthesia’’
[All Fields], ‘‘Diabetes Mellitus’’ [All Fields] AND
‘‘Anesthesia’’ [All Fields] AND ‘‘Perioperative’’ [All
Fields];
2. ‘‘Diabetes Mellitus’’ [MeSH Terms] AND ‘‘Anesthesia’’
[MeSH Terms], ‘‘Diabetes Mellitus’’ [MeSH Terms] AND
‘‘Perioperative Period’’ [MeSH Terms], ‘‘Anesthesia’’
[MeSH Terms] AND ‘‘Diabetes Mellitus’’ [MeSH Terms]
AND ‘‘Perioperative Period’’ [MeSH Terms], ‘‘Diabetes
Mellitus’’ [MeSH Terms] AND ‘‘Perioperative Care’’
[MeSHTerms];
3. ‘‘Diabetes Mellitus’’ [MeSH Terms] OR (‘‘diabetes’’
[All Fields] AND‘‘mellitus’’ [All Fields]) OR ‘‘diabetes
mellitus’’ [All Fields] AND (‘‘anaesthesia’’ [All Fields]
OR ‘‘anesthesia’’ [MeSH Terms] OR ‘‘anesthesia’’ [All
Fields])ANDPerioperative[AllFields].
Physiologicalchangesandanestheticimplications
Diabetesmellitusisadiseasecharacterizedbyabnormality
in carbohydrate metabolism, which evolves with
hyper-glycemia. If left untreated, it is a debilitating disease,
leadingtochronicorganfailureanddysfunction.Type1
dia-betes(DM1)resultsfromthedestructionofinsulin-producing
pancreatic -cells by an autoimmunemechanism, causing
complete deficiency in insulin secretion. Type 2 diabetes
(DM2),themostcommonformofdiabetes,isaconsequence
ofperipheral resistancetoinsulinaction andisfrequently
associatedwithprogressivefailureininsulinsecretionover
theyears,resultingfromdysfunctioninpancreatic-cells
duetoglycotoxicity,lipotoxicity,andamyloidformation.3
Thediagnosticcriteriafordiabetesmellitusarelistedin
Table1 Diagnosticcriteriafordiabetesmellitusaccording totheAmericanDiabetesAssociation---2015.4
1.Glycosylatedhemoglobin(HbA1c)≥6.5%aOR
2.Fastingglucose≥126mg.dL−1a(nocaloricintakeforat
least8h)OR
3.Glycemiaafter2h---oralGTT≥200mg.dL−1aOR
4.Patientswithclassicsymptomsofhyperglycemiaor hyperglycemiccrisis,withrandomglycemia≥200mg.dL−1
GTT,glucosetolerancetest.
a Intheabsenceofunambiguoushyperglycemia,theresults
shouldbeconfirmedbytestrepetition.
With the broader screening of blood glucose, another
groupofpatientsknownaspre-diabeticshasalsobeen
iden-tified.Theycanbeclassifiedintotwomainclasses:impaired
fastingglucoseandglucoseintolerance.Positivescreening
of thesepatients includes: fastingblood glucosebetween
100 and 125mg.dL−1; glycemia 2h after oral glucose
tol-erancetest(GTT)between140and199mg.dL−1;orHbA1c
between5.7and6.4%.5
The physiological changesindiabeticpatientsare
mul-tipleandprogressiveand,foranestheticmanagement,the
followingorgansandsystemsmustbeemphasized:
muscu-loskeletal,kidney,neurological,andcardiovascular.
Musculoskeletalsystem
Chronic hyperglycemia leads to non-enzymatic
glycosyla-tionofproteinsandabnormalcollagencross-linksinjoints,
limiting mobility and leading to the so-called stiff joint
syndrome(SJS).Temporomandibular,atlanto-occipital,and
cervical spine joints may be affected.6 Diabetes
sclere-demaischaracterizedbyfirm,wood-like,non-compressible
nuchal edema and upper dorsum regions and, associated
with reduced jointmobility, may limit the neck rangeof
motionandhinderorotrachealintubation.7
Kidney
A relevant proportion of patients with DM have diabetic
nephropathy.Thischroniccomplicationischaracterizedby
thedevelopmentofalbuminuriaandprogressivereduction
of renal function in patients without adequate glycemic
control. In general, patients with this complication are
at greater risk of perioperative morbidity and mortality.
Therefore, albuminuriascreening in thesepatients would
contributetofurtherassessmentoftheriskofacuterenal
failure(ARF).8
In the presence of hypovolemia, intraoperative use of
non-steroidalanti-inflammatorydrugs(NSAIDs)mayimpair
redistribution of renal blood flow and worsenrenal
func-tion.Thisisespeciallyimportantwhenconcomitantlyusing
drugsthatmodulatetherenin-angiotensin-aldosterone
sys-tem(RAAS).8Therefore,cautionshouldbeexercisedinthe
useof NSAIDs inpatients withDM,whomayalreadyhave
somedegreeofkidneyfailure.Moreover,theuseofNSAIDs
alsoincreasestheriskofedema,whichmaybeaggravated
whengivenconcomitantlywiththeclassoforalantidiabetic
drugsknownasglitazones.2
Likewise,cyclooxygenasetype2(COX-2)inhibitorsmay
affect kidney function in at-riskpatients, including those
with diabetic nephropathy. In a review of the literature,
ARFand/orsevereelectrolytechanges(particularly
hyper-kalemiaandmetabolic acidosis)wereclearlytriggered by
celecoxiborrofecoxib.9InBrazil,thereisalackofstudies
onthesafetyofparecoxibforperioperativevenoususeand
itsimpactonthekidneyfunctionofthispopulation.
Neurologicalsystem
Neurological effects of diabetes increase the risk of
cerebrovascularaccident(CVA)andthepresenceof
hyper-glycemiaisastrongpredictorofworseoutcomesinvarious
forms of acute brain injury.10 A prospective study found
association between HbA1c levels and risk of CVA in
dia-beticandnon-diabetic patients.11 Infact, the vasodilator
responsetohypercapnia,measuredbytranscranialDoppler,
wasreducedindiabeticpatientscomparedtonon-diabetics
patients.The degreeofreductionwascorrelatedwiththe
HbA1c levels of patients.12 This finding raises interesting
questionsabout the roleof long-term glycemiccontrol in
the regulation of cerebral vascular reactivity in diabetic
patients.
Nerve fibers in diabetic patients may be more
suscep-tible toischemic injury,as they arealready under stress
fromchronic ischemic hypoxia. Local anesthetics may be
neurotoxic.Toavoidnervedamageinthesepatientscaution
shouldbeexercisedregardingtotaldoseandconcentration
oflocalanestheticsusedinregionalanesthesia.8
Autonomicneuropathy
DiabeticautonomicneuropathyisacommonDM
complica-tionoften undiagnosed.This complication mayaffect the
gastrointestinal,genitourinary,andcardiovascularsystems.
The main clinical manifestations of diabetic autonomic
neuropathy include resting tachycardia, exercise
intol-erance, orthostatic hypotension, intestinal constipation,
gastroparesis,bladderdysfunction,impairedneurovascular
function,andlossofautonomicresponsetohypoglycemia.
Foranestheticmanagement,in additiontocardiovascular
autonomic alterations, it is important to remember that
reducedesophagealmotilityandgastroparesismayleadto
vomitingandaspirationofgastriccontent.8Acuteorchronic
hyperglycemiaincreasesthegastricemptyingtimeandmay
increasethevolumeofgastriccontents.10
Cardiovascularsystem
Diabetic patients are at increased risk of
hyperten-sion, coronary artery disease (CAD), silent myocardial
ischemia,systolicanddiastolicheartfailure,andcongestive
heartfailure.8Throughseveralmechanisms,hyperglycemia
impairs vasodilation and induces a proinflammatory,
pro-thrombotic,andproatherogenicstate,which arethebasis
for vascular complications commonly found in diabetic
patients.13Patientswithdiabetesbutnoprioracute
myocar-dialinfarction(AMI)havethesameriskofcoronaryevents
as a non-diabetic patient with previous AMI.14 In fact,
diabetic patients are considered to be at increased risk
for CAD----intensive use of antiatherosclerotic therapy is
mandatory.15 TheAmericanHeartAssociation(AHA)
guide-linesonperioperativecardiovascularevaluationofpatients
undergoingnon-cardiacsurgeryreportdiabetes,especially
inpatientsreceivinginsulintherapy,asanindependentrisk
PreoperativeassessmentandimportanceofHbA1c
In DM patients, clinical history should clarify the type
of diabetes (DM1, DM2, gestational DM or other types),
glycemic control, diagnostic time (predictor of chronic
complications), drug therapy (oral, noninsulin injectable
antidiabetic drugs or insulin), dose and dosing time of
medications.17
The occurrence and frequency of hypoglycemia should
be questioned, as they interfere with preoperative
man-agement of medications, in addition to the frequency of
hospitalizationrelatedto glycemiccontrol (acute
decom-pensation).Patient’sabilitytomeasurehisbloodsugarand
understand the principles of diabetes therapy should be
evaluated,asit influencesthe perioperativemanagement
ofthesepatients.17
Other riskfactorsfor atherosclerosisshould be
investi-gated(smoking,hypertension,dyslipidemia,familyhistory,
sedentary lifestyle), presence of recent infections that
mayalterperioperative glycemiccontrol (skin, feet,
gen-itourinary tract, dental), and use of drugs for other
comorbidities.18
Animportant concernindiabeticpatientsis the
signif-icant number of patients with DM2 who are unaware of
thediagnosis andonly becomeaware ofit at thetimeof
surgery.Astudywithpatientsundergoingnon-cardiac
sur-geriesfoundan undiagnosedDMrateof10% andimpaired
fastingglycemiaof11%.19Anotherstudyshowedthat24%of
patientsreferredfromprimarycaretoelectivesurgeryhad
aDMdiagnosis orimpaired fastingglycemiadiscoveredon
thedayofsurgery.20Interestingly,patientswithundiagnosed
DMweremorelikelytorequireresuscitation, reintubation
andlongerpostoperativemechanicalventilation,andhigher
perioperative mortality comparedto patients without DM
andpatientswithpreviouslydiagnosedDM.21Thesefindings,
togetherwiththoseofotherinvestigators,suggestthat
undi-agnosedDMisanevengreaterriskfactorforperioperative
morbidityandmortalitythanpreviouslydiagnosedDM.The
increasedriskmayberelatedtoseveralfactors,including
inadequatepreventivecareandlessaggressivetherapyby
thecareteam.5
Physicalexaminationincludesbloodpressureassessment
withemphasis on the search for orthostatic hypotension,
a potential sign of autonomic neuropathy. Dilated fundus
examination mayprovide an idea of the risk of a patient
developing postoperativevisual loss, especially after
pro-longedprostheticcolumnsurgeryandaftercardiacsurgery
withcardiopulmonarybypass.Duetothehomologybetween
cerebral and retinal microcirculations, changes in retinal
vasculaturemayreflectsimilarchangesincerebral
vascul-ature.Thepresenceofdiabeticretinopathymaytherefore
alsoindicateimpairmentofcerebralmicrocirculation.Some
studieshaveshownthatdiabeticretinopathywasapredictor
ofpostoperativecognitivedysfunctionduetoimpairmentof
coexistingcerebralcirculation.22
Stiffjoint syndromeadds significant risk duringairway
management.Onphysicalexamination,thepatientpresents
withan inability to move close the palm surfaces of the
interphalangealjointswhile pressingonehandagainstthe
other----positive‘‘prayersignal’’. Airwayevaluationshould
includethesizeofthethyroidgland,aspatientswithDM1
have an association of about 15% withother autoimmune
Table 2 Mean glycemia assessment for specific HbA1c
values.
HbA1c(%) Plasmameanglycemia
mg.dL−1 mmol.L−1
6 126 7.0
7 154 8.6
8 186 10.2
8.5 200 11.0
9 212 11.8
10 240 13.4
11 269 14.9
12 298 16.5
AdaptedfromRefs.25,26.
diseases, such as Hashimoto’s thyroiditis and Graves’
disease.18
Toassess thedegree of subsequentnerve damage,the
degree of preoperative neurological dysfunction should
alwaysbedocumented,particularlypriortoregional
anes-thesia. In search of signs of skin lesion or infection,
examining theskin (insulin injectionsite)and feetshould
bepartoftheevaluationroutine.
Basiccomplementaryinvestigation shouldinclude:
res-tingelectrocardiogram(ECG),assessmentofkidneyfunction
(serumcreatinine),electrolytes,fastingbloodglucoseand
HbA1c (ifnotmeasured inthe lasttwotothreemonths).
In individualized cases,additional investigationsincluding
non-invasivecardiactestsshouldbeconsidered.23
HbA1cprovidesaviewofglycemiccontroloverthelast
twotothreemonthsandhasastrongpredictivevaluefor
complications of diabetes.24 High preoperative levels are
associatedwithincreasedperioperativeriskandconstitutea
goodpreoperativescreeningtest.2,5,8Table2showsthe
cor-relation between HbA1cand average blood glucoselevels
basedontwolargestudies.25,26
Studieshaveshownthatpoorglycemiccontrolreflected
through perioperative high levels of blood glucose and
HbA1careassociatedwithworsesurgicaloutcomes.These
resultswerefound inbothelective andemergency
surger-iesincludingspinal,27 vascular,28 colorectal,29 cardiac,30,31
trauma,32 thoracic,33 orthopedic,34 neurologicaland
hepa-tobiliarysurgeries.35,36Astudyhasshownthatan increase
in mortality greater than 50%, a 2.4-fold increase in the
incidenceofpostoperativerespiratoryinfections,incidence
of duplicateAMI,1,2 anda nearlytwo-fold increase in the
incidenceofARIareamongtheworstoutcomes.37
Due to the new evidence linking high levelsof HbA1c
as a marker of poor glycemic control and perioperative
complications,arecentBritishguidelinerecommendsthat
patients withDM referred fromprimary care for surgical
evaluation should have their most recent HbA1c results
includedintheirreferralandthattheHbA1cdosageshould
berequestedfromdiabeticpatientswithscheduledsurgery
if theyhave not hada measurement recordedin the last
threemonths.38Inadditiontotheroutineevaluationin
dia-beticpatientswithoutHbA1cmeasurementinthelastthree
months, during preoperative evaluation of non-diabetic
patientswithDMriskfactors(age>45years,hypertension,
polycysticovary,amongothers),someauthorsrecommend
routinemeasurementsofHbA1c.4,8
Infact,HbA1cmeasurementisthepreoperativetest
indi-catedforpatientsdiagnosedwithDMorriskfactors.Onthe
otherhand,inordertobetterevaluateglycemiccontroland
diagnosesdiabetesinthosewithunknownDM,someauthors
suggestthedeterminationofHbA1clevelsinthe
preoper-ative period of all patients undergoing major surgeries.39
This approach is justified considering that hyperglycemic
patientsand/orpatientswithuntreatedDMinthe
preopera-tiveperiodpresentedworseoutcomescomparedtopatients
withtreateddiabetesevenwithsimilarpreoperativeblood
glucosevalues.1,21,40SuchapproachmaynotonlyidentifyDM
intheseundiagnosedpatients,buthelpinchoosingthebest
time for elective surgery, considering that postponement
couldimproveglycemiccontrolandreducecomplications.39
On theotherhand,asystematicreviewconcludedthat
thepreoperativebloodglucoseandHbA1cmeasurementin
patientsundergoingelectivenon-cardiacsurgeryisnot
nec-essary in asymptomatic and non-diabetic patients. In this
groupofpatients,theHbA1candbloodglucosevalueswould
only be justified in those undergoing major vascular and
orthopedicsurgerybecausetheyareathigherrisk.41
Impactofsurgicalstressandanesthesiaon metaboliccontrol
Severalconditionsindiabeticpatientsmayresultin
wors-eningofhyperglycemiaduringtheperioperativeperiod.42,43
Surgicalstressinducesneuroendocrineresponse;glucagon,
epinephrine,andcortisol(counterregulatoryhormones)are
the first secreted hormones. These hormones lead to a
catabolicstate, which contributestoperioperative
hyper-glycemia.Inextremecases,theincreasedcounterregulatory
hormones and consequent hyperglycemia may lead to a
metabolicdecompensationandresultindiabetic
ketoacido-sisinpatientswithDM1orinahyperosmolarhyperglycemic
nonketoticstate(DM2).44
Drugs used during surgery may also interfere with the
degree of hyperglycemia in diabetic patients. Anesthetic
agents and sedatives may affect glucose homeostasis via
modulation of sympathetic tone.42 In fact, some
anes-thetic agents mayreduce catabolic hormone secretionor
changeinsulinsecretioninDM2patientswithresidualinsulin
secretion.8
General anesthesia may mask the common signs and
symptoms of hypoglycemia, one of the main concerns of
anesthesiologistsintheperioperativeperiod.8Thechoiceof
anestheticagentmayaffectglucosehomeostasis.Highdoses
ofbenzodiazepinesandgamma-aminobutyricacidagonists
(GABA) reduce thesecretion of adrenocorticotrophic
hor-mone(ACTH)andcortisolandmayreducethehyperglycemic
response tosurgery.8 Etomidate inhibits adrenal synthesis
of steroids by blocking the 11-hydroxylase activity and
triggersareductioninhyperglycemicresponsetosurgery.45
Clonidine reduces sympathetic tone and norepinephrine
releaseatnerveterminals.Highdoseofopioidsappearto
decreasethehyperglycemicresponsetosurgeryby
reduc-ingcatabolichormones.46 In vitrostudieshaveshown that
inhalationalanesthetics,suchashalothaneandisoflurane,
inhibit the normal production of glucose-triggered insulin
in a dose-dependent manner and result in hyperglycemic
response.47
Regional anesthesia, including subarachnoid, epidural
andother regionalblockades,can modulatethesecretion
ofcatabolic hormones andinsulin. The activationof
sym-pathetic nervous system and hypothalamic-pituitary axis
induced by surgical stress may be avoided by this type
of anesthesia.48 In patients with insulin resistance some
authorshave shown that regionalanesthesiaandepidural
analgesia,comparedtogeneralanesthesia,mayreducethe
degreeofinsulinresistanceinearlypostoperativeperiod.49
However,therearereservationsandconcernsregardingthe
useofregionalanesthesiainDMpatients,bothforperipheral
blocks and neuraxial approach techniques. DM is
associ-atedwithseveraltypesofneuropathies;symmetricaldistal
polyneuropathy(diabeticpolyneuropathy---DPN)and
auto-nomicneuropathyarepresentinupto50%oflong-standing
diabeticpatients.7,22 DPN patients maybe more
suscepti-bletodouble-crushinjury(increasedsusceptibilitytonerve
damage following low-grade secondary aggression, if we
assumethatdiabeticfiberalreadyhassomedegreeofinjury
fromchronichypoxemia),50butthecurrentclinicalevidence
isinconclusive.Animalstudieshaveshownthatnervefibers
ofdiabeticanimalsaremoresensitivetotheeffectsoflocal
anestheticsandmaybemoresusceptibletothe
neurotox-icitytriggered by thesedrugs.51,52 Clinicalstudies suggest
increasedsensitivitytolocalanestheticsindiabeticpatients
undergoing peripheral nerve blocks.53 Moreover, diabetic
nerves are less sensitive to electrical stimulation, which
theoreticallywouldincreasetheriskofnerveinjurybythe
needlewhentrying tolocatethenerveswithaperipheral
nervestimulator.54 For these reasons, the American
Soci-ety of Regional Anesthesia (ASRA)55 recommendations for
peripheralnerveblocksinverysymptomaticpatientsareto
limittheconcentrationand/ordoseofthelocalanesthetic,
avoidtheuseofepinephrineasanadjuvant,anduse
ultra-soundasaguidetokeeptheneedletipawayfromthenerve.
Inaddition,evidencehasshown thatdiabeticpatientsare
morelikelytodevelopepiduralabscessesandhemodynamic
instability following neuraxial blocks (patients with
auto-nomicneuropathy).2
Surgicalplanning
The main goals areto reduce fasting period,ensure
nor-moglycemia (capillary blood glucose between 108 and
180mg.dL−1), and reduce patientdisruption tothe
maxi-mum.Ideally,thepatientshouldbescheduledforthefirst
hoursofsurgicalmap.Ifthepatient’sfastingtimeislimited
toone missedmeal, the option is to change his/her
nor-mal medication for diabetes. If longer periods of fasting
arepredicted,a variablerate intravenousinsulin infusion
(VRIII)shouldbeusedandaspecialistassessmentrequested.
On theday of surgery, thepatientshould receive written
instructions on medication management, control of
peri-operativehypo-orhyperglycemia,andprobableeffectsof
surgeryondiabetescontrol.2
Capillaryglycemiashouldbecheckedonadmission,prior
toinductionofanesthesia,andmonitoredregularlyduring
the procedure (at least every hour, or more often if the
Managementoforalandinjectablenon-insulin antidiabeticdrugs
Theglycemiccontrolindiabeticpatientsconsistsofthe
bal-ancebetweencarbohydrateintakeanditsexpenditure(for
example,exercise).Italsodependsonwhichdrugis used
and how these drugs work. During fasting periods, some
agents(sulfonylureasandglinides)reduceglucose
concen-tration, which require dose modification and/or agent
suspension.Other agentspreventincreased glucoselevels
(metformin, glucagon-like peptide-1 [GLP-1] analogs,and
dipeptidylpeptidase-4[DPP-4]inhibitors)andmaybe
con-tinuedwithoutriskofhypoglycaemia.2
Metforminactsasaninsulinsensitizerandinhibits
gluco-neogenesis.Someguidelinesrecommenddiscontinuingthe
useofmetformin24---48hpriortosurgerybecauseoftherisk
ofdevelopinglacticacidosisandperioperativerenalfailure
duetometforminaccumulation.56 Astheevidenceforthis
approachisweakandthereisevidencethatperioperative
continuationofmetforminissafe,arationalapproachisto
continuetheperioperativeuseofmetformininallpatients
with a short fasting period, normal kidney function, and
whencontrastisnotused.2,39Ontheotherhand,metformin
should be discontinued when there is preexisting renal
damage(glomerular filtration rate--- GFR<60mL.min−1 or
increasedcreatinine),2,57 use ofcontrastor significantrisk
ofARFdevelopment.Insuchcases,discontinuationshould
occuronthedayofsurgeryandforthenext48h.2
During fasting, sulfonylureas stimulate insulin
secre-tionand maylead tohypoglycemia. Because theyhave a
longerhalf-life (2---10h),58 it is recommendedtoomitthe
dose on the day of surgery regardless of the procedure
time.2 Glinides’ mechanism of action is similartothat of
sulphonylureas and, for having a short half-life (1h) and
early action peak, they are used to control postprandial
bloodglucose----hypoglycemia withthistypeof drugisless
common.17Doseomissiononthedayofsurgeryshouldoccur
inthe morningprocedures. Ifsurgery isperformed in the
afternoonandthepatienthasa mealin themorning,the
pre-mealdosemaybeused.2
Similar to metformin, glitazones (or thiazolinediones)
act through peripheral sensitization to insulin. They are
notassociated withlacticacidosis, although theymaybe
associatedwithwaterretentionandpossible worseningof
postoperative edema and heart failure.59 Consensus does
notsuggest thisdrug discontinuationduring the
perioper-ativeperiod2,17,60,61;itshouldbeusedonthedayofsurgery
andattention shouldbegiven tothepossibilityof edema
worseningandcardiacdecompensationinpatientsatrisk.2
Alpha-glycosidaseinhibitorsinhibitoligosaccharidaseand
disaccharidaseenzymesandreduceglucoseabsorptionafter
meals.Onthedayofsurgery,thedoseshouldbeomittedin
morningprocedures.However,ifthesurgeryisinthe
after-noonand thepatienthas hada mealinthe morning,the
pre-mealdosemaybeused,2ifweconsiderthatthesedrugs
arenothypoglycemicandhaveashorthalf-life.17
Thenewincretinicdrugs,representedbyGLP-1analogs
andDPP-4 inhibitors,increase insulin secretionafter
glu-cose ingestion and reduce glucagon secretion.58 It does
notcause hypoglycemia, but may leadto delayed gastric
emptying by increasing GLP-1.60 Therefore, some authors
suggestthatitbediscontinuedonthedayofprocedure.8,60
Notwithstanding,the mostrecentBritishguideline
recom-mends its use until the day of surgery regardless of the
proceduretime.2
Thesodiumglucoseco-transportertype2(SGLT2)protein
inhibitors,presentintheproximalconvolutedtubuleofthe
nephron,haverecentlybeenintroducedforDMtreatment.
BecauseSGLT2leadtoglycosuria,itcangenerateosmotic
diuresiswithdehydrationandhypotension;theseeffectsare
morecommonwiththeconcomitantuseofdiuretics.62Due
tolack ofexperiencewiththesedrugs,itisrecommended
toomit thedose on theday of surgery, regardless of the
proceduretime.2
The managementof oral antidiabeticdrugs in patients
whowillundergoashortfastingperiod;thatis,limitedtoa
lostmeal,issummarizedinTable3.Allsuchdrugsmustbe
discontinueduntiltheoralintakeisreestablished.2,8
Insulinmanagement
Patientswith DM1are oftentreated with multiple insulin
injection.Thepreferredregimenofphysiologicinsulin
dos-ing (also called basal bolus) mimics endogenous insulin
production by providing basal, prandial, and correction
doses. Basal dose may be offered by a continuous
sub-cutaneous insulininfusion throughan insulinpump (based
on a rate of rapid-acting insulin analogs) or through
long-actingandnon-peakinsulinanalogs.Basalinsulin
com-prisesapproximately 50%of the patient’stotal dailydose
of insulin, meeting the metabolic needs without causing
hypoglycemia. Patients inject variable boluses of
fast-acting insulin according to their carbohydrate intake at
meals.63
However,inDM2patients,currenttreatmentalgorithms
include the use of different types of oral hypoglycemic
agents, non-insulin injectable drugs, and insulins.8
Long-acting,intermediate-actingorpremixedinsulinareoptional
regimens used most often by these patients to
supple-mentoraldrugsandendogenousinsulinproduction,butmay
causehypoglycemiaduringfasting.DM2patientsare
insulin-resistantandusuallyrequirehigherdosesofinsulinforthe
samelevelofglycemiccontrol.
Itisoffundamentalimportancetorememberthatbasal
metabolism uses approximately 50% of the daily insulin
produced by an individual, even in the absence of food.
Therefore, the patient should continue to receive a
cer-tainamountofinsulinevenwhenfasting.Thisismandatory
in DM1 patients, as they are insulin-deficient and prone
todevelop diabetic ketoacidosis.Theyneed, therefore, a
continuous exogenous supply of insulin. A common
mis-take is to treat these patients as DM2 patients who
are not prone to ketosis. The latter are susceptible to
develop an HHS,whichmay leadtoseverevolume
deple-tion and neurological complications, although they may
also develop ketoacidosis in response to extreme stress
conditions.8
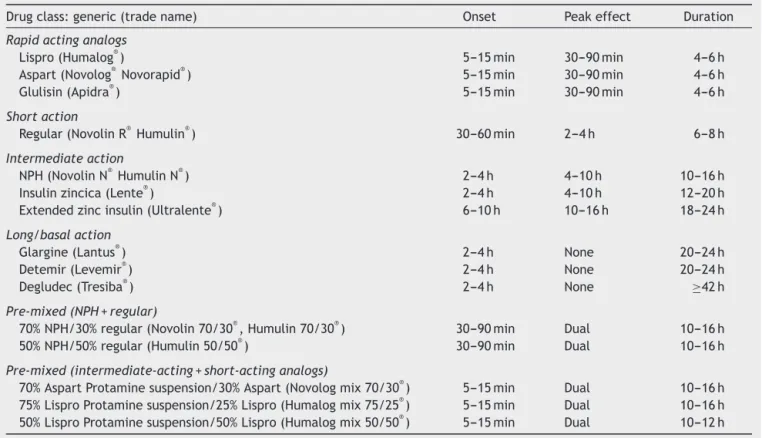
ThetypesofinsulinavailableforDMtreatmentarelisted
inTable4,aswellastheirpharmacokinetics.
Long-actinginsulin analogs, suchasglargine, degludec
ordetemirarecommonlyusedtomaintainglycemiccontrol
betweenmeals. Patientsgenerallydonotpresent withan
Table3 Recommendationsforperioperativeuseoforalandnon-insulininjectableantidiabeticdrugs.
Class(tradename) Previousday Dayofsurgery
Morningsurgery Afternoonsurgery
Biguanides Regularuse,unlesscontraindicateda
Metformin(Glifage®)
Sulphonylureas Regularuse Omitthedoseregardlessofthetime Gliclazide(Diamicron®)
Glibenclamide(Daonil®) Glimepiride(Amaryl®) Glipizide(Glucotrol®
)
Glinides Regularuse Omitthemorningdose Takethemorningdose (pre-meal)ifthepatient hadbreakfast
Nateglinide(Starlix®) Repaglinide(Prandin®
)
Alpha-glucosidaseinhibitors
Acarbose(Glucobay®)
Glitazones Regularuse Regularuse(attentiontopatientsatriskfor cardiaccongestion)
Rosiglitazone(Avandia®
) Pioglitazone(Actos®
)
DPP-4inhibitors Regularuse Regularuse2oromitthedoseonthedayof
surgery(potentialdelayofgastricemptying)8
Sitagliptin(Januvia®) Vildagliptin(Galvus®
) Saxagliptin(Onglyza®
) Alogliptin(Nesina®) Linagliptin(Trayenta®)
GLP1analogs
Exenatide(Byetta®Bydureon®) Liraglutide(Victoza®
)
SGLT-2inhibitors Regularuse Omitdoseonthedayofsurgery.Attentionfor concomitantuseofdiuretics. Dapaglifozina(Forxiga®)
Canaglifozina(Invokana®) Empaglifozina(Jardiance®
)
a Useofradiologicalcontrast,GFR<60mL.min−1,elevatedcreatinineorsignificantriskofARF.2
AdaptedfromRefs.2,8,17.
theyhavenoteaten,asseeninpreandpostoperative
fas-ting.Theadministrationoftheusualdoseoftheseanalogs
on the day prior to surgery and on the day of surgery is
recommended,unlessthereisahistoryofhypoglycemiaor
reduced caloric intake on the eve of the procedure.17,60
Some authors recommend reducing doses by 20---30% the
nightbeforeorinthemorningofsurgery.2,63
Combined treatment with insulin (intermediate-action
or premixed)and oralantidiabeticdrugs maycause
hypo-glycemia during fasting. Regarding intermediate-acting
insulin,suchasneutralprotaminehagedorn(NPH)or
neu-tralprotaminelispro(NPL),givenonthedaybeforesurgery,
thedosegiveninthemorningmaybemaintained;however,
someauthorsrecommenda25%reductioninthedosegiven
atnight,particularlyifthereisahistoryofhypoglycemia.
Onthedayofsurgery,areductionof25---50%inthemorning
doseisrecommended.2,8,17,60
Premixed insulinsarefixed combinations of fast-acting
and intermediate-acting insulins.63 It is not necessary to
change the dose on the day beforesurgery. However, on
the day of surgery, they should be replaced by those of
intermediateandfastaction.Tominimizetheriskof
hypo-glycemiacausedbythefast-actingcomponent,thedoseof
eachtypeofinsulinshouldbegivenindependently.63Asfor
theintermediate-actingcomponent,itisrecommendedto
proportionallyreducethemorningdoseby25---50%.2,17,60,63
Short-acting insulin (regular insulin) or fast-acting
analogs (aspart, glulisine, lispro) are intended to control
meal-induced glycemic changes. It is therefore
recom-mended that the dose remain unchanged the day before
surgery. On the day of surgery, due to the risk of
hypo-glycemia,itisintuitivetoavoid giventheseinsulinswhile
thepatientisfasted.2,8,17,60,63
Inordertodeterminethepreoperativemanagementof
insulin, besides knowing the insulin scheme used by the
patient, it is essential to define the time scheduled for
surgeryandhowmanymealswillbelost.Inpatientswhowill
manip-Table4 Insulintypeandpharmacokinetics.
Drugclass:generic(tradename) Onset Peakeffect Duration
Rapidactinganalogs
Lispro(Humalog®
) 5---15min 30---90min 4---6h
Aspart(Novolog® Novorapid®) 5---15min 30---90min 4---6h
Glulisin(Apidra®) 5---15min 30---90min 4---6h
Shortaction
Regular(NovolinR® Humulin®) 30---60min 2---4h 6---8h
Intermediateaction
NPH(NovolinN®
HumulinN®
) 2---4h 4---10h 10---16h
Insulinzincica(Lente®) 2---4h 4---10h 12---20h
Extendedzincinsulin(Ultralente®) 6---10h 10---16h 18---24h
Long/basalaction
Glargine(Lantus®) 2---4h None 20---24h
Detemir(Levemir®) 2---4h None 20---24h
Degludec(Tresiba®
) 2---4h None ≥42h
Pre-mixed(NPH+regular)
70%NPH/30%regular(Novolin70/30®,Humulin70/30®) 30---90min Dual 10---16h
50%NPH/50%regular(Humulin50/50®) 30---90min Dual 10---16h
Pre-mixed(intermediate-acting+short-actinganalogs)
70%AspartProtaminesuspension/30%Aspart(Novologmix70/30®) 5---15min Dual 10---16h 75%LisproProtaminesuspension/25%Lispro(Humalogmix75/25®
) 5---15min Dual 10---16h
50%LisproProtaminesuspension/50%Lispro(Humalogmix50/50®
) 5---15min Dual 10---12h
AdaptedfromRef.17.
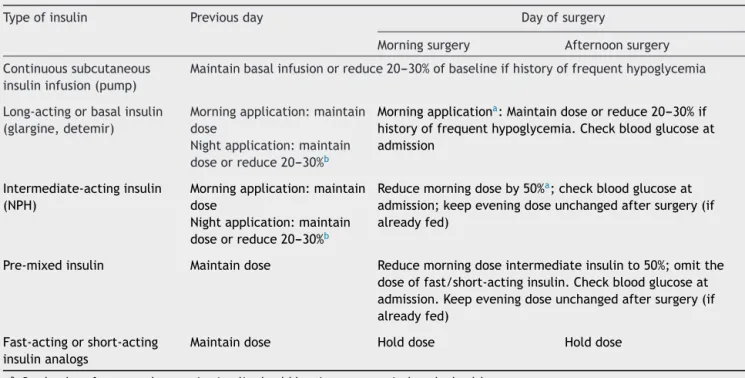
ulatingtheusual dosesof insulinaspreviously mentioned
andsummarizedinTable5.2,17,60
Itisimportanttorememberthatevidenceonthe
peri-operativemanagementofinsulinisstillscarceandthereis
noconsensusamongdifferentguidelines.However,for
sur-geriesrequiringa longperiodof fastingwithloss ofmore
thanonemealor largesurgeries,2,61 the useofa variable
rateintravenousinsulininfusion(VRIII)ismoreindicated.
Variablerateintravenousinsulininfusion(VRIII)
VRIII is preferred for patients who will miss more than
one meal, those with DM1 who underwent surgery and
did not receive basal insulin, those with poorly
con-trolled diabetes (HbA1c>8.5%), and for the majority of
diabetic patients who require emergency surgery. VRIII
shouldbegivenandmonitoredbyqualifiedandexperienced
professionals.2Adequateglucosesupplyshouldbeprovided
toprevent induction of catabolic state, fast ketosis, and
insulin-inducedhypoglycemia.Itisrecommendedthatblood
glucosebemeasuredatleasteveryhour.8
TherearenumerousVRIIIalgorithmspublishedinthe
lit-erature,withinsulinandglucosesolutionsinfusedaloneor
combinedwith glucose, insulin and potassium (GIK)
solu-tion.The injectionregimen of choiceis separate infusion
of insulin andglucose in which glucoseis givenat a rate
of 5---10g.h−1, and the insulin used is the short-acting
insulin (1mL.100−1U insulin in 99mL of 0.9% SS).23 Most
DM1patientsrequireaninfusionrateof1---2units.h−1,while
insulin-resistantDM2patientsmayrequirehigherrates.23
An algorithm commonly followed calculates the initial
rateofinfusionbydividingtheglycemiclevel(inmg.dL−1)
per100andthenroundsuptheresultinunits.h−1(e.g.,a
glucose of 210 divided by 100=2.1units.h−1).In the case
ofhypoglycemia,theinfusionofinsulinmaybedecreased;
however, toavoid ketosis, the temptation to discontinue
insulin infusionshould beavoidedin DM1patients.In such
cases,insulininfusionmaybereducedto0.5units.h−1and
therateofglucoseinfusionincreasedtomaintainglycemic
targets.23
The rate of insulin infusion should be titrated
accord-ingtotheprocedure anddegreeof insulinresistance.For
myocardial revascularization procedures, insulin
require-mentsmayincreaseupto10-fold,especiallyafterrecovery
fromthehypothermiaperiod;athreetofivefoldincrease
intheinitialrateofinsulinisrequired.23
Whichfluidtouseintheperioperativeperiod?
The goal is to avoid solutions with glucose, unless
hypo-glycemia is present.2 The recommended solution for
diabetic patients who do not require VRIII is Hartmann’s
solution(ringerlactate---RL),preferredfor reducing0.9%
sodiumchloride, as it reducesthe risk of hyperchloremic
acidosis.8 In diabetic patients, RL may lead to
hyper-glycemia.Infact,ithasbeenshownthat1LofRLsolution
increases plasma glucose by no more than 1mmol.L−1
(18mg.dL−1).64 Thisdoes notcontraindicateitsusein
Table5 Managementofinsulintherapyforpatientsundergoingshortfastingperiod(uptoamissedmeal).
Typeofinsulin Previousday Dayofsurgery
Morningsurgery Afternoonsurgery
Continuoussubcutaneous insulininfusion(pump)
Maintainbasalinfusionorreduce20---30%ofbaselineifhistoryoffrequenthypoglycemia
Long-actingorbasalinsulin (glargine,detemir)
Morningapplication:maintain dose
Nightapplication:maintain doseorreduce20---30%b
Morningapplicationa:Maintaindoseorreduce20---30%if
historyoffrequenthypoglycemia.Checkbloodglucoseat admission
Intermediate-actinginsulin (NPH)
Morningapplication:maintain dose
Nightapplication:maintain doseorreduce20---30%b
Reducemorningdoseby50%a;checkbloodglucoseat
admission;keepeveningdoseunchangedaftersurgery(if alreadyfed)
Pre-mixedinsulin Maintaindose Reducemorningdoseintermediateinsulinto50%;omitthe doseoffast/short-actinginsulin.Checkbloodglucoseat admission.Keepeveningdoseunchangedaftersurgery(if alreadyfed)
Fast-actingorshort-acting insulinanalogs
Maintaindose Holddose Holddose
a Onthedayofsurgery,themorninginsulinshouldbegivenuponarrivalatthehealthcenter. b Historyofhypoglycemiaduringdawn/morning.
AdaptedfromRefs.2,17,61,64.
ForpatientsreceivingVRIII,thegoalistoprovideglucose
asasubstratetopreventproteolysis,lipolysisand
ketogene-sisandtoimproveintravascularvolumeandmaintainplasma
electrolytesat normalvalues,particularlypotassium.
Flu-idsshould begivenat a rateappropriate tothepatient’s
normalmaintenanceneeds----typically25---50mL.kg−1.day−1
(about83mL.h−1fora70kgpatient).2Toavoidcatabolism,
glucoseshouldbeprovidedatarateofabout5---10g.h−1.23
AdditionalRLsolutionorotherbalancedisotoniccrystalloid
solutionshouldbeusedtorestoreintravascularvolume.2
Perioperativeglycemictargets
There is strong recommendation2,17,60,65 to follow the
implantationoftheWorldHealthOrganization(WHO)
surgi-calsafetytarget,whichestablishesthattheidealin-hospital
glucoserangefornon-criticallyilldiabeticpatientsshould
be 108---180mg.dL−1 (6---10mmol.L−1 in the USA, with the
lower limit of 100mg.dL−1 or 5.6mmol.L−1). Adequate
glycemiccontrolreducesperioperativeinfection,morbidity,
andmortality.1,40
Some authors considerthat arange of72---216mg.dL−1
(4---12mmol.L−1) would be acceptable.60 However, there
are some arguments against using this broad range. The
upperlimit of 216mg.dL−1 (12mmol.L−1) issimilar tothe
invitroconcentration,whichresultsinavarietyofchanges
in endothelial function, increasedcytokine synthesis, and
impaired neutrophil function that increase the risk of
infection.66 The lower limit of 72mg.dL−1 (4mmol.L−1)is
closetothebloodglucosevaluesthatinducesymptomsof
hypoglycemiainsomediabeticpatients.39
Systematicreviewsandmeta-analysishaveattemptedto
identifythebenefitsofintensiveglycemiccontrolindiabetic
patientsundergoingsurgery.Ameta-analysisconcludedthat
moderate glycemic control, defined as a glycemic target
between150and200mg.dL−1(8.3---11.1mmol.L−1),during
orimmediatelyaftersurgery,isassociatedwithareduced
risk of mortality and stroke in DM patients compared to
a liberal glycemic control, defined as a glycemic target
>200mg.dL−1 (>11.1mmol.L−1). The results of this
meta-analysis also showed that there were no differences in
theoutcomesbetweenmoderateandsevereglycemic
con-trol, which was defined as glycemic targets between 90
and 150mg.dL−1 (5.6---8.3mmol.L−1).67 These findings are
supported by a recent Cochrane review, which concluded
thattherewerenodifferencesbetweenintensiveglycemic
control, near-normal glycemia, and conventional control
regardingpostoperativeoutcomes, exceptfor an increase
in hypoglycemic events that occurred in patients treated
withintensivecontrol.68
Chronically elevated glycemic levels should not be
acutely reduced or normalized due to the potential for
hypoglycemiaandbecausesignificantfluctuationsinblood
glucose levels may increase perioperative morbidity and
mortality.5,42
Whentopostponesurgery?
In general, surgery should be postponed in patients with
significant complications of hyperglycemia, such as
dehy-dration,ketoacidosisorHHS.17,42 However,surgerymaybe
indicated for patients with preoperative hyperglycemia,
inrecentmonths.17Dependingonindividualcircumstances,
anupperlimitofHbA1cbetween8%and9%isacceptable.8
ThelatestBritishguidelinesrecommendthatsurgeryshould
bepostponed inthepresenceof HbA1cabove8.5%(mean
of200mg.dL−1) in ordertoimprove glycemic controland
reduce complications.2 For the Australian Society of
Dia-betes,HbA1cvalueshouldbeabove9%(meanbloodglucose
of215mg.dL−1)forpostponingsurgery.61
Onadailybasis,theserecommendationsmaybepoorly
practical ifwe consider that reducingHbA1c levels could
takeweeks/months60 andthatin certaincasesitmaynot
bepossibletoimproveglycemiccontrolinatimelymanner,
particularlyifthereasonforsurgery,suchaschronic
infec-tion,contributetoworseglycemiccontrolorifthesurgeryis
urgent.Inthesecircumstances,itmaybeacceptableto
con-tinuesurgeryafterexplainingtothepatienttheincreased
risks.2 In thesepatients, HbA1cwould bea usefultool to
enhance perioperative diabetic therapy in an attempt to
reducecomplications.8
Conclusion
DMpatientsareatincreasedriskfordeveloping
periopera-tivecomplications.Metabolicstresscausedbythesurgical
procedureleads toan increasein thedemandfor insulin,
whichmaycausedecompensationandhyperglycemia.Prior
tosurgery,athoroughassessmentofthecharacteristicsof
thesepatients,includingtreatmentforDM,iscritical.
Peri-operativemanagement,particularlydrugtreatment,should
beadjustedaccordingtothepatient’sroutineandsurgical
procedurecharacteristics(typeandduration).Ifthefasting
periodis limitedtoamissedmeal, thechoice isto
main-tainor modify thewayin whichthemedication isusually
used.Iflongerperiodsof fastingarepredicted,avariable
rateintravenousinsulininfusion(VRIII)shouldbeusedand
aspecialistassessmentrequested.Evidenceonthe
periop-erativemanagementofmedicationsisstillscarceandthere
is noagreement between the differentguidelines,
there-foremoreclinicaltrialsareneededtodetermine thebest
planningforthetreatmentofthesepatients.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.FrischA, ChandraP,SmileyD,et al.Prevalence and clinical outcomeofhyperglycemiaintheperioperativeperiodin non-cardiacsurgery.DiabetesCare.2010;33:1783---8.
2.BarkerP,CreaseyPE,DhatariyaK,etal.Peri-operative manage-mentofthesurgical patientwithdiabetes2015:Association of Anaesthetists of Great Britain and Ireland. Anaesthesia. 2015;70:1427---40.
3.Stumvall M, Goldstein BJ, van Haeften TW. Type 2 dia-betes: principles of pathogenesis and therapy. Lancet. 2005;365:1333---46.
4.Standardsofmedicalcareindiabetes---2015.Classificationand diagnosisofdiabetes.DiabetesCare.2015;38Suppl.1:S8---16.
5.SebranekJJ,LugliAK, CoursinDB. Glycaemic control inthe perioperativeperiod.BrJAnaesth.2013;111Suppl.1:i18---34.
6.Larkin ME, Barnie A, Braffett BH, et al. Musculoskele-tal complications in type 1 diabetes. Diabetes Care. 2014;37:1863---9.
7.WallR.Endocrinedisease.In:HinesRL,MarschallKE,editors. Stoelting’sanesthesiaandco-existingdisease.6thed. Philadel-phia:Elsevier;2012.p.376---84.
8.Soldevila B, Lucas AM, Zavala R, et al. Perioperative man-agement of thediabetic patient. In: Stuart-Smith K, editor. Perioperativemedicine--- currentcontroversies.Switzerland: Springer;2016.p.165---92.
9.Perazella MA, Tray K. Selective cyclooxygenase-2 inhibitors: apatternofnephrotoxicitysimilartotraditionalnonsteroidal anti-inflammatorydrugs.AmJMed.2001;111:64.
10.MoitraVK,MeilerSE.Thediabeticsurgicalpatient.CurrOpin Anaesthesiol.2006;19:339---45.
11.SelvinE,CoreshJ, ShaharE,et al.Glycaemia(haemoglobin A1c) and incident ischaemic stroke: the Atherosclerosis Risk in Communities (ARIC) Study. Lancet Neurol. 2005;4: 821---6.
12.KadoiY,HinoharaH,KunimotoF,etal.Diabeticpatientshavean impairedcerebralvasodilatoryresponsetohypercapniaunder propfolanesthesia.Stroke.2003;34:2399---403.
13.BeckmanJA,CreagerMA,LibbyP.Diabetesandatherosclerosis. JAMA.2002;287:2570---81.
14.HaffnerSM,LehtoS,RonnemaaT,etal.Mortalityfromcoronary arterydiseaseinsubjectswithtype2diabetesandin nondia-beticsubjectswithandwithoutpriormyocardialinfarction.N EnglJMed.1998;339:229---34.
15.ExecutivesummaryoftheThirdReportoftheNational Choles-terol Education Program (NCEP) Expert Panel on Detection. Evaluationand treatmentof highbloodcholesterolinadults (AdultTreatmentPanelIII).JAMA.2001;285:2486---97.
16.Fleisher LA, Fleischmann KE, Auerbach AD, et al. 2014 ACC/AHAguidelineonperioperativecardiovascularevaluation and managementof patientsundergoingnoncardiacsurgery: executivesummary:areportoftheAmericanCollegeof Car-diology/American Heart Association Task Force on Practice Guidelines.Circulation.2014;130:2215---45.
17.Joshi GP, Chung F, Vann MA, et al. Society for ambulatory anaesthesiaconsensusstatementonperioperativeblood glu-cosemanagementindiabeticpatientsundergoingambulatory surgery.AnesthAnalg.2010;111:1378---87.
18.Loh-Trivedi M, Croley WC. Perioperative management of
thediabeticpatient;2015.http://emedicine.medscape.com/ article/284451-overview#a3[accessed27.08.16].
19.AbdelmalakB,AbdelmalakJB,KnittelJ,etal.Theprevalence ofundiagnosed diabetesin non-cardiac surgery patients, an observationalstudy.CanJAnaesth.2010;57:1058---64.
20.SheehyAM,BencaJ,GlinbergSL,etal.Preoperative‘NPO’asan opportunityfordiabetesscreening.JHospMed.2012;7:611---66.
21.LauruschkatAH,ArnrichB,AlbertAA,etal.Prevalenceandrisks ofundiagnoseddiabetesmellitusinpatientsundergoing coro-naryarterybypassgrafting.Circulation.2005;112:2397---402.
22.KadoiY.Anaestheticconsiderationsindiabeticpatients.PartI: preoperativeconsiderationsofpatientswithdiabetesmellitus. JAnesth.2010;24:739---47.
23.Khan NA, Ghali WA, Cagliero E. Perioperative management of blood glucose in adults with diabetes mellitus; 2016
www.UpToDate.com
24.AmericanDiabetes Association. Standardsof medicalcare in diabetes---2015.DiabetesCare.2015;38Suppl.1:S33---40.
26.Nathan DM, Kuenen J, Borg R, et al. Translating the A1C assayinto estimatedaverage glucosevalues. Diabetes Care. 2008;31:1473---8.
27.WalidMS,NewmanBF,YelvertonJC,etal.Prevalenceof pre-viouslyunknownelevationofglycosylatedhemoglobininspine surgerypatientsandimpactonlengthofstayandtotalcost.J HospMed.2010;5:10---4.
28.O’Sullivan CJ, Hynes N, Mahendran B, et al. Haemoglobin A1c (HbA1C)in non-diabetic and diabetic vascular patients. IsHbA1Canindependentriskfactorandpredictorofadverse outcome?EurJVascEndovascSurg.2006;32:188---97.
29.GustafssonUO,ThorellA,SoopM,etal.Haemoglobin A1cas apredictorofpostoperativehyperglycaemiaandcomplications aftermajorcolorectalsurgery.BrJSurg.2009;96:1358---64.
30.HalkosME, LattoufOM,PuskasJD, etal.Elevated preopera-tivehemoglobinA1clevelisassociatedwithreducedlong-term survivalaftercoronaryarterybypasssurgery.AnnThoracSurg. 2008;86:1431---7.
31.AlseriusT,AndersonRE,HammarN,etal.Elevatedglycosylated haemoglobin(HbA1c)isariskmarkerincoronaryarterybypass surgery.ScandCardiovascJ.2008;42:392---8.
32.KreutzigerJ,SchlaepferJ,WenzelV,etal.Theroleofadmission bloodglucoseinoutcomepredictionofsurvivingpatientswith multipleinjuries.JTrauma.2009;67:704---8.
33.Vilar-Compte D,Alvarezde Iturbe I,Martin-Onraet A, etal. Hyperglycemia as a risk factor for surgical site infections in patients undergoing mastectomy. Am J Infect Control. 2008;36:192---8.
34.ShibuyaN,HumphersJM,FluhmanBL,etal.Factorsassociated withnonunion,delayedunion,andmalunioninfootandankle surgeryindiabeticpatients.JFootAnkleSurg.2013;52:207---11.
35.Chuang SC, Lee KT, Chang WT, et al. Risk factors for woundinfectionaftercholecystectomy.JFormosMedAssoc. 2004;103:607---12.
36.AmbiruS, Kato A, KimuraF,et al. Poorpostoperativeblood glucosecontrolincreasessurgicalsiteinfectionsaftersurgery forhepato-biliary-pancreaticcancer:aprospectivestudyina high-volumeinstituteinJapan.JHospInfect.2008;68:230---3.
37.UnderwoodP,AskariR,HurwitzS,etal.PreoperativeA1Cand clinicaloutcomesinpatientswithdiabetesundergoingmajor noncardiacsurgicalprocedures.DiabetesCare.2014;37:611---6.
38.NICE Guideline. Preoperative tests (update): routine pre-operative tests for elective surgery. London: National Institute for Health and Care Excellence (UK); 2016, nice.org.uk/guidance/ng45.
39.AldamP,LevyN,HallGM.Perioperativemanagementofdiabetic patients:newcontroversies.BrJAnaesth.2014;113:906---9.
40.KwonS, ThompsonR, DellingerP,et al. Importanceof peri-operativeglycemiccontrol ingeneralsurgery: areportfrom thesurgicalcareandoutcomesassessmentprogram.AnnSurg. 2013;257:8---14.
41.BockM,JohanssonT,FritschG,etal.Theimpactof preoper-ativetestingforbloodglucoseconcentrationandhaemoglobin A1conmortality,changesinmanagementandcomplicationsin noncardiacelectivesurgery:asystematicreview.EurJ Anaes-thesiol.2015;32:152---9.
42.AkhtarS,BarashPG,InzucchiSE.Scientificprinciplesand clini-calimplicationsofperioperativeglucoseregulationandcontrol. AnesthAnalg.2010;110:478---97.
43.BagryHS, Raghavendran S, Carli F. Metabolic syndrome and insulinresistance: perioperative considerations. Anesthesiol-ogy.2008;108:506---23.
44.McAnulty GR, Robertshaw HJ, Hall GM. Anaesthetic man-agement of patients with diabetes mellitus. Br J Anaesth. 2000;85:80---90.
45.Fragen RJ, Shanks CA, Molteni A, et al. Effects of etomi-dateonhormonalresponsestosurgicalstress.Anesthesiology. 1984;61:652---6.
46.Belhoula M, Ciébiéra JP, De La Chapelle A, et al. Cloni-dine premedication improves metabolic control in type 2 diabetic patients during ophthalmic surgery. Br J Anaesth. 2003;90:434---9.
47.LattermannRT,SchrickerU,WachterM,etal.Understanding themechanismsbywhichisofluranemodifiesthehyperglycemic responsetosurgery.AnesthAnalg.2001;93:121---7.
48.HalterJB,PflugAE.Effectofsympatheticblockadebyspinal anaesthesiaonpancreaticisletfunctioninman.AmJPhysiol. 1980;239:150---5.
49.DonatelliF,VavassoriA,BonfantiS.Epiduralanaesthesiaand analgesiadecreasethepostoperativeincidenceofinsulin resis-tance in preoperative insulin-resistant subjects only. Anesth Analg.2007;104:1587---93.
50.OstermanAL.Thedoublecrushsyndrome.OrthopClinNAm. 1988;19:147---55.
51.KalichmanMW,CalcuttNA.Localanesthetic-induced conduc-tionblockandnervefiberinjuryinstreptozotocin-diabeticrats. Anesthesiology.1992;77:941---7.
52.Willams BA. Toward a paradigm shift for the clinical care of diabetic patients requiring perineural analgesia: strate-giesfor using the diabeticratmodel. RegAnesth Pain Med. 2010;35:329---32.
53.GebhardRE,NielsenKC,PietrobonR,etal.Diabetesmellitus, independentofbodymassindex,isassociatedwitha‘‘higher success’’rate forsupraclavicular brachialplexusblocks.Reg AnesthPainMed.2009;34:404---7.
54.Sites BD, Gallagher J, SparksM. Ultrasound-guidedpopliteal blockdemonstratesanatypicalmotorresponsetonerve stimu-lationin2patientswithdiabetesmellitus.RegAnesthPainMed. 2003;28:479---82.
55.NealJM,BarringtonMJ,BrullR,etal.ThesecondASRApractice advisoryonneurologiccomplicationsassociatedwithregional anesthesia and painmedicine executive summary 2015. Reg AnesthPainMed.2015;40:401---30.
56.DuncanAI,KochCG,XuM,etal.Recentmetforminingestion doesnotincreasein-hospitalmorbidityormortalityafter car-diacsurgery.AnesthAnalg.2007;104:42---50.
57.TheRoyalCollegeofRadiologists.Standardsfor intravascular contrast agent administration to adult patients. 2nd ed. London:TheRoyalCollegeofRadiologists;2010.Availablefrom
https://www.rcr.ac.uk/docs/radiology/pdf/BFCR(10)4Stand contrast.pdf[accessed05.06.16].
58.Standards of medical care in diabetes --- 2015. Approach to glycemic control. Diabetes Care. 2015;38 Suppl. 1: S41---8.
59.Sudhakaran S, Surani SR. Guidelines for perioperative man-agement of the diabetic patient. Surg Res Pract. 2015; 2015:284063.
60.DhatariyaK, LevyN,KilvertA, etal.NHSdiabetesguideline for theperioperative management oftheadultpatient with diabetes.DiabetMed.2012;29:420---33.
61.Australian Diabetes Society. Peri-operative diabetes man-agement guidelines; 2012. https://diabetessociety.com.au/ documents/PerioperativeDiabetesManagementGuidelinesFINAL CleanJuly2012.pdf[accessed10.06.16].
62.FerreiraVA.Avanc¸osfarmacológicosnotratamentododiabetes tipo2.BrazJSurgClinRes(BJSCR).2014;8:72---8.
63.Vann MA. Management of diabetes medications for patients undergoing ambulatory surgery. Anesthesiol Clin. 2014;32:329---39.
64.Simpson AK, Levy N, Hall GM. Peri-operative i.v. fluids in diabetic patients --- don’t forget the salt. Anaesthesia. 2008;63:1043---5.
66.Langouche L, Vanhorebeek I, Vlasselaers D, et al. Inten-siveinsulintherapy protectsthe endotheliumofcritically ill patients.JClinInvest.2005;115:2277---86.
67.SathyaB,DavisR,TaveiraT,etal.Intensityofperi-operative glycaemic control and postoperative outcomes in patients
with diabetes: a meta-analysis. Diabetes Res Clin Pract. 2013;102:8---15.